Child Safety

Learning Objectives
By the end of this lecture, you will be able to:
- Define unintentional vs. intentional injuries.
- Understand the burden of childhood injuries globally and in Saudi Arabia.
- Apply age-specific injury prevention strategies (The Developmental Approach).
- Identify specific Saudi regulations regarding child safety (Car seats, Child Protection).
- Recognize radiological signs of abuse and accidental trauma.
The Burden of Injury
Epidemiology:
- Injuries are the leading cause of death in children > 1 year old in developed countries.
- 50% of childhood deaths are due to trauma.
- For every death, there are dozens of hospitalizations and hundreds of emergency department visits.
Terminology: “Accident” vs. “Injury”
- Concept: The word “Accident” implies unpredictability and unpreventability.
- Shift: Modern pediatrics uses “Unintentional Injury”—recognizing predictable patterns and preventable risks.
- Saudi Context: Vision 2030 emphasizes reducing road traffic fatalities.
The Epidemiologic Triangle (Agent-Host-Environment)
- Host (The Child): Age, development, behavior.
- Agent (The Source of Energy):
- Kinetic (cars)
- Thermal (fire)
- Chemical (poison)
- Electrical
- Environment:
- Physical (road design, home hazards)
- Social (parental supervision, socioeconomic status)
Developmental Approach
Infants (0 - 12 Months)
- Risks: Falls (changing table, beds), Suffocation (soft bedding), Shaken Baby Syndrome.
- Prevention:
- “Back to Sleep” (SIDS prevention).
- Never shake a baby.
- Supervision during bath time.
Toddlers (1 - 3 Years)
- Risks: Poisoning (exploration via mouth), Burns (scalds), Choking.
- Development: Mobile, curious, no impulse control, no danger sense.
- Prevention: Cabinet locks, stove guards, cut food into small pieces.
Preschoolers (3 - 5 Years)
- Risks: Pedestrian injuries (darting into traffic), Falls (playground), Drowning.
- Development: Increasing motor skills but poor judgment.
- Prevention: Supervision near roads, fencing pools, teaching “look left, right, left”.
School Age (5 - 12 Years)
- Risks: Bicycle injuries, Sports injuries, Dog bites.
- Prevention: Helmet use, protective gear, teaching road safety rules.

Adolescence (12 - 18 Years)
- Risks: Road Traffic Accidents (driver/passenger), Substance use, Suicide/Depression.
- Prevention: Driver education, graduated licensing, mental health screening.
- Saudi Context: High rates of MVC (Motor Vehicle Crashes) in young males.
Road Traffic Injuries (Saudi Guidelines Focus)
- Statistics: MVCs account for a significant portion of pediatric trauma mortality in Saudi Arabia.
- Mechanism: Unrestrained passengers, speeding, driver distraction.
- Photo Idea: [Graphic] Graph showing declining MVC rates in KSA post-implementation of traffic cameras.
Car Seat Safety (CRS) Guidelines
- Rear-Facing: As long as possible (minimum until age 2, or per seat weight limit).
- Forward-Facing: Harness until max weight/height reached.
- Booster Seat: Until the seat belt fits properly (usually <145cm height or <10 years).
- Saudi Traffic Law: Mandatory use of CRS (Child Restraint Systems) for children.
The “Seat Belt Sign” & Trauma Clinical Sign: Bruising across the abdomen/lap from a seat belt during high-impact deceleration. Implication: High risk of intestinal perforation or lumbar spine fracture (Chance fracture)

Pedestrian Safety
- Problem: Children are small and hard to see; they judge speed poorly.
- Prevention: Sidewalks, crossing guards, speed bumps near schools (common in KSA urban planning).
Burns & Thermal Injuries
Types of Pediatric Burns
- Scald Burns (60-70%): Hot liquids, bath water. Most common in toddlers.
- Flame Burns: House fires, playing with lighters.
- Contact Burns: Touching stoves, irons.
- Electrical Burns: Mouth burns (biting cords).
Burn Severity Assessment
- Depth:
- Superficial (1st degree)
- Partial Thickness (2nd degree)
- Full Thickness (3rd degree)
- Rule of 9s (Lund-Browder): Children have larger heads relative to bodies than adults.
- Critical Burn Area: >10% TBSA (Total Body Surface Area) in a child is considered a major burn.
Scald Prevention
- Tap Water: Set water heater to <49°C (120°F).
