Other Pediatric Bacterial Infections
Chlamydia trachomatis
- Chlamydia trachomatis is an obligate intracellular bacteria.
- Transmission: Perinatal transmission (most important in pediatrics) occurs when an infected mother transmits bacteria to the infant during passage through birth canal. Risk: 30–50% of exposed infants. Rarely: postnatal transmission via caregivers.
Manifestations
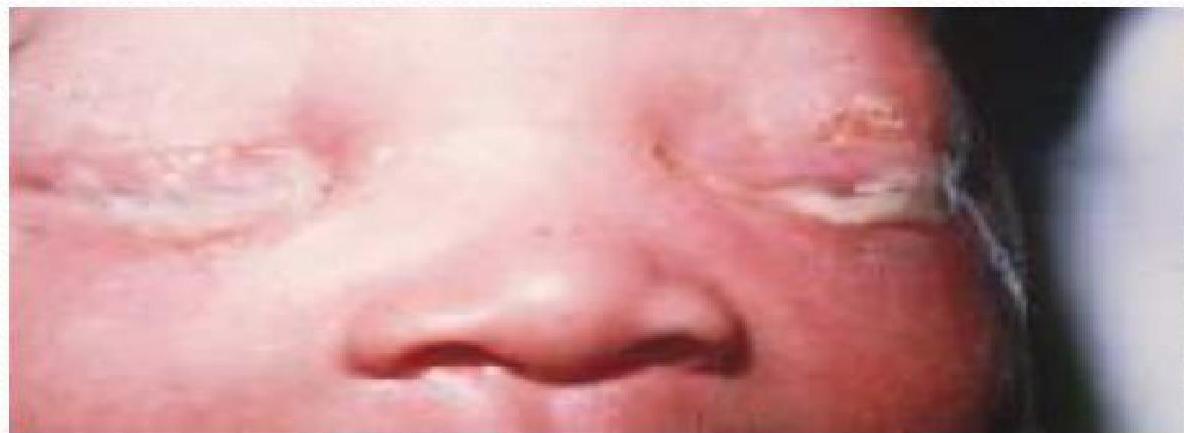
- Ophthalmia neonatorum (Neonatal conjunctivitis):
- Onset: 5–14 days after birth (later than gonococcal).
- Symptoms: eye discharge (watery to mucopurulent), eyelid swelling, conjunctival hyperemia. If untreated → risk of corneal damage and scarring.
- Chlamydial pneumonia:
- Onset: 2–12 weeks of age.
- Features: Afebrile pneumonia with staccato cough, tachypnea, nasal congestion. Inspiratory crackles, hyperinflated chest. Often associated with conjunctivitis history.
- Labs: eosinophilia (up to 400–500 cells/μL).
- Other: Otitis media, pharyngitis, though less common.
Diagnosis and Treatment
- Diagnosis: Conjunctival / nasopharyngeal swabs → Nucleic acid amplification test (NAAT) (gold standard). Culture (less used now). Chest X-ray in pneumonia: hyperinflation, bilateral interstitial infiltrates.
- Treatment: Oral erythromycin (50 mg/kg/day divided 6 hourly for 14 days). Alternative: Oral azithromycin (20 mg/kg once daily for 3 days). Topical therapy alone is not sufficient.
- Prevention: Screening and treatment of pregnant women. Prophylactic eye drops at birth do not prevent chlamydial conjunctivitis (they mainly prevent gonococcal infection).
Gonococcal
Chlamydia Trachomatis

Neisseria Gonorrhoeae
- N. gonorrhoeae infection in a newborn usually involves the eyes (Gonococcal Ophthalmia Neonatorum).
- Transmission: During passage through the birth canal.
- Features: Usually present within the first 5 days (2 – 5 days) of life. Characterized initially by a clear, watery discharge, which rapidly becomes purulent. Marked conjunctival hyperemia and eye swelling.
- Complications: Untreated infections can spread to the cornea (keratitis) and anterior chamber of the eye causing corneal perforation and blindness.
Recommended Treatment
- First line treatment is ceftriaxone 25-50 mg/kg single dose IV or IM.
- Infants with gonococcal ophthalmia should receive eye irrigations with saline solution at frequent intervals.
