Cerebral Palsy
Dr. Mansour Alqurashi
Learning Objectives
- Definition
- Etiology/Risk Factors
- Signs and symptoms (types of CP)
- Diagnosis
- Conditions Associated with CP and complications
- Treatment
- Follow-up and prognosis
Definition
Cerebral Palsy (CP)
- Cerebral: Brain
- Palsy: Disorder of movement & posture
CP is a group of permanent disorders of movement and posture causing activity limitations that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain.
The motor disorders of CP are often accompanied by disturbances of sensation, cognition, communication, perception, behaviour, and seizure disorder.
The brain lesions that cause CP occur from the fetal or neonatal period to up to age 3 years.
Some authorities advocate not making a definitive diagnosis in selected cases until age 5 years or later. This approach allows the clinical picture to be clear and potentially allows exclusion of progressive diseases. As the brain continues to develop postnatally, abnormalities of motor tone or movement in the first several weeks or months after birth may gradually improve over the first year of life (or even later).
CP is historically considered a static encephalopathy, but some of the neurologic features of CP—such as movement disorders and orthopedic complications including scoliosis and hip dislocations—can change or progress over time.
Epidemiology
In developed countries, the overall estimated prevalence of CP is 2–2.5 cases per 1000 live births. In Saudi Arabia, it is approximately 4 per 1000.
The prevalence of CP among preterm infants is extensively higher. Z - more prone for complications
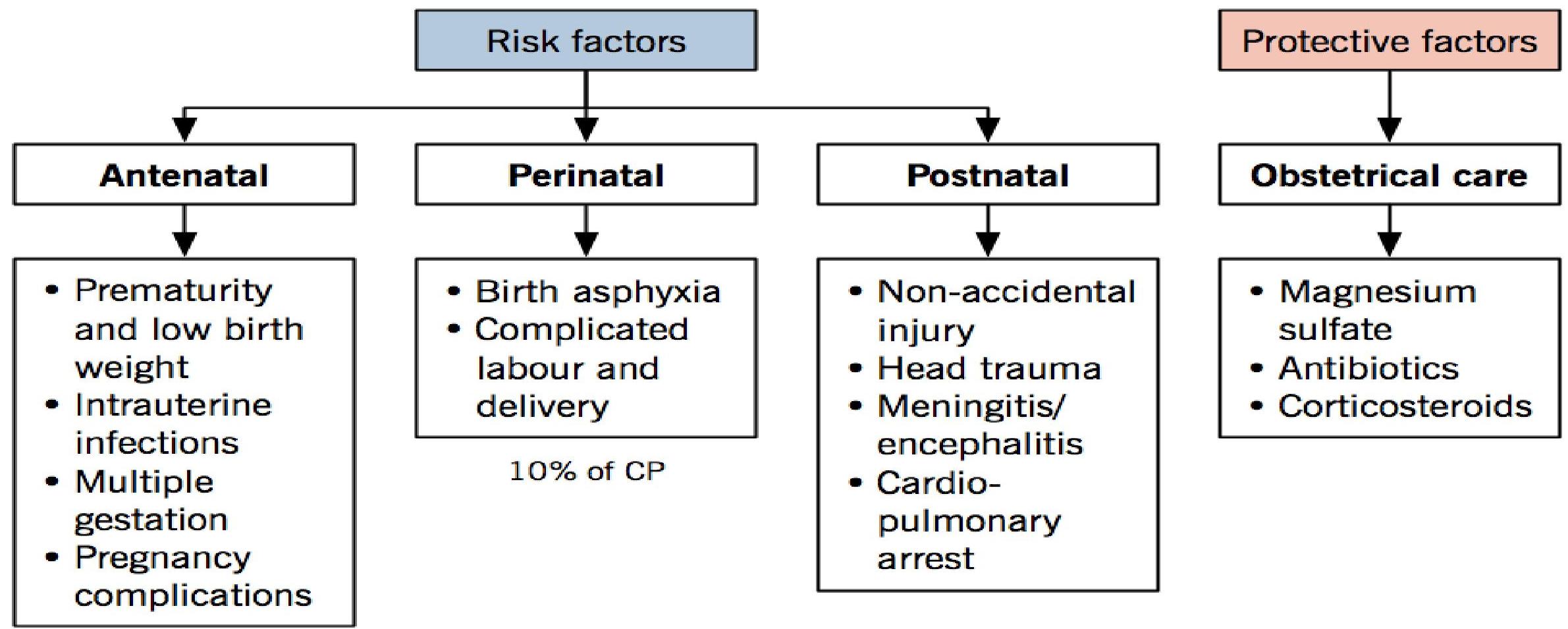
Etiology and Risk Factors
Risk factors can be divided by time period into antenatal, perinatal, and postnatal factors. The majority of the risk occurs in the antenatal period.
Prematurity is a significant risk factor, predisposing to the development of periventricular leukomalacia (PVL). Prudent obstetrical care, with management of preeclampsia (magnesium), infections (antibiotics), and preterm labour (corticosteroids), can help reduce the risk of CP.
 70-80% of CP cases are due to prenatal causes.
70-80% of CP cases are due to prenatal causes.
Prenatal Risk Factors (70-80%)
Maternal, prenatal, and gestational factors
The following maternal and prenatal risk factors statistically correlate with CP:
- Previous pregnancy loss or loss of newborn
- Maternal mental retardation
- Maternal thyroid disorder (especially iodine deficiency), treatment with thyroid hormone
- Maternal seizure disorder
- History of delivering a child weighing less than 2000 g
- History of delivering a child with a motor deficit, mental retardation, or a sensory deficit
- Polyhydramnios
- Maternal severe proteinuria or high blood pressure
- Maternal methyl mercury exposure, estrogen, progesterone
- Congenital malformations in the fetus
- Bleeding in third trimester
- Intrauterine growth retardation (IUGR)
- Multiple gestation
Perinatal Risk Factors (10%)
The following perinatal factors are associated with an increased risk of CP:
- Prematurity
- Chorioamnionitis
- Nonvertex and face presentation of the fetus
- Birth asphyxia
Birth Asphyxia (10%)
- Even when birth asphyxia is thought to be clearly associated with cerebral palsy, abnormal prenatal factors (e.g., IUGR, brain malformations) may have contributed to perinatal fetal distress.
- Cases of CP attributed to birth asphyxia must document clear evidence of acidosis, moderate to severe neonatal encephalopathy, restriction to spastic quadriplegia, dyskinetic or mixed types of CP, and exclusion of other etiologies.
- Additionally, an intrapartum event must be suggested by a sentinel event, fetal heart rate changes, Apgar score less than 4 at 5 minutes, organ system damage related to tissue hypoxia, and early imaging abnormalities.
