JUVENILE IDIOPATHIC ARTHRITIS (JIA)
Definition & Overview
- JIA represents a heterogeneous group of disorders sharing the clinical manifestation of arthritis.
- JIA incorporates all of what was called JRA (Juvenile Rheumatoid Arthritis) in the past and all other forms of “idiopathic” arthritis in childhood.
- JIA is the most common rheumatic disease in children and one of the more common chronic illnesses of childhood.
- It is an autoimmune disorder:
- Multiple HLA loci are associated with the development of JIA.
- Associated with alterations in both humoral and cell-mediated immunity.
- T lymphocytes have a central role, releasing proinflammatory cytokines favoring a type 1 helper T-lymphocyte response.
Classification Criteria (Juvenile Rheumatoid Arthritis)
Modified from Cassidy JT, Levinson JE, Bass JC et al: A study of classification criteria for a diagnosis of juvenile rheumatoid arthritis, Arthritis Rheum
- Age at onset: <16 yr
- Arthritis: Swelling or effusion, or presence of two or more of the following signs: limitation of range of motion, tenderness or pain on motion, and increased heat in one or more joints.
- Duration of disease: 6 wk or longer
- Onset type defined by type of disease in first 6 mo:
- Polyarthritis: ≥5 inflamed joints
- Oligoarthritis (pauciarticular disease): <5 inflamed joints
- Systemic-onset: Arthritis with characteristic fever
- Exclusion of other forms of juvenile arthritis
Types of JIA
- Systemic-onset juvenile idiopathic arthritis
- Oligoarticular juvenile idiopathic arthritis (1-4 joints)
- Polyarticular juvenile idiopathic arthritis (RF+): 2 positive tests at least 3 months apart.
- Polyarticular juvenile idiopathic arthritis (RF-)
- Psoriatic arthritis
- Enthesitis-related arthritis
- Undifferentiated arthritis
Definitions of Clinical Terms
- Quotidian fever: Defined as a fever that rises to 39°C once daily and returns to 37°C between fever peaks.
- Serositis: Refers to pericarditis, pleuritis, or peritonitis.
- Dactylitis: Swelling of one or more digit(s), usually in an asymmetric distribution, that extends beyond the joint margin.
- Nail pitting: A minimum of two pits on any one or more nails at any time.
- Enthesitis: Defined as tenderness at the insertion of a tendon, ligament, joint capsule, or fascia to bone.
- Inflammatory lumbosacral pain: Refers to lumbosacral pain at rest with morning stiffness that improves on movement.
JIA Exclusion Criteria
- Psoriasis History: A personal history of or first-degree relative affected by psoriasis. Patients meeting this criterion are excluded from all categories except for psoriatic arthritis and undifferentiated arthritis.
- Specific Conditions History: A personal history of or first-degree relative affected by certain conditions (including ERA, ankylosing spondylitis, sacroiliitis with inflammatory bowel disease [IBD], reactive arthritis, and/or acute anterior uveitis). Patients meeting this criterion are excluded from all categories except for ERA and undifferentiated arthritis.
- HLA-B27 in Males: Arthritis starting after six years of age in a male patient who is positive for HLA-B27. Patients meeting this criterion are excluded from all categories except for ERA and undifferentiated arthritis.
- Positive RF: Positive testing for RF (defined as having a positive immunoglobulin M RF test on at least two occasions checked at least three months apart within the first six months of disease). Patients meeting this criterion are excluded from all categories except for polyarthritis and undifferentiated arthritis.
Clinical Manifestations
Arthritis Characteristics
- Arthritis Diagnosis: Must be present ≥6 weeks to make a diagnosis of any JIA subtype.
- Definition: Intraarticular swelling OR the presence of two or more of the following signs:
- Limitation in range of motion (ROM)
- Tenderness or pain on motion
- Warmth
- Synovitis: Characterized by synovial proliferation and increased joint volume.
- The joint is held in a position of maximum comfort.