- Infants should be hospitalized and evaluated for disseminated disease (sepsis, arthritis, meningitis and others sexually transmitted diseases).
- Prevention: Topical prophylaxis (Ophthalmic ointment) with erythromycin or tetracycline is recommended for all newborns.
Neonatal Sepsis
Classification by Age of Onset
- Early-onset sepsis: usually acquired before or during delivery usually within the first 72 hr (up to the end of the 1st wk). Source is usually maternal. Usually multisystemic.
- Late-onset sepsis: after 72 hr (4 - 28) of life. Usually due to either nosocomial or community-acquired infection. Multisystemic or localized.
- Very-late-onset sepsis: after (>28 days in preterm/VLBW infants still in NICU). Organisms are usually multidrug resistant.
Risk Factors for Early-Onset Sepsis (within 72 hr)
- Maternal: Maternal features of sepsis or chorioamnionitis; Prolonged rupture of the membrane (> 18 hr); Prolonged labor(more than 12 hours); Frequent vaginal examinations; GBS colonization; Previous infant with early onset GBS disease; Inadequate antibiotic administration before delivery.
- Neonatal: Prematurity and LBW; infants that need resuscitation at birth; Invasive procedures (monitoring, respiratory support); Males > 4 times than females; black infants > white; Improper hand washing. (doctors ,nurses family members ..etc).
Clinical Features
Neonates may have nonspecific signs or focal signs initially.
- General: “not doing well”, temperature instability (fever or hypothermia), poor feeding and edema.
- Respiratory: Apnea, dyspnea, tachypnea, retractions, flaring, grunting, cyanosis.
- CVS: Pallor, mottling, cold, clammy skin, tachycardia, bradycardia, hypotension.
- GIT: Abdominal distention, vomiting, diarrhea, HSM.
- CNS: Irritability, lethargy, tremors, seizures, hyporeflexia, hypotonia, abnormal Moro reflex, bulging fontanel.
- Hematologic: Jaundice, splenomegaly, pallor, petechiae, purpura, bleeding.
- Renal: Oliguria.
Organisms
- Early Onset: GBS, E.coli, Listeria monocytogenes, HSV, Chlamydia trachomatis.
- Late Onset: Coagulase negative staphylococci, Pseudomonas, Klebsiella, Fungal infections (e.g. candida albicans).
- Late-Onset Presentations: Meningitis, Lower respiratory tract infection, UTI, Skin infection, Gastroenteritis, Osteomylitis, Systemic candidates.
Investigations (Septic Screen)
- CBP & Blood film.
- CRP & ESR.
- Blood culture (obtain before antibiotics).
- CSF exam & culture (important if meningitis suspected).
- GUE & culture.
- CXR, if pneumonia is suspected.
- PCR or DNA testing for specific infections.
Management
It is generally involve parenteral antibiotics & supportive care:-
- Antibiotics: Given IV immediately after blood culture.
- Empirical: Ampicillin + Aminoglycoside (gentamycin) or 3rd generation Cephalosporins.
- Staph: anti-staphylococcal penicillin or Vancomycin.
- Anaerobic: metronidazole or clindamycin.
- Supportive: Fluids & electrolytes, correction of hypoglycemia & acidosis. Ventilatory support (O₂ & humidification). Management of seizure, jaundice, & DIC. Trial of IVIG, Granulocyte transfusion. (to abolish sepsis induced neutropenia ) .
Complications
- Systemic: Shock. HF, respiratory failure, pulmonary hypertension, ARF, liver dysfunction, cerebral edema & thrombosis, adrenal hemorrhage, BM dysfunction, and DIC.
- Meningitis: ventriculitis, cerebritis, and brain abscess.
- Bacteremia: endocarditis, septic emboli, abscess formation, septic arthritis, and osteomyelitis.
- Candidemia: vasculitis, endocarditis, endophthalmitis, abscesses in kidneys/liver/lungs/brain.
Prevention
- Maternal immunization against preventable intrauterine infections .
- Intrapartum penicillin to the mother can prevent perinatal and postnatal GBS infections .
- Aggressive treatment of chorioamnionites .
- Prevention of nosocomial infection .
- Prophylactic administration of fluconazole during the first six weeks of life