- Note: Although Apgar scores provide a method for documenting cardiopulmonary and neuromotor status in the minutes following birth, low scores alone cannot be used as an indicator of birth asphyxia. Such scores may reflect circumstances unrelated to birth asphyxia, such as infections and other preexisting prenatal conditions.
Postnatal Risk Factors (10%)
The following postnatal factors may contribute to CP:
- Infections (e.g., meningitis, encephalitis)
- Intracranial hemorrhage (e.g., due to prematurity, vascular malformations, or trauma)
- Periventricular leukomalacia (PVL) in premature infants
- Hypoxia-ischemia (e.g., from meconium aspiration)
- Persistent fetal circulation or persistent pulmonary hypertension of the newborn
- Kernicterus
Possible Causes by Clinical Type
Spastic Hemiplegic (25%)
- Unilateral lesions of the brain: Cerebral hypoperfusion in middle cerebral artery; hemi-brain atrophy and posthemorrhagic porencephaly.
- Premature infants: Asymmetric PVL.
- Etiology: Stroke, IVH.
Spastic Diplegic (35%)
- Premature infants: Often results from parenchymal-intraventricular hemorrhage or periventricular leukomalacia (PVL).
- Term infants: No risk factors may be identifiable, or the etiology might be multifactorial.
Spastic Quadriplegic (20%)
- Origin: 50% prenatal, 30% perinatal, 20% postnatal.
- Pathology: Associated with multiple cystic lesions in white matter, diffuse cortical atrophy, and hydrocephalus.
- Term infants: Structural brain abnormalities or cerebral hypoperfusion in major cerebral artery end zone distribution.