- Range of motion often is limited only at the extremes.
- Fingers: May appear swollen; range of motion becomes painful.
- Wrist: Goes into flexion.
- Knee: Parapatellar fossae often are obliterated; doughy synovium may be palpable. A soft, boggy swelling is appreciated in the popliteal fossa.
- Hip/TMJ/Spine: Do not demonstrate swelling when affected by synovitis but demonstrate the combination of loss of motion and pain. The hip is held in an attitude of flexion, abduction, and external rotation; guarding is an early sign.
- Presentation:
- Either insidious or abrupt disease onset.
- Often with morning stiffness or gelling phenomenon (stiffness after long periods of sitting or inactivity) and arthralgia during the day.
- Involved joints are often swollen, warm to the touch, and uncomfortable on movement or palpation with reduced ROM, but usually are not erythematous.
- Children often stop using joints normally (e.g., develop contractures, decreased wrist range, limp) rather than complain of pain. Up to a quarter of children with oligoarticular JIA have no pain.
- Growth Effects:
- Arthritis in large joints (especially knees) initially accelerates linear growth causing limb length discrepancy.
- Continued inflammation stimulates rapid and premature closure of the growth plate, resulting in shortened bones.
Systemic & General Symptoms
- Easy fatigability and poor sleep quality.
- History of school absences or limited ability to participate in physical education classes.
- Spiking fevers (Systemic-onset JIA).
- Skin rash (Systemic-onset JIA).
Comparison of Major JIA Subtypes Z
| Feature | Systemic JIA | Oligoarticular JIA | Polyarticular JIA |
|---|---|---|---|
| Percent of JIA patients | 10 to 15% | 50% | 30 to 40% |
| Sex | F = M | F > M | F > M |
| Age | Any <17 years | Peak 2 to 3 years, rare >10 | Peaks 2 to 5, 10 to 14 years |
| Joints | Any number and any joint | Large joints, but rarely hips | Any, usually symmetrical; rare to start in hips |
| Fever, Rash, LAD, HSM | Yes | No | No |
| Uveitis | Rare | 20% (Most common in ANA+ patients) Z | Less frequent than in Oligo |
| Laboratory Abnormalities | |||
| - Leukocytosis | Marked | No | No |
| - Anemia | Marked | No | Mild |
| - Elevated ESR | Marked | Mild | Mild |
| - ANA | Absent | Low titer common | Low titer common in younger |
| - Rheumatoid Factor | Rare | Absent | 10-20% in those >10 years |
| - Elevated Ferritin | Marked | No | Mild |
| Destructive Arthritis | >50% | Rare | >50% |
| DMARDs / Biologics | Commonly used | Rarely used | Commonly used |
F: female; M: male; ANA: antinuclear antibody; ESR: erythrocyte-sedimentation rate; LAD: Lymphadenopathy; HSM: Hepatosplenomegaly. (Source: UpToDate)
SYSTEMIC-ONSET JUVENILE IDIOPATHIC ARTHRITIS (sJIA) / STILL’S DISEASE
Diagnosis & Definition
- Diagnosis of Exclusion: sJIA is a diagnosis of exclusion.
- Hallmark: Combination of intermittent but daily fevers >38.5°C (quotidian fever pattern) and arthritis.
- Criteria:
- ILAR: Fever must be present for at least two weeks and arthritis for at least six weeks for definitive diagnosis.
- CARRA: Modified criteria do not include arthritis as a required criterion for early diagnosis and treatment.
- Arthritis Development: A definite diagnosis must await the development of arthritis. This may occur at onset of fever/rash or lag by months or (rarely) years.
- Work-up: Thorough work-up for Fever of Unknown Origin (FUO) is recommended to exclude infection (blood/urine cultures, viral studies), IBD, and malignancy (CT abdomen/pelvis, BM aspiration).
- Adult-onset Still’s disease: Clinically similar illness in adults/adolescents >16 years.