- Cooking: Turn pot handles inward, use back burners, do not carry hot liquids while holding a child.

Electrical Injuries
- Oral Commissure Burns: Occurs when a child bites an extension cord.
- Management: Monitor for labial artery bleeding (can occur 7-10 days later as eschar separates).

Falls
Prevention
- Baby Walkers: CONTRAINDICATED. They allow mobility before the child is ready and increase the risk of falling down stairs.
- Windows: Install window guards (stops). Do not rely on screens.
- Playgrounds: Shock-absorbing surfaces (sand/rubber) under equipment.
Radiology in Pediatric Trauma
Radiographic Signs of Trauma (X-Rays)
- Nursing Maid’s Elbow (Radial Head Subluxation): Common in toddlers (pulled arm).
- X-Ray Findings: Usually normal; diagnosis is clinical subluxation.
Pediatric Fracture Patterns
- Greenstick Fracture: One cortex broken, one intact (bends like a twig).
- Torus/Buckle Fracture: Bulging of cortex due to compression.
- Growth Plate (Salter-Harris) Injuries: Potential for growth arrest.
Poisoning & Ingestion
Epidemiology of Poisoning
- Peak Age: 1-3 years (exploratory ingestion).
- Common Agents: Medications, cleaning products, petroleum distillates, hydrocarbons (kerosene is common in some regions).
- Saudi Poison Control Centers: Available 24/7.
Prevention Strategies
- Storage: Keep poisons in locked cabinets, above shoulder height.
- Packaging: Child-resistant caps (CRCs) are effective but not child-proof.
- Labeling: Never transfer chemicals to food/drink containers (e.g., bleach in a water bottle).
The “Button Battery” Emergency Risk
- Risks: Esophageal burns, fistula formation (tracheoesophageal), hemorrhage.
- X-Ray Sign: “Double Halo” or “Step-off” sign on lateral view.
- Action: Immediate removal required if stuck in the esophagus.

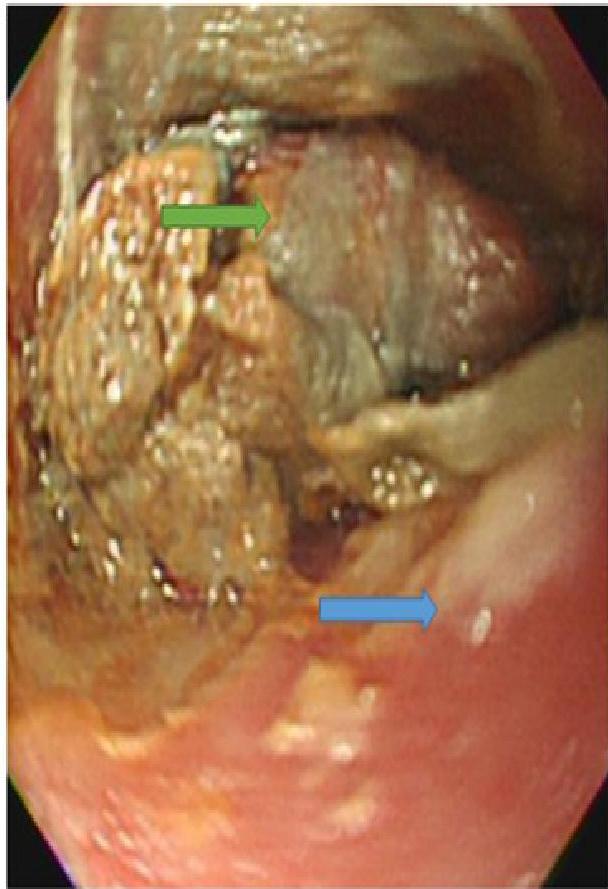
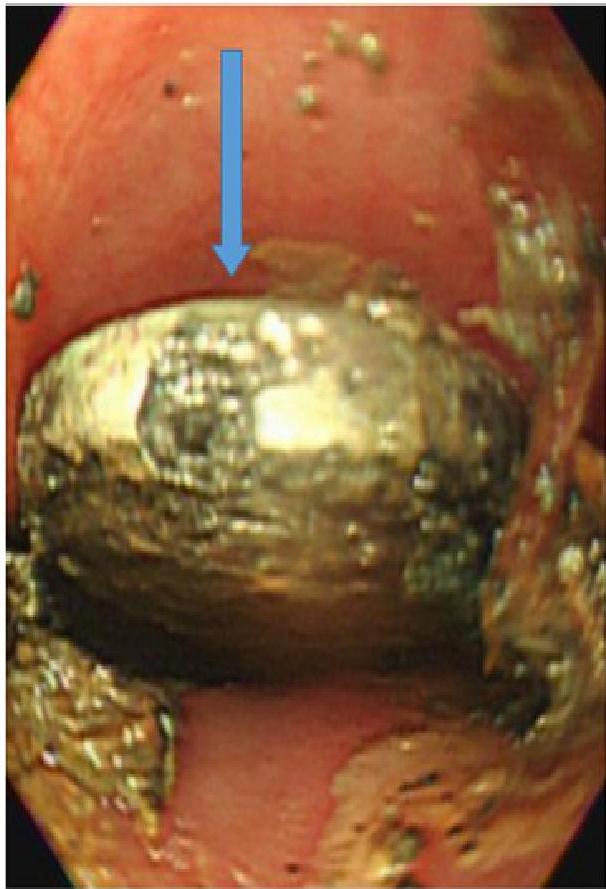 A, B, C: Imaging examples of button battery ingestion.