- Preterm infants: May have PVL.
- Evidence of perinatal asphyxia.
Dyskinetic / Extrapyramidal (15%)
- Kernicterus, or acute neonatal bilirubin encephalopathy
- Hypoxic ischemic injury
- Prematurity
- Metabolic or neurodegenerative disorders must be considered in the absence of the above causes.
Classification
CP can be classified by Topography (Anatomy), Physiology (Motor Type), Etiology, and Function.
1. Topographic Classification (Anatomic)
-
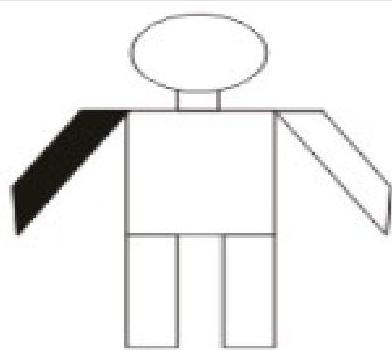
Monoplegia: Only one limb is affected, usually an arm.
-
Hemiplegia: One side of the body is affected. The arm is usually more involved than the leg.
-
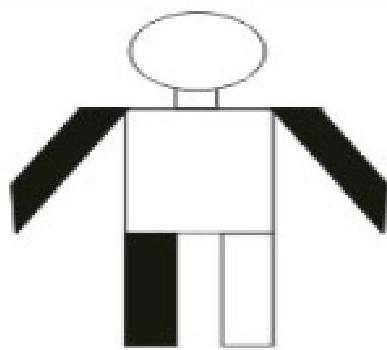
Diplegia: All four limbs are involved. Both legs are more severely affected than the arms.
-
Triplegia: Three limbs are involved, usually both arms and a leg.
 (Note: Images for triplegia may overlap with others in source material)
(Note: Images for triplegia may overlap with others in source material) -
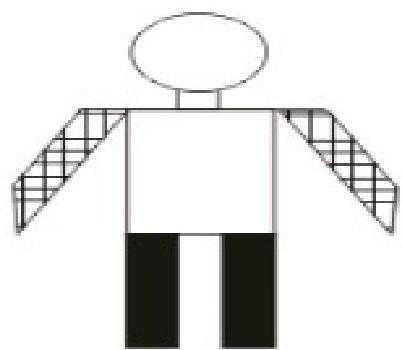
Quadriplegia: All four limbs are involved.
-
Paraplegia: Both lower limbs are affected.
-
Double Hemiplegia: Arms are more involved than legs.
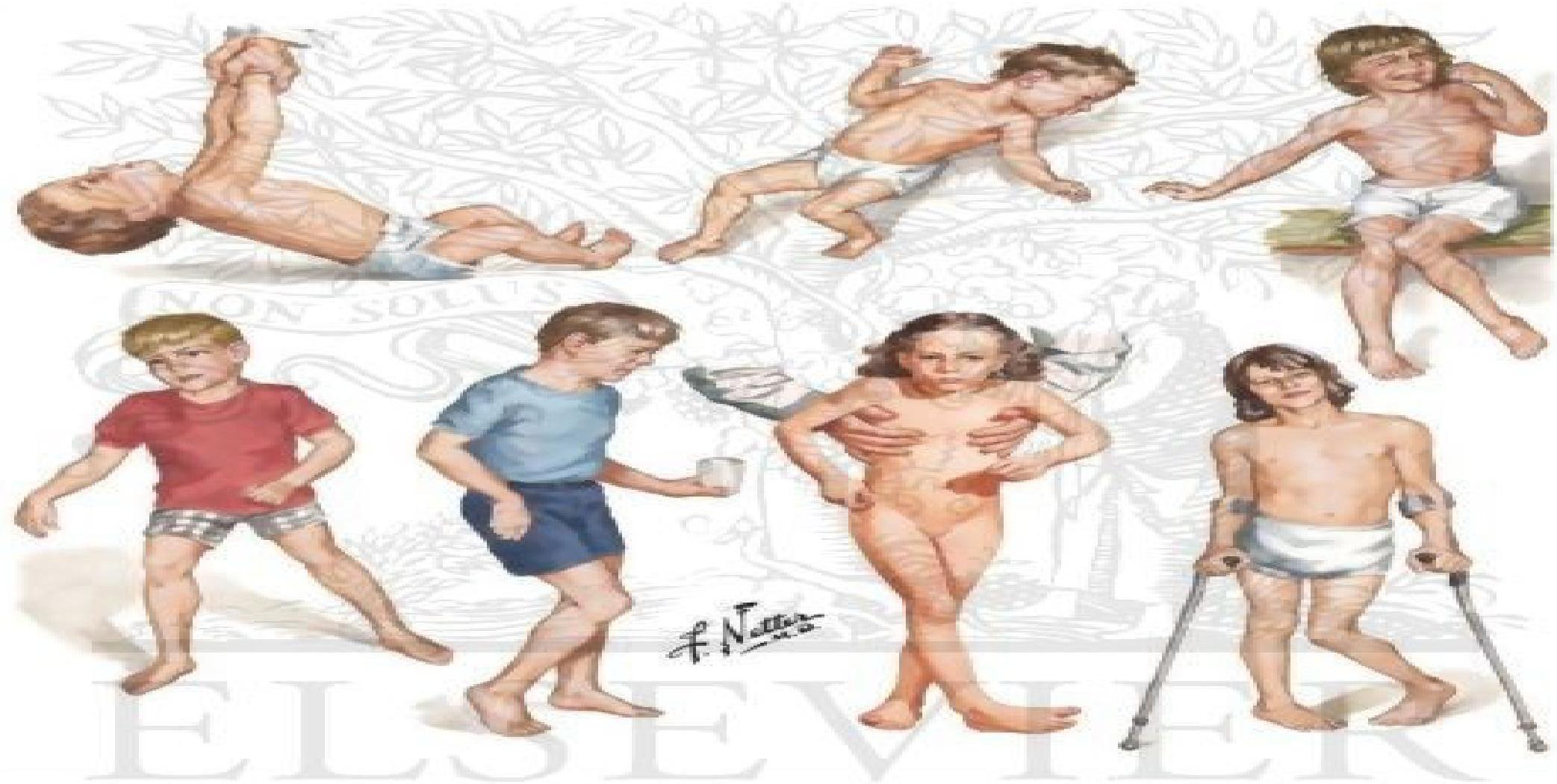
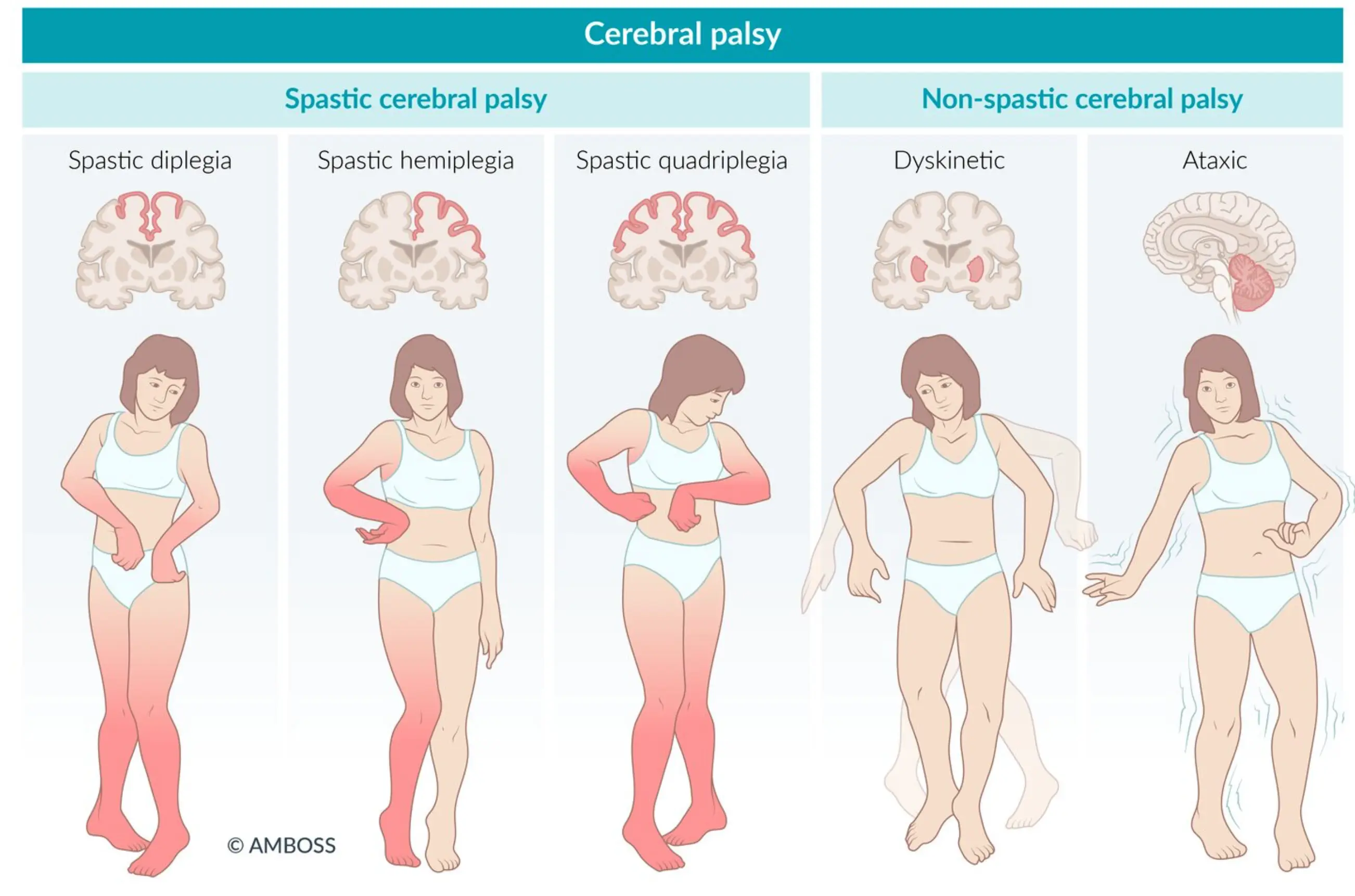
2. Physiological Classification (Motor Disability Type)
-
Spastic (Pyramidal): Tense, contracted muscles. Most common type (75%).
- Signs: Hypertonia, hyperreflexia, clonus, extensor Babinski response, persistent primitive reflexes, overflow reflexes (crossed adductor).