Clinical Manifestations (sJIA)
- General: Child appears systemically ill. Peak age at onset 1-5 years.
- Fever: High spiking temp to ≥39°C, occurs once or twice daily for at least 2 weeks. Rapid return to normal/subnormal temp. Often presents in the evening and accompanied by characteristic rash.
- Rash:
- Evanescent (lasting a few hours), salmon-pink, macular (often linear).
- Predominantly on trunk and extremities.
- typically nonpruritic (occasionally extremely pruritic).
- Migratory and associated with fever spikes.
- Koebner phenomenon is present. Heat can also evoke rash.
- Arthritis: May affect any number of joints; course is classically polyarticular. Can be very destructive and include hip, cervical spine, and TMJ involvement.
- Musculoskeletal:
- Arthralgia: Often present early.
- Myalgia: Generalized, muscle tenderness to palpation.
- Organomegaly: Marked hepatosplenomegaly, lymphadenopathy (especially axillary).
- Serositis:
- Pleural and pericardial effusions.
- Chest pain/shortness of breath (signs of pericarditis/pleuritis).
- Friction rub may occur.
- Myocarditis: , basilar rales, and hepatomegaly suggestive of heart failure.
Imaging Findings (sJIA)
Early radiographic changes (6 month duration): Soft tissue swelling and periosteal new bone formation appear adjacent to the second and fourth proximal interphalangeal joints.

Typical Rash: - Salamon rash - macular raises above the skin. - associated w/ fever - mainly on trunk extremely itchy. -

Pericardial Effusion:
 X-RAY of child with pericardial effusion
X-RAY of child with pericardial effusion
Complications of sJIA
- Endarteritis, Serositis.
- Macrophage Activation Syndrome (MAS).
- Inflammatory lung disease: Pulmonary alveolar proteinosis and/or endogenous lipoid pneumonia.
- CNS disease.
- Hematologic: Hemolytic anemia, Pancytopenia.
- Chronic Arthritis: Progresses rapidly causing severe damage, dysfunction, need for joint replacement surgery.
- Loss of growth potential in younger patients.
- Tenosynovitis and synovial cysts.
- Micrognathia and cervical spine fusion (longstanding disease).
Macrophage Activation Syndrome (MAS) / Hemophagocytic Lymphohistiocytosis (HLH)
- Rare but potentially fatal complication of sJIA (can occur at any time).
- Pathophysiology: Excessive activation and expansion of macrophages and T cells, release of massive amounts of cytokines (cytokine storm). Can be familial/sporadic or triggered by Infections, malignancies, rheumatologic disorders, immunodeficiencies.
- Manifestations: Acute onset high-spiking fevers, lymphadenopathy, hepatosplenomegaly, encephalopathy, purpura, mucosal bleeding (DIC: elevated fibrin split products, prolonged PT/PTT).
- Labs: ESR falls (hypofibrinogenemia/hepatic dysfunction), leukopenia, elevated LDH.
- Criteria for sJIA-associated MAS:
- Hyperferritinemia (>684 ng/mL) AND any two of:
- Thrombocytopenia (≤181 × 10⁹/L)
- Aspartate transaminase >48 U/L
- Hypertriglyceridemia (>156 mg/dL)
- Hypofibrinogenemia (≤360 mg/dL)
- Bone Marrow: Biopsy/aspirate usually shows hemophagocytosis.
- Hyperferritinemia (>684 ng/mL) AND any two of:
Differential Diagnosis (sJIA)
- Infection: Endocarditis, rheumatic fever, brucellosis, MIS-C, Septic arthritis, Osteomyelitis, Subacute bacterial endocarditis, Malaria, Viral/Postinfectious arthritis (self-resolving).
- Other Rheumatic Disorders: SLE, vasculitis syndromes, serum sickness, Kawasaki disease, sarcoidosis.
- Malignancy: Leukemia, neuroblastoma, lymphoma.