A, B, C: Imaging examples of button battery ingestion.
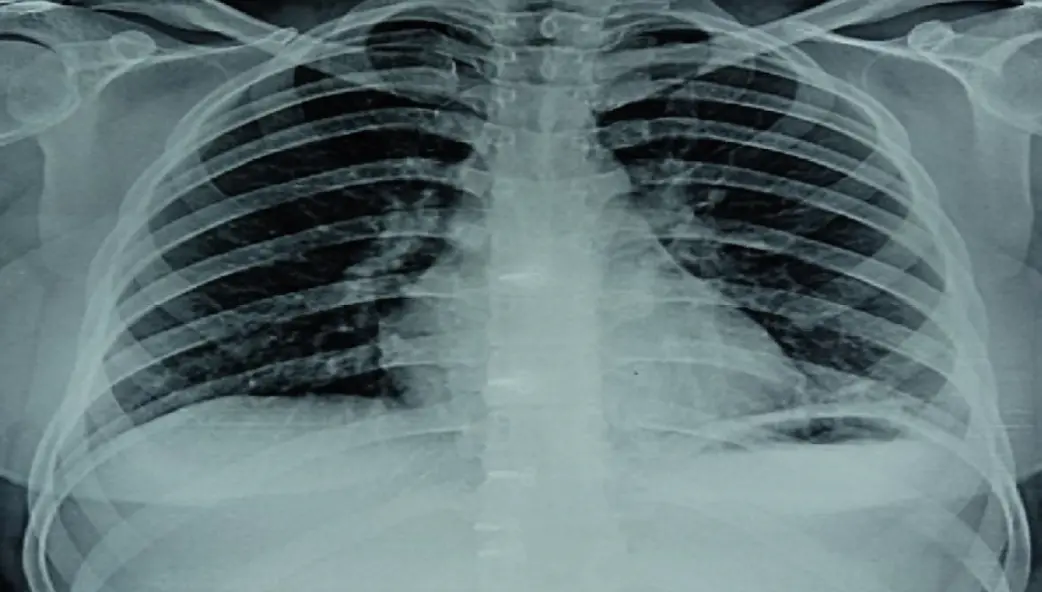
Hydrocarbons (Inhaled/Ingested)
- Agents: Kerosene, gasoline, lighter fluid.
- Pathophysiology: Low surface tension → aspiration pneumonitis.
- Clinical: Coughing, choking, hypoxia.
- X-Ray Finding: Pneumonitis (often within hours), usually in the lower lobes.
Drowning
- “Silent Killer”: No splashing or screaming usually.
- Time: Irreversible brain damage occurs in 4-6 minutes.
- Risk Sites: Home swimming pools (villas), bathtubs (infants), wadis (seasonal).