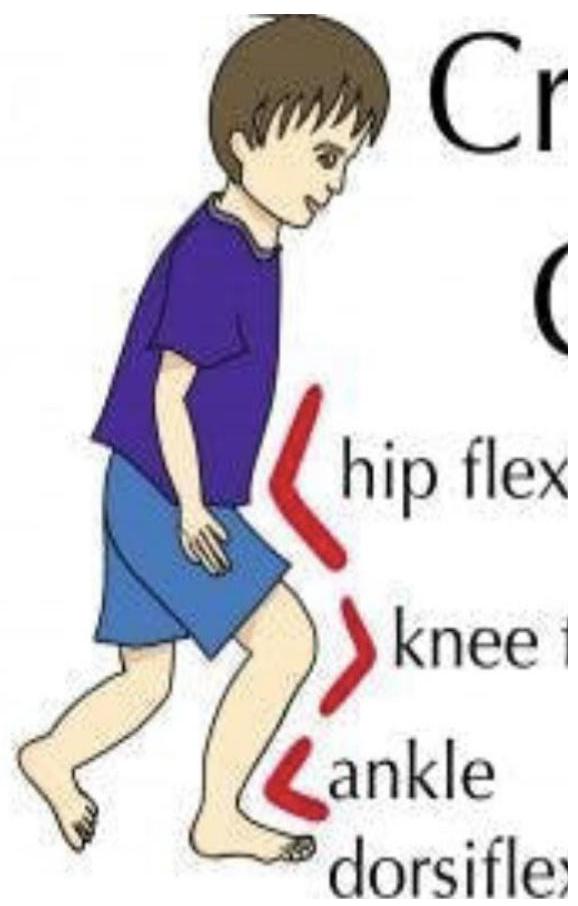
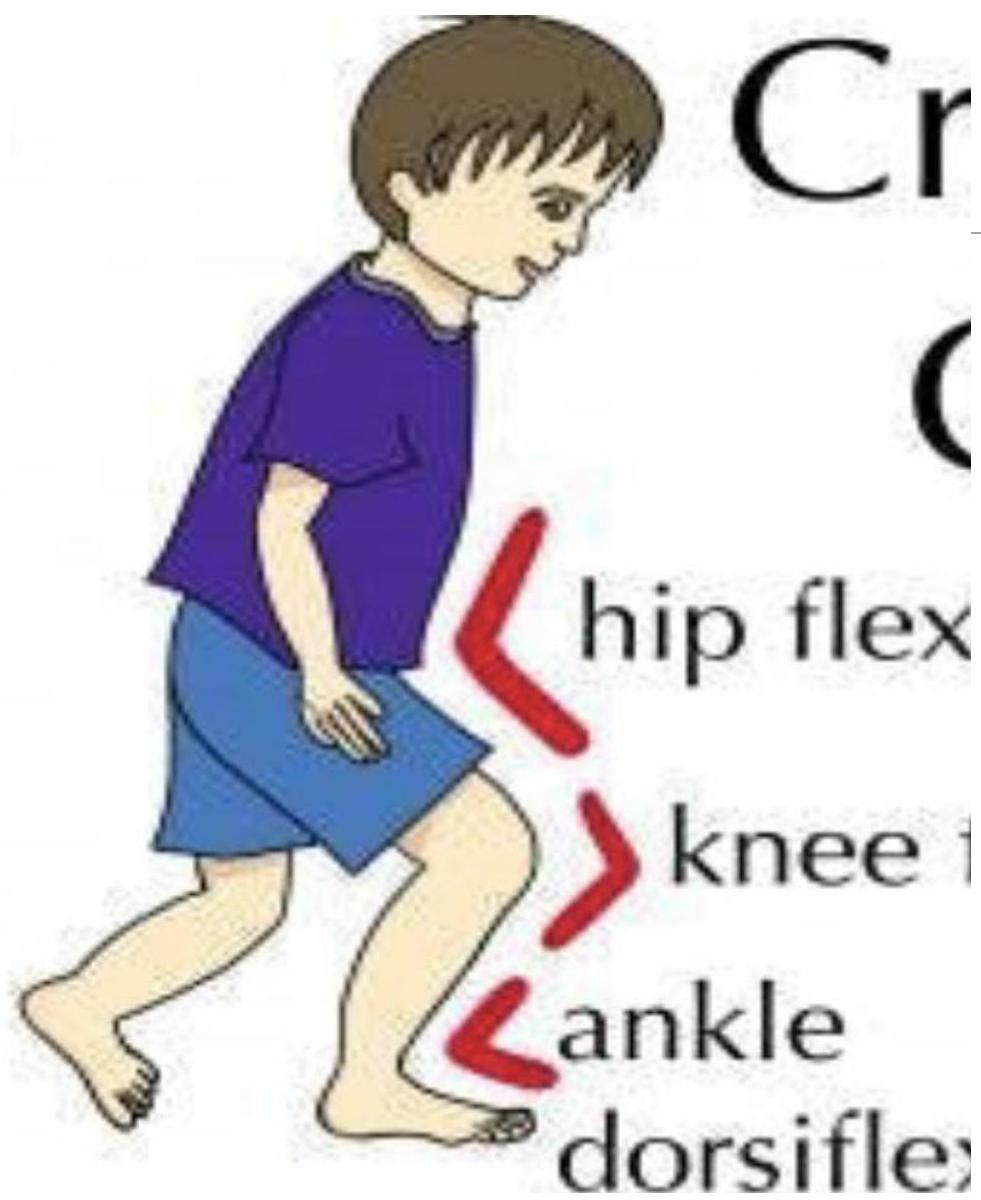
- Postures: Tendency to keep elbow flexed; hips flexed and adducted with knees flexed and in valgus; ankles in equinus (toe walking).
-
Dyskinetic (Extrapyramidal):
- Athetoid: Constant, slow, writhing, involuntary movements (distal extremities).
- Chorea: Abrupt, irregular, jerky movements.
- Choreoathetosis: Combination of athetosis and chorea.
- Dystonia: Slow, rhythmic movements with increased tone and abnormal postures.
-
Ataxic: Poor sense of balance, often causing falls and stumbles.
-
Mixed: Combination of types (e.g., Spastic + Dyskinetic).
-
Atonic: Hypotonia.
Motor Syndromes Overview (Nelson Textbook of Pediatrics)
- Spastic Hemiplegia (25%):
- Gait: Circumductive (swinging leg outward).
- Hand: Early handedness, decreased use of affected side.
- Spastic Diplegia (35%):
- Gait: Scissor gait (legs adduct past midline), commando crawl (drags legs).
- Pathology: Associated with PVL.
- Spastic Quadriplegia (20%):
- Most severe form.
- High likelihood of seizures, cognitive impairment, and swallowing difficulties.
- Athetoid/Extrapyramidal (15%):
- Involuntary contraction of all muscle groups.
- Difficulty with speech and swallowing.
- Normal intelligence (78%) and low risk of seizures.
3. Etiologic Classification
- Prenatal: Infection, Anoxia, Toxic, Vascular, Rh disease, Genetic, Congenital malformation.
- Natal: Anoxia, Traumatic delivery, Metabolic.
- Postnatal: Trauma, Infection, Toxic.