- Other: Inflammatory bowel disease (IBD), HLH syndromes, Autoinflammatory (episodic fever) syndromes.
OLIGOARTICULAR JUVENILE IDIOPATHIC ARTHRITIS
Definition & Clinical Features
- Definition: Involvement of four or fewer joints within the first 6 months of disease onset. Often only a single joint is involved.
- Prevalence: 50% of JIA.
- Affected Joints: Knees and ankles typically affected.
- Extended Oligoarticular JIA: Evolution of disease in five or more joints after 6 months (worse prognosis).
- Presentation:
- Children appear to be well, despite ambulating with a limp.
- Flexion contractures in knees and (less commonly) wrists.
- Muscle atrophy: Often of extensor muscles (e.g., vastus lateralis, quadriceps).
- Leg-length discrepancy: Chronic inflammation-related hyperemia in a knee or ankle leads to overgrowth of that limb (in asymmetrical arthritis).
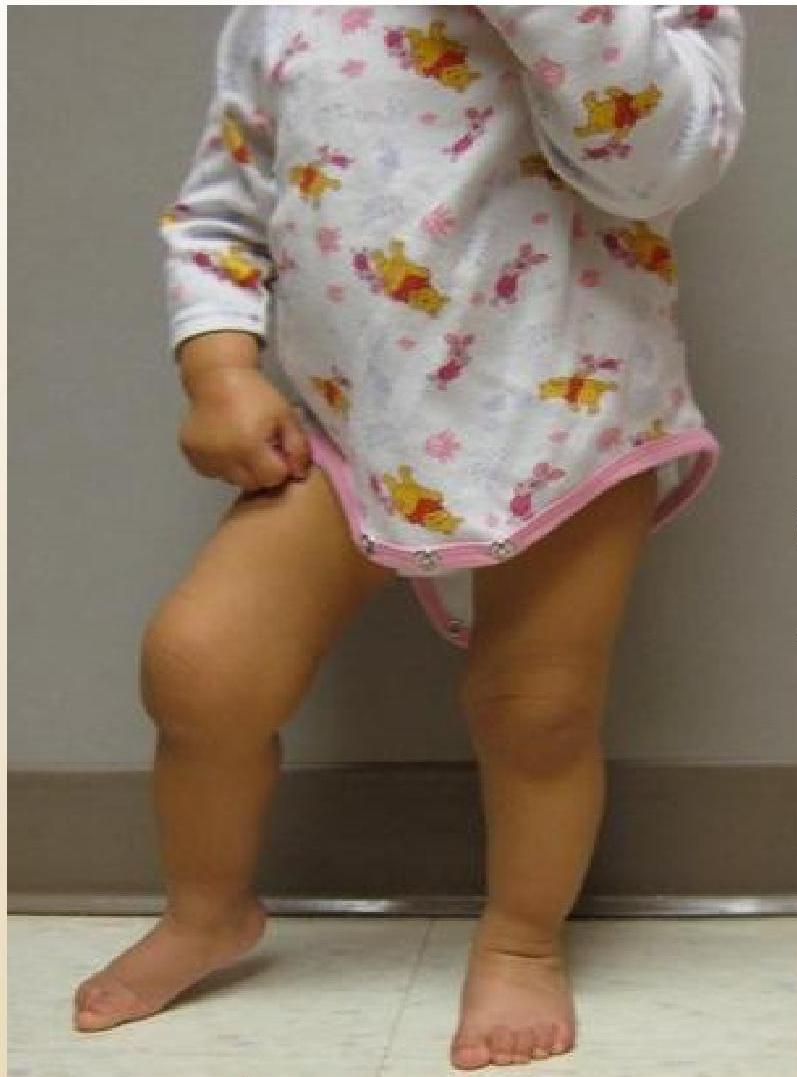 18M-old girl with arthritis in right knee. Note the flexion contracture of that knee.