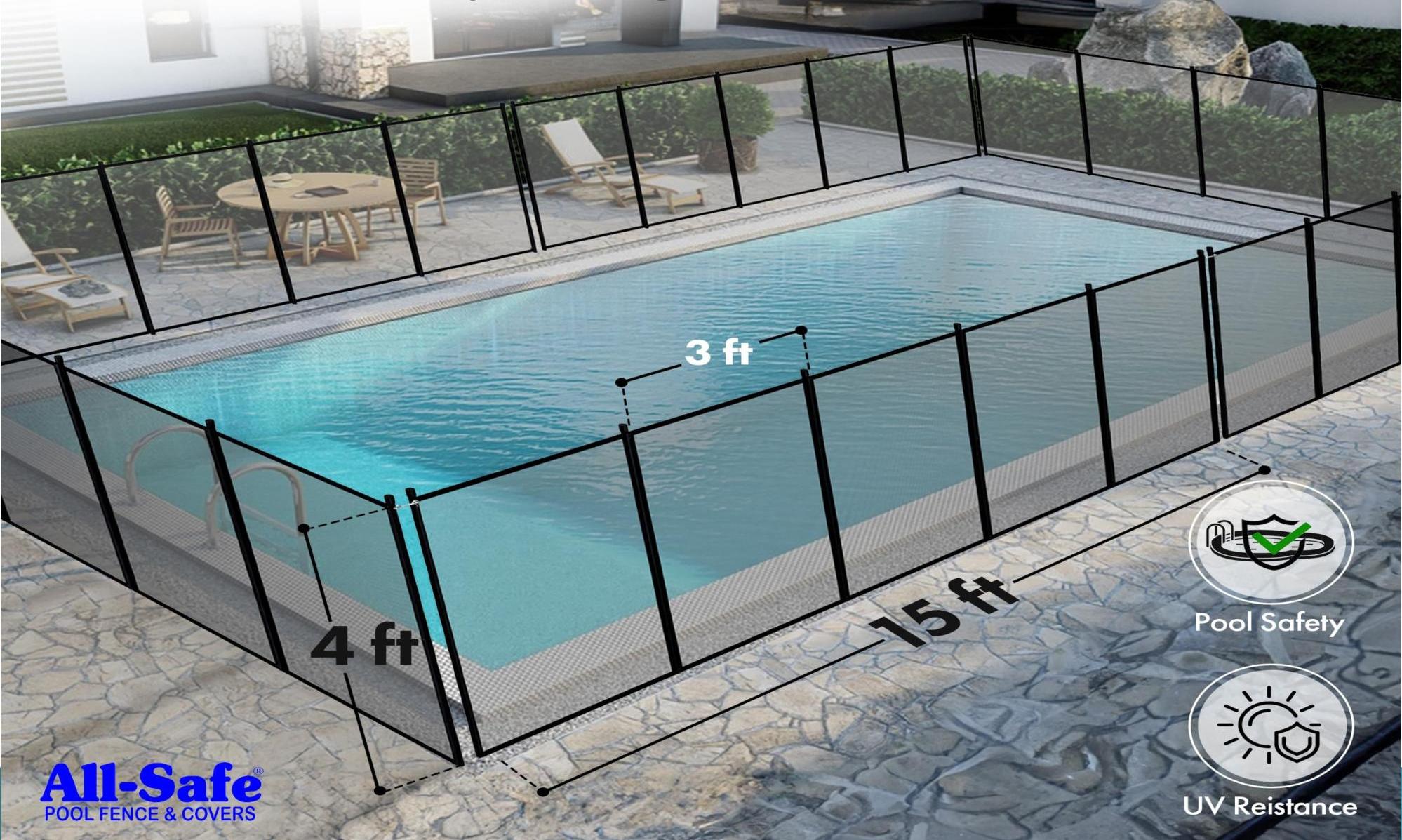
- Saudi Context: Increasing number of private pools necessitates strict fencing laws.
Prevention of Drowning
- Fencing: Isolate the pool from the house (climb-resistant).
- Supervision: “Touch Supervision” for toddlers (within arm’s reach).
- Life Jackets: Mandatory when boating or swimming in open water.
Enhanced Protection (Fencing)
Child Abuse & Neglect (Non-Accidental Trauma)
- Defining Abuse:
- Saudi Child Protection Law (2015): Criminalizes physical, psychological, and sexual abuse of children.
- Physician’s Role: Mandatory reporting.
- Protection of the child supersedes confidentiality.
Bruises: Accidental vs. Suspicious
- Accidental: Shins, knees, forehead (bony prominences).
- Suspicious:
- “Trophy Sign”: Bruises to ears, cheeks, inner thighs, genitals.
- Handprint: Shape of a grab or slap.