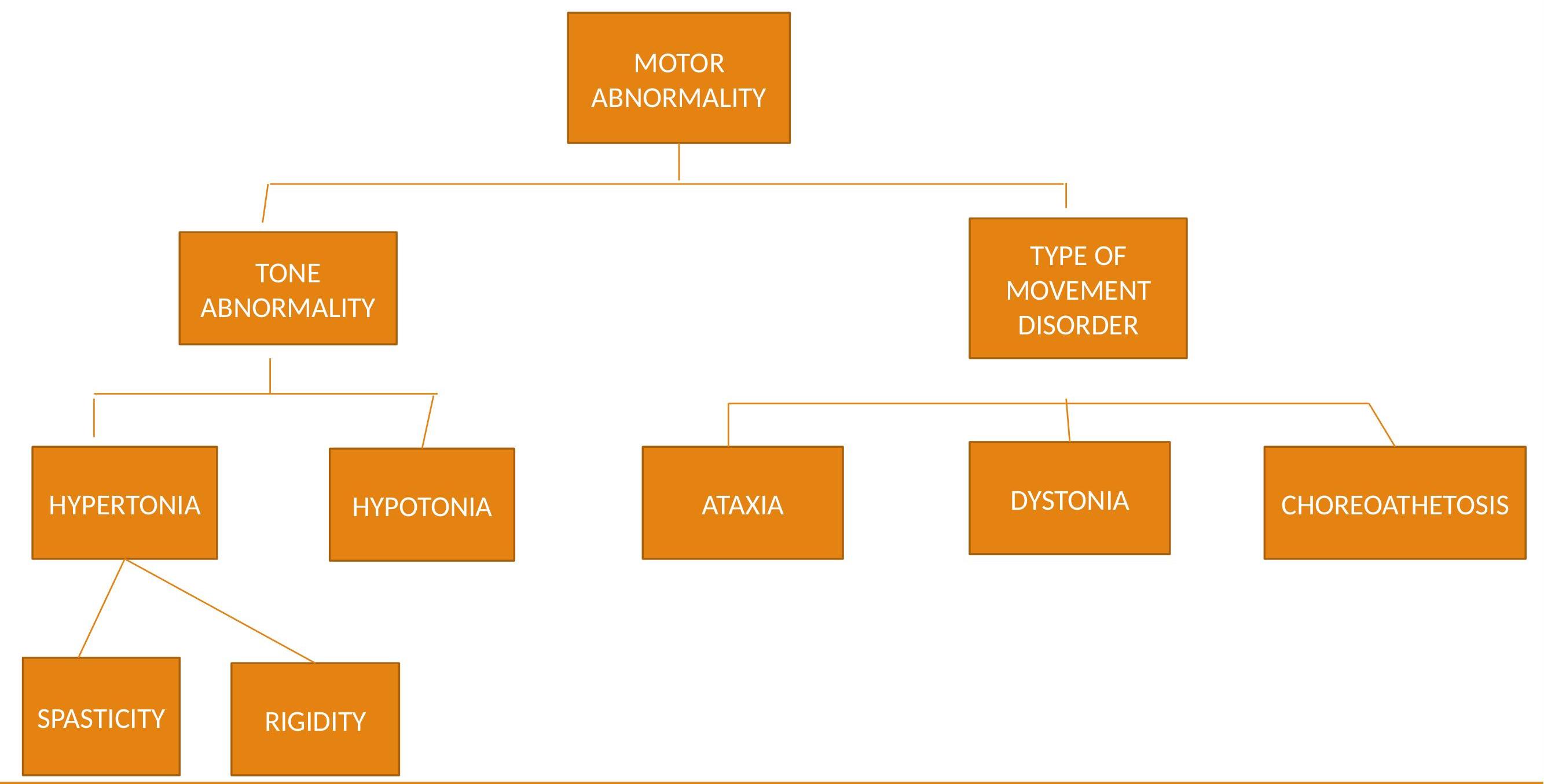
Classification Tree (SCPE)
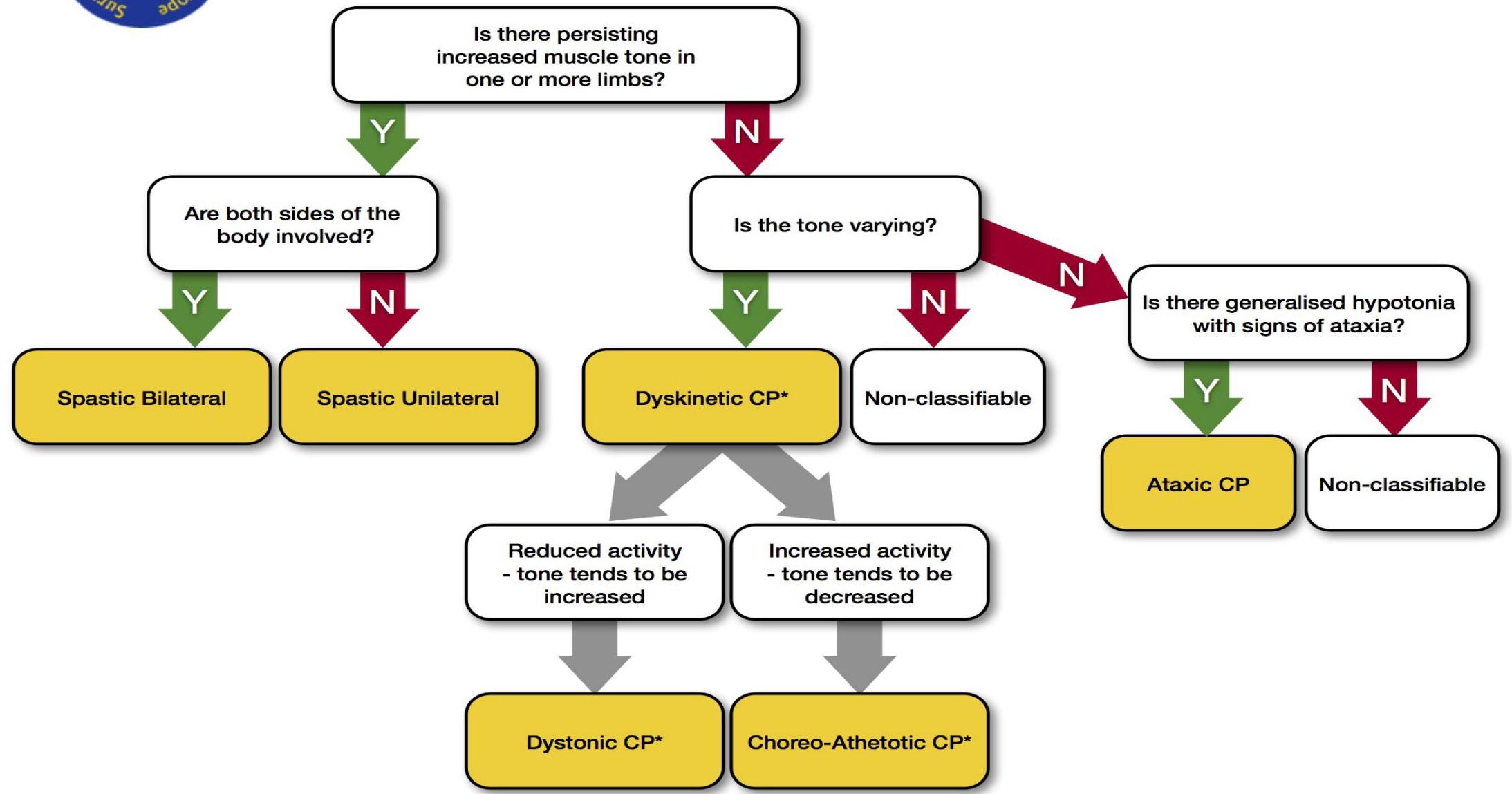 Source: SCPE Collaborative Group. Surveillance of cerebral palsy in Europe. Dev Med Child Neurol. 2000.