18M-old girl with arthritis in right knee. Note the flexion contracture of that knee.
Complications: Anterior Uveitis
- Occurs in 20% of children with oligoarticular JIA.
- Risk Factors: ANA positive (correlates with younger age, females, asymmetric arthritis), young girls.
- Nature: Asymptomatic.
- Screening: Evaluation with a slit-lamp every 4 months is required.
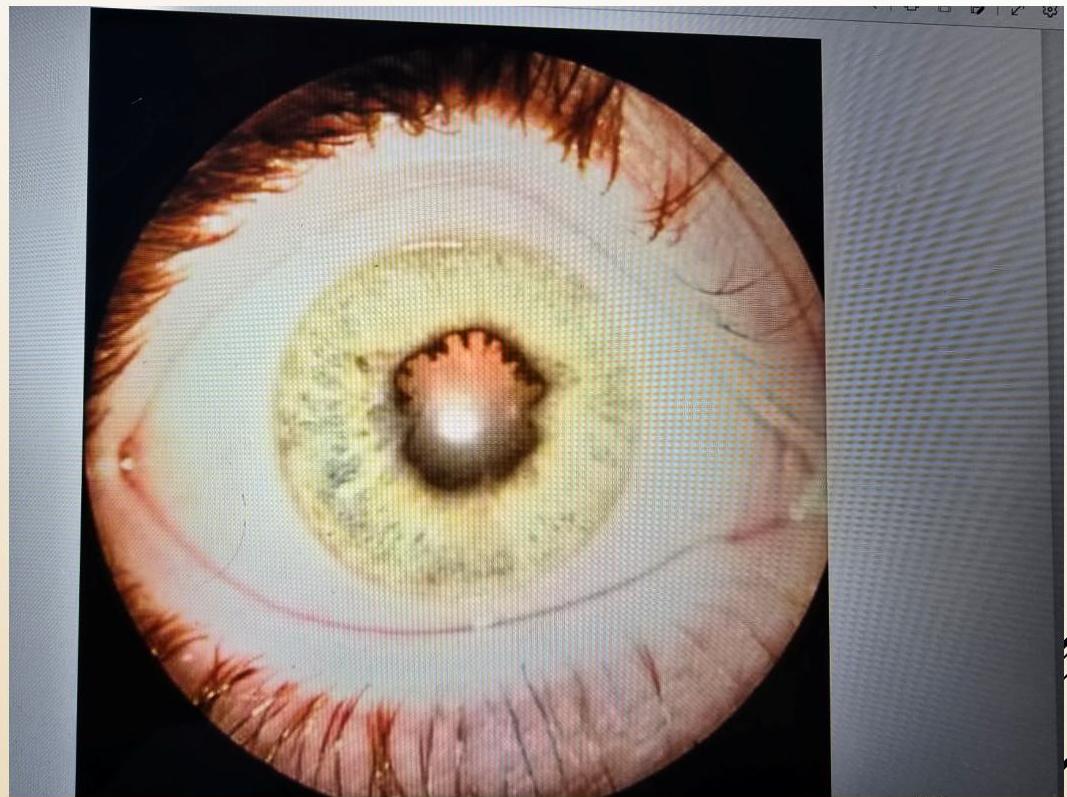 Chronic anterior uveitis demonstrating posterior synechiae
Chronic anterior uveitis demonstrating posterior synechiae
POLYARTICULAR JUVENILE IDIOPATHIC ARTHRITIS
Definition & Epidemiology
- Definition: Inflammation of five or more joints in both upper and lower extremities in the first 6 months after disease onset.
- Prevalence: 20-30% of JIA patients. More frequent in Females than Males.
- Age of Onset: Two peaks: 2-5 years and 10-14 years.
Clinical Subtypes & Presentation
1. RF Negative Polyarthritis
- Population: Most children with polyarticular-onset. Usually younger children (2-5 years).
- Features:
- Disease is not etiologically similar to adult-onset RA. No anti-CCP.