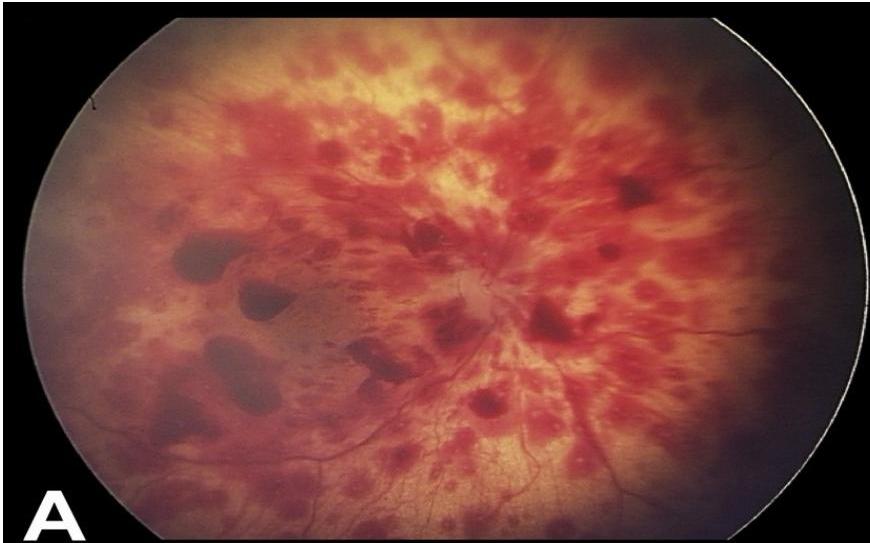
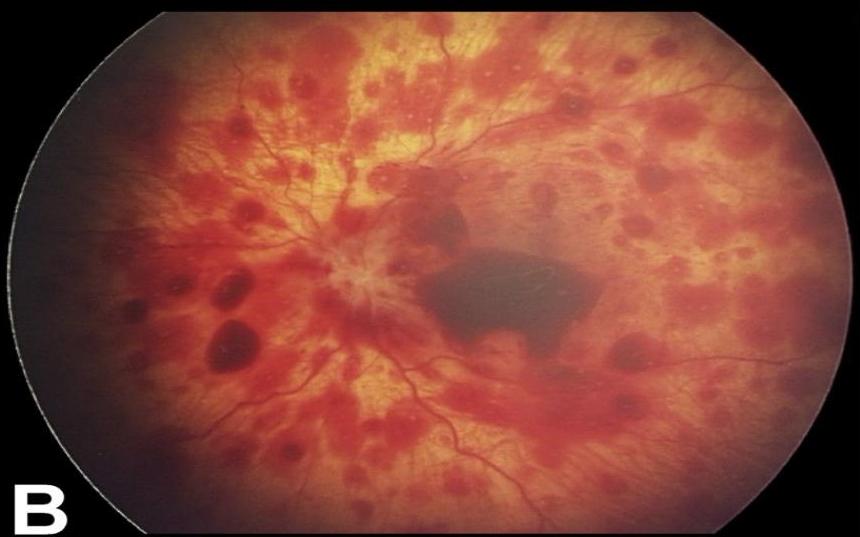
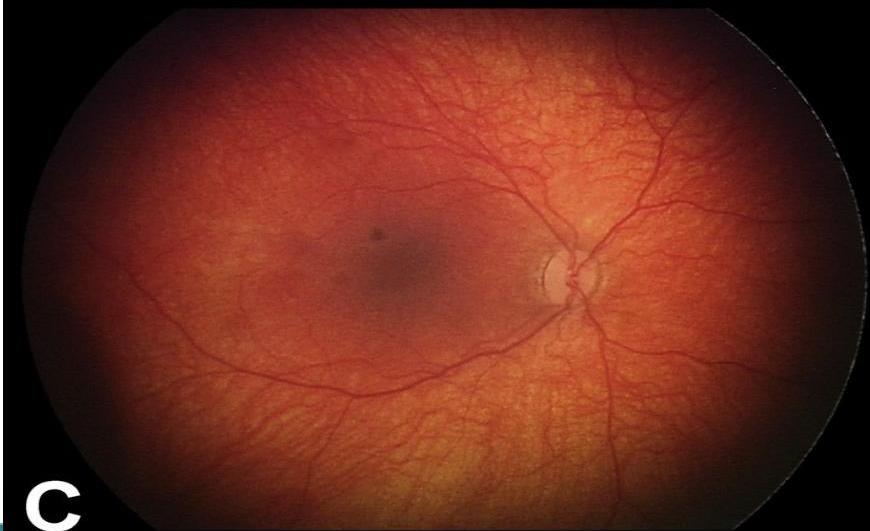
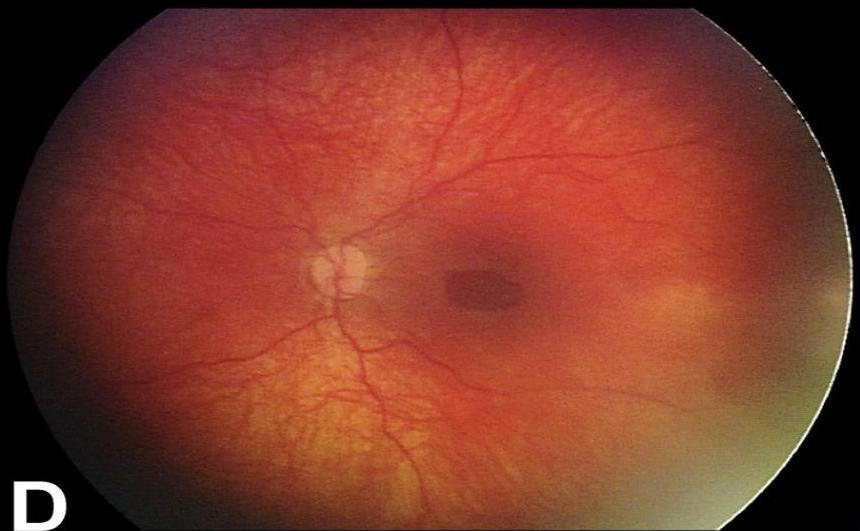
Shaken Baby Syndrome (Abusive Head Trauma)
- Mechanism: Violent shaking causing acceleration-deceleration forces.
- The Triad:
- Subdural Hematoma.
- Retinal Hemorrhages.
- Encephalopathy (diffuse brain injury).
Radiologic Signs of Abuse (Fractures)
- Classic Metaphyseal Lesion (CML): “Bucket handle” or “Corner fracture” due to traction on limbs.
- Rib Fractures: Posterior rib fractures (highly specific for squeezing).
- Patterns: Multiple fractures in different stages of healing.
Skeletal Survey (The “Babygram”)
- Indication: Any child <2 years with suspicious injuries.
- Protocol: Includes AP/Lateral of all limbs, skull, chest, spine, pelvis, hands, and feet.
- Note: Do not confuse “Babygram” (single shot) with a proper Skeletal Survey (multiple films).
Choking Hazards
- Foods: Grapes, hot dogs, nuts, popcorn (round/solid foods).
- Objects: Balloons (leading cause of toy death), coins, small batteries.
- Prevention: Cut grapes/hot dogs lengthwise, no nuts under age 4.
Safe Sleep Environment
- Sudden Infant Death Syndrome (SIDS)
- Triple Risk Model:
- Vulnerable infant (brainstem defect).