Source: SCPE Collaborative Group. Surveillance of cerebral palsy in Europe. Dev Med Child Neurol. 2000.
4. Functional Classification (GMFCS)
Gross Motor Function Classification System (GMFCS)
GMFCS Levels (Visual Guide)
Level I: Able to walk without restrictions
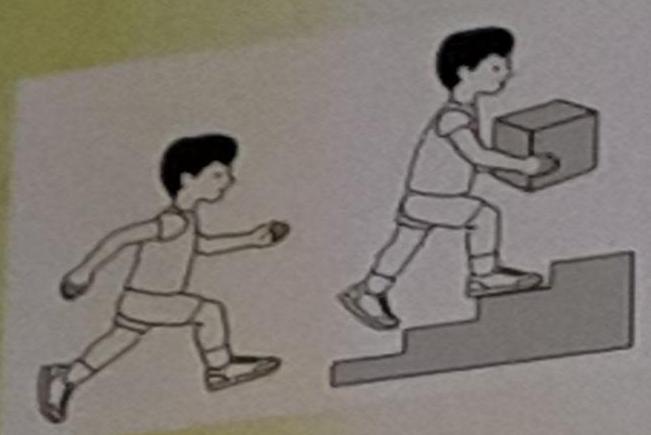 Children walk at home, school, outdoors, and in the community. Climb stairs without railing. Perform running and jumping, but speed/balance limited.
Children walk at home, school, outdoors, and in the community. Climb stairs without railing. Perform running and jumping, but speed/balance limited.
Level II: Able to walk without devices
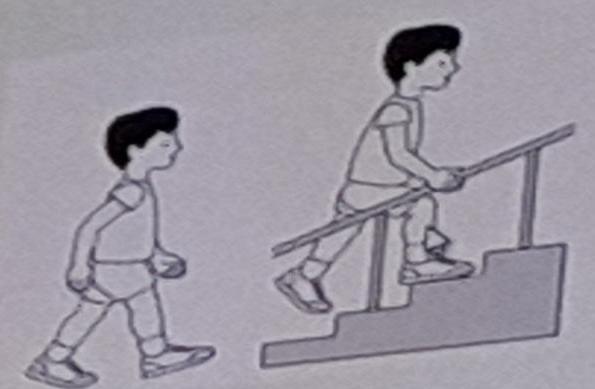 Walk in most settings; climb stairs holding railing. Difficulty on uneven terrain/crowds. Minimal ability to run/jump.
Walk in most settings; climb stairs holding railing. Difficulty on uneven terrain/crowds. Minimal ability to run/jump.
Level III: Able to walk with mobility devices
 Walk with hand-held mobility device indoors. Wheeled mobility for long distances.
Walk with hand-held mobility device indoors. Wheeled mobility for long distances.
Level IV: Self mobility with limitations (power mobility)
 Powered mobility or physical assistance in most settings. Manual wheelchair for community transport.
Powered mobility or physical assistance in most settings. Manual wheelchair for community transport.
Level V: Self mobility severely limited
 Transported in manual wheelchair. Limited ability to maintain antigravity head/trunk postures.
Transported in manual wheelchair. Limited ability to maintain antigravity head/trunk postures.
GMFCS Descriptions by Age
Before 2nd Birthday
| Level | Description |
|---|---|
| I | Infants move in and out of sitting and floor sit with both hands free. Crawl on hands and knees, pull to stand, take steps holding furniture. Walk between 18 months - 2 years without assistive devices. |
| II | Infants maintain floor sitting but may need hands for support. Creep on stomach or crawl. May pull to stand and take steps holding furniture. |
| III | Infants maintain floor sitting when low back is supported. Roll and creep forward on stomachs. |
| IV | Infants have head control but trunk support is required for floor sitting. Can roll to supine and may roll to prone. |
| V | Physical impairments limit voluntary control. Unable to maintain antigravity head/trunk postures. Require assistance to roll. |
Between 6th and 12th Birthday
| Level | Description |
|---|---|
| I | Walk indoors/outdoors, climb stairs without limitations. Run & jump with reduced speed/balance. |
| II | Walk indoors/outdoors, climb stairs holding railing. Limitations on uneven surfaces/crowds. Minimal running/jumping. |
| III | Walk with assistive mobility device on level surfaces. Climb stairs with railing. Use wheelchair for long distances. |
| IV | Rely more on wheeled mobility. May use power wheelchair. |
| V | Restricted voluntary control. No independent mobility; transported. |
Clinical Presentation
History
Diagnosis begins with a history of gross motor developmental delay in the first year of life.
- Developmental Delay: CP frequently manifests as early hypotonia (first 6 months to 1 year), followed by spasticity.
- Primitive Reflexes: Persistent primitive reflexes (usually not diagnosed until after age 1 year).
- “Red Flags”: Definite hand preference before age 1 year (possible hemiplegia). Asymmetric crawling or failure to crawl.
- Growth Disturbance: Failure to thrive is often noted.
Detailed History:
- Prenatal: Exposure to toxins/infections, maternal diabetes, trauma, family history of neurologic disease.
- Perinatal: Gestational age, birth weight, Apgar scores, neonatal complications (seizures, jaundice, apnoea). -
- Developmental: Milestones (gross/fine motor, language, social). Unexplained regression suggests hereditary neurodegenerative disease, not CP. Review social skills, academic performance, and the need for standardized cognitive/educational testing to determine if therapy (speech, OT, PT) or adaptive equipment (communication devices, orthotics, specialized seating) is required.
Physical Examination
General Indicators:
- Joint contractures, hypotonic to spastic tone, growth delay.
- Tone: Abnormal neck or truncal tone; early hypotonia followed by spasticity (spasticity often manifests >6 months).
- Reflexes: Increased reflexes (UMN lesion), persistence of primitive reflexes (Moro, asymmetric tonic neck).
- Gait: Asymmetric posture, strength, or gait; abnormal coordination.