- Onset: Often indolent with 1-2 joints affected until intercurrent infection, then progressive spread to ≥5 joints in first 6 months.
- Pattern: Symmetric involvement. Knees, wrists, and ankles most frequently affected.
- Course: Typically periods of response to therapy followed by relapses with increasing number of joints.
2. RF Positive Polyarthritis
- Population: Uncommon in children <10 years. Older children/adolescents. Likely female.
- Features:
- Resembles characteristic symmetric presentation of adult rheumatoid arthritis.
- More severe/aggressive disease course.
- Markers: Some HLA-DR4 positive, have anti-CCP antibodies.
- Onset: Rapid onset of inflammation in multiple joints (including small joints of hands/feet) within 2-3 months.
- Rheumatoid Nodules: May be seen on extensor surfaces of elbows, spine, and over Achilles tendons.
- Joints: Fingers, wrists, elbows, hips, knees, ankles. Pain/stiffness in small joints common.
Specific Musculoskeletal Manifestations
- Hands:
- Symmetric involvement of small joints.
- Swelling of PIP joints, boney overgrowth. Z
- Interosseous muscle wasting (dorsum of hands).
- Subluxation and ulnar deviation of wrists.
- Cervical Spine:
- Decreased extension is asymptomatic.
- Can lead to subluxation (typically C2 on C3).
- Radiographic: Fusion of neural arch (C2-C3), narrowing/erosion of remaining joints, obliteration of apophyseal space, loss of normal lordosis.
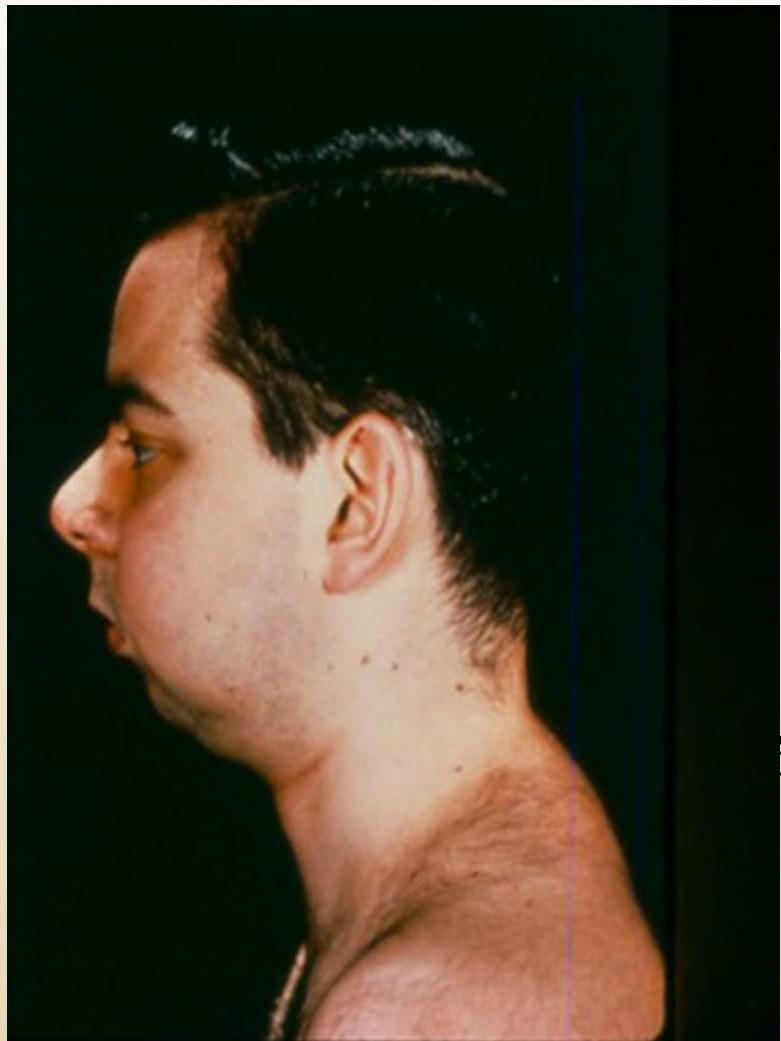
- Temporomandibular Joint (TMJ):
- Typically asymptomatic; signs include decreased mouth aperture, lateral deviation of jaw gait.