- Critical developmental period (1-6 months).
- Exogenous stressor (prone sleeping, overheating).
- Safe Sleep (ABC): Alone, on Back, in Crib.
- Firm Mattress: No soft bedding, pillows, or bumpers.
- Room Sharing vs. Bed Sharing: Room sharing is recommended; Bed sharing increases risk.
- Pacifier Use: Protective effect against SIDS after breastfeeding established.
Implementation & Conclusion
The “TEAR” Model for Prevention:
- Trauma surveillance (Data collection).
- Education (Parents and children).
- And Environmental modification (Product safety, laws).
- Renforcement (Regulations, Seatbelt laws).
- Audit (Monitoring effectiveness).
Summary of Key Points
- Injuries are predictable, preventable, and treatable.
- Age-specific risks dictate the prevention strategy (Developmental Approach).
- MVCs, Burns, Drowning, and Falls are the “Big 4” mechanisms.
- Abuse: Always have a high index of suspicion; know the legal requirement to report in Saudi Arabia.
- X-rays and photos are crucial tools for diagnosis and legal documentation.
References
- Kliegman, R. M., et al. Nelson Textbook of Pediatrics, 21st Edition.
- Lissauer, T., & Clayden, G. Illustrated Textbook of Paediatrics, 5th Edition.
- Saudi Ministry of Health. Child Abuse and Neglect Protocol.
- Saudi Traffic Law (Royal Decree No. M/85).