Musculoskeletal Assessment:
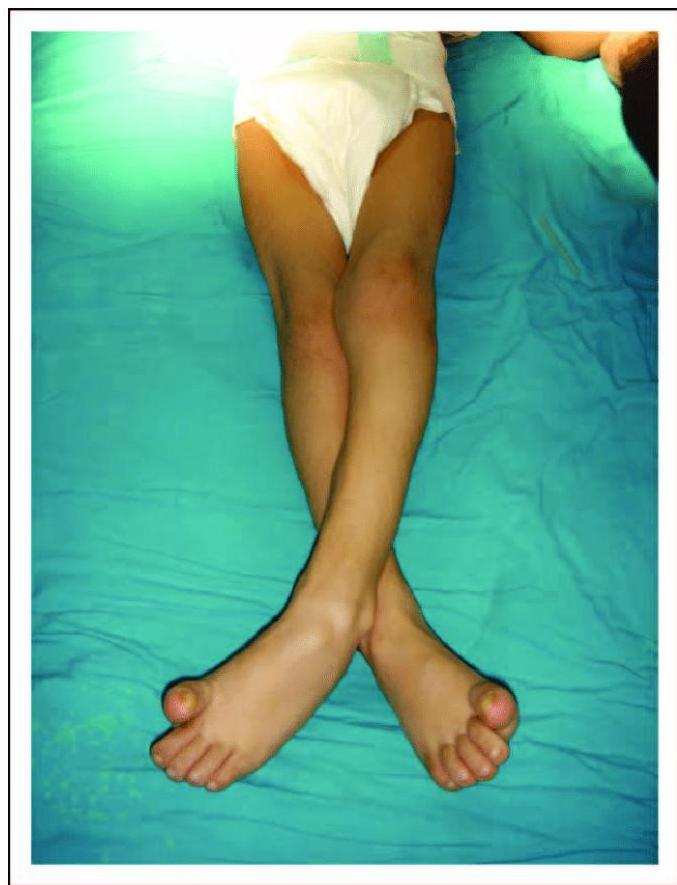
- Hip: Excessive flexion, adduction, femoral anteversion. Scissoring is common.
- Knee: Flexion/extension with valgus/varus stress.
- Foot: Equinus (toe walking), varus or valgus of hindfoot.
- Gait Abnormalities: Crouch position (tight hip flexors/hamstrings), weak quadriceps.

Specific Findings by Type
Spastic Hemiplegic:
- Presentation: One-sided UMN deficit. Arm > Leg.
- Signs: Weak hip flexion/ankle dorsiflexion, hip circumduction, supinated foot, shoulder adducted, elbow flexed, forearm pronated, wrist flexed, fisted hand, and unilateral sensory deficits.
- Associated: Cognitive impairment (28%), oromotor dysfunction, visual-field deficits (homonymous hemianopsia), strabismus, seizures.
Spastic Diplegic:
- Presentation: UMN findings in Legs > Arms.
- Signs: Hypotonia followed by extensor spasticity. Scissoring gait (hips flexed/adducted, knees flexed/valgus, ankles equinus).
- Associated: Cognitive impairment (30%), delay in gross motor skills. Seizures/learning disabilities less common than in hemiplegia.
Spastic Quadriplegic:
- Presentation: All limbs affected. Full-body hypertonia or truncal hypotonia with extremity hypertonia.
- Signs: Oromotor dysfunction.
- Associated: Multiple medical complications, seizures, increased risk of cognitive difficulties.
- Double Hemiplegic: If arms more involved than legs.

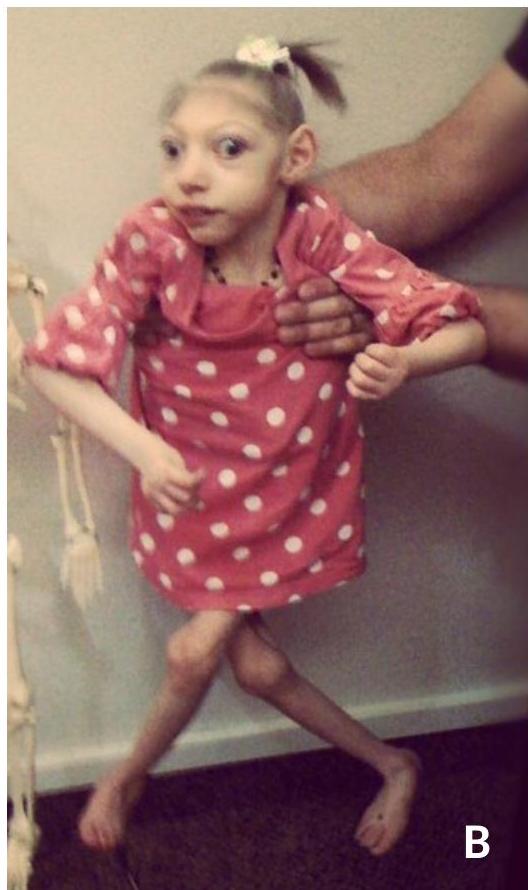 (A) Severe microcephaly. (B) Severe spastic quadriplegic CP.
(A) Severe microcephaly. (B) Severe spastic quadriplegic CP.
Dyskinetic (Extrapyramidal):
- Presentation: Arms > Legs. Early hypotonia, movement disorder emerges age 1-3 years.
- Signs: Involuntary movements (athetosis, chorea, dystonia) increasing with stress, excitement, or purposeful activity. Tone may be normal or decreased during sleep. Oromotor dysfunction (drooling, swallowing).
- Reflexes: DTRs usually normal to slightly increased.
- Associated: Intelligence normal in 78% of athetoid CP. Risk of sensorineural hearing loss (kernicterus).
 Child showing involuntary muscle spasms and poor saliva control.
Child showing involuntary muscle spasms and poor saliva control.
Primitive Reflexes
Persistence of primitive reflexes at 12 months is seen in patients with CP.

Diagnosis
Diagnosis is generally based on the clinical picture (history and physical examination). It should be deferred until the child is 2 years or older, as early motor abnormalities may resolve.
Diagnostic Criteria:
- Delayed motor milestones.
- Abnormal neurologic examinations.
- Persistence of primitive reflexes.
- Abnormal postural reactions.
Differential Diagnosis: Rule out progressive disorders:
- Degenerative diseases
- Metabolic diseases (e.g., glutaric aciduria)
- Genetic diseases / Hereditary spastic paraplegias
- Rett syndrome
- Spinal cord lesions (tethered cord)
- Muscular diseases
Investigations:
- Neuroimaging:
- Cranial Ultrasonography / CT / MRI:
- MRI is the study of choice for older children.
- Defines cortical/white matter structures (e.g., PVL, malformations) and appropriate myelination for age.
- MRI may help predict neurodevelopmental outcomes in preterm infants.
- Spine MRI if tethered cord suspected (e.g., worsening bowel/bladder function).