- Auscultatory abnormalities (signs of underlying arthritis).
- May lead to micrognathia.
- Weight-bearing joints: Commonly affected.
- Bone Health: Osteopenia and osteoporosis may occur.
Radiographic Progression (Examples)
Hand Progression: A: Radiograph at onset. B: 4 years later - Loss of articular cartilage, destructive changes in distal/proximal interphalangeal and metacarpophalangeal joints, destruction and fusion of wrist bones.
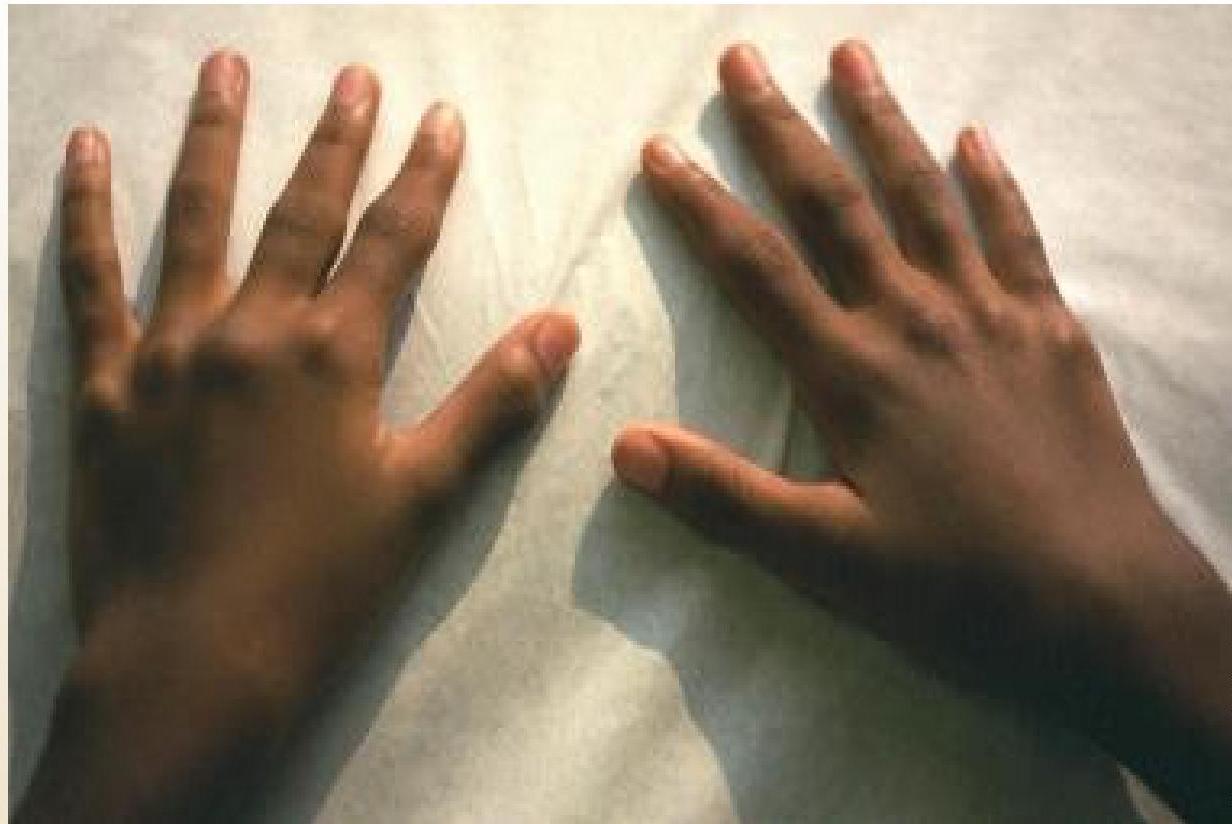
 (Left: Patient with active polyarticular arthritis. Right: Radiographic progression)
(Left: Patient with active polyarticular arthritis. Right: Radiographic progression)
Cervical Spine:

 (Left: Fusion of neural arch C2-C3. Right: Flexion/extension views)
(Left: Fusion of neural arch C2-C3. Right: Flexion/extension views)
TMJ (Micrognathia):
Ocular Manifestations (Polyarticular)
- Less common than in oligoarticular type.