- 89% of children with CP have abnormal MRIs.
- Laboratory / Metabolic:
- Cerebrospinal Protein: Levels may assist in determining asphyxia in the neonatal period.
- Metabolic Workup: Thyroid function, Lactate/Pyruvate, Ammonia, Organic/Amino acids.
- Genetic: Chromosomal analysis.
- Neurophysiology: EEG (if seizures/hypoxic injury), EMG/Nerve conduction, Evoked potentials (auditory/visual).
Comorbidities
CP is often accompanied by associated illnesses:
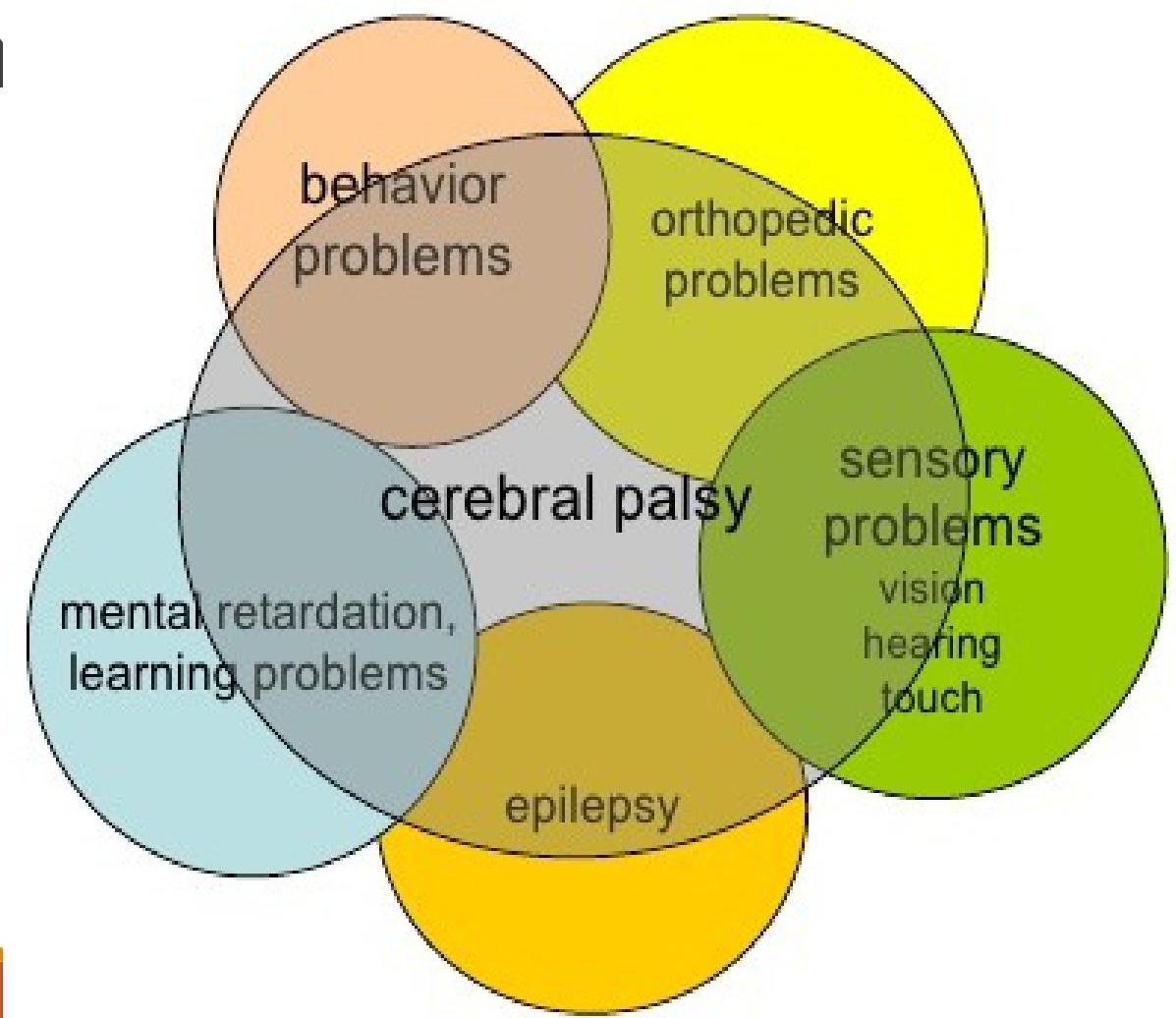
- Speech & Language Disorder: 60%
- Mental Retardation: 50%
- Visual Disorder: 40% (Myopia, squint, glaucoma, cortical visual impairment)
- Epilepsy: 25% (Focal more common; 70% onset in first year)
- Auditory Limitations: 5% (Higher risk of sensorineural hearing loss in kernicterus)
- Motor Disability: 60%
- Undernutrition: 30% (GER, pseudobulbar palsy)
- Other: Bladder/Bowel dysfunction (UTIs, constipation, incontinence), sleep disturbances, drooling, orthopedic abnormalities (contractures, scoliosis, hip dislocation).
Correlations:
- Spastic Diplegia ↔ Visual disorders
- Spastic Hemiplegia ↔ Epilepsy
- Spastic Quadriplegia ↔ Epilepsy & Mental Retardation
- Dyskinetic/Mixed ↔ Language-speech disorders
Management
Management is multidisciplinary:
- Developmental Pediatricians / Neurologists
- Rehabilitation: Pediatric physiatrists, Physical therapy (PT), Occupational therapy (OT).
- Speech Therapy
- Orthopedics


Treatment Modalities
- Goals: Maximize functional control, increase motor function, improve posture.
- Medication:
- Spasticity/Dystonia: Botulinum toxin (with/without casting). Effective for lower limb spasticity (age 2-17) to improve range of motion and delay surgery. Casting is especially useful for equinus deformity.
- Seizures: Antiepileptic drugs.
- Movement Disorders: Antiparkinsonian, anticonvulsant, antidopaminergic, and antidepressant agents.
- Surgical:
- Orthopedic surgery (contracture release, scoliosis correction).
- Neurosurgery (e.g., selective dorsal rhizotomy).
- Supportive: Management of feeding/swallowing (GER), adaptive equipment (orthotics, wheelchairs, communication devices).
Prognosis
- Ambulation: One of the most important issues for parents.
- Dependent on type and severity.
- Positive Predictors: Head balance before 9 months, rolling supine to prone by 18 months, independent sitting by 2 years (highly reliable).
- Cognition/Communication: Many have normal IQ but impaired communication due to oro-motor, fine motor, and gross motor difficulties, which can affect academic and social success.
- Quality of Life: Varies based on severity and functional disabilities. Survival depends on the number of disabilities.