- Usually ANA titer positive.
- More common with RF Negative than RF Positive.
- More common with 1st peak incidence (2-5 years).
- Management: Routine eye examination aiming to minimize risk of ocular complications due to late diagnosis/treatment of uveitis.
Laboratory Tests
- Routine: CBC, CMP, ESR, CRP, ANA, RF, Anti-CCP, HLA-B27.
- Findings:
-
ESR (≥40 mm/H), Anemia (HB ≤11 g/dL), Hypergammaglobulinemia. present in P-JIA
-
ANA: Many younger children are positive (marker for increased uveitis risk). Antibodies to dsDNA, Sm, SSA or Ro, SSB or La, or RNP are not expected in polyarticular JIA.
-
RF: Positive results should be confirmed after 3 months. Rare in <10 years. Children with polyarticular disease are divided to polyarthritis RF negative and polyarthritis RF positive : Most children with polyarticular-onset disease are RF negative and don’t have antibodies to CCP . Their disease is not etiologically similar to adult-onset RA . Older children with RF are likely female , have more severe disease, mimicking adult RA. Some HLA-DR4 positive , have anti-CCP antibodies, aggressive disease course in the absence of appropriate therapy
-
Specific Abs: Antibodies to dsDNA, Sm, SSA/Ro, SSB/La, or RNP are not expected.
-
Diagnosis & Differential
- Diagnosis: Clinical. Requires arthritis in >4 joints during first 6 months. Exclude other causes. No specific diagnostic test. Other causes of arthritis must be excluded, primarily based upon clinical history and exam findings There are no specific diagnostic tests to confirm the diagnosis. Rather, it is a clinical diagnosis
- Differential Diagnosis:
- Reactive arthritis,
- Psoriatic JIA,
- Enthesitis related JIA,
- Systemic JIA.
- SLE and Mixed connective tissue disease (MCTD),
- Systemic vasculitis.
- Sarcoidosis,
- Juvenile systemic granulomatosis (Blau syndrome).
- Inflammatory bowel disease.
- Malignancy.
- Epiphyseal dysplasia.
JIA MANAGEMENT & TREATMENT
- Approach: Supportive not curative. Multidisciplinary team (Pharmacologic, Psychosocial, Physical, Occupational therapy, Nutrition).
- Goals:
- Control pain.
- Suppress articular and/or systemic inflammation with lowest risk.
- Maintain function/prevent disabilities (e.g., prevent joint damage).
- Prevent adverse effects of treatment.
- Foster normal psychological and social development.
Medication Strategy
- 1st Line: NSAIDs (e.g., Naproxen, Ibuprofen)
- Preferred for mild disease and symptomatic relief.
- 2nd Line: For Moderate/Severe cases or Mild cases with continuing active disease:
- csDMARDs: (e.g., Methotrexate).
- Biologic Agents: (e.g., Infliximab, Rituximab, Anakinra, Tocilizumab).
- Glucocorticoids.
Remission Criteria
Criteria for complete remission:
- No inflammatory joint pain
- No morning stiffness
- No fatigue
- No synovitis
- No progression of damage (sequential radiographic exams)
- No elevation of ESR and CRP