Specific Pathogens (TORCHS)
Toxoplasmosis
- Caused by protozoan, toxoplasma gondii, an intracellular protozoa parasite.
- Domestic cat is the definitive host with infection via:
- Ingestion of oocysts (uncocked meats, unwashed fruits and vegetables).
- Contact with oocysts in feces or soil.
- Transmission occurs when a non-immune mother acquires primary infection during pregnancy, and the parasite crosses the placenta.
- Infection of the mother in early pregnancy: low risk of transmission rate (10–15%) but severe disease in the fetus.
- Infection of the mother in late pregnancy: high risk of transmission rate (60–90%) but milder disease.
Pathophysiology
- Parasite invades the placenta → enters fetal circulation.
- Causes tissue cysts and inflammation in brain, eye, and other organs.
- Fetal immune system is immature → severe manifestations.
Clinical Manifestations
- Most (70 – 90%) are asymptomatic at birth.
- Classic triad of symptoms:
- Chorioretinitis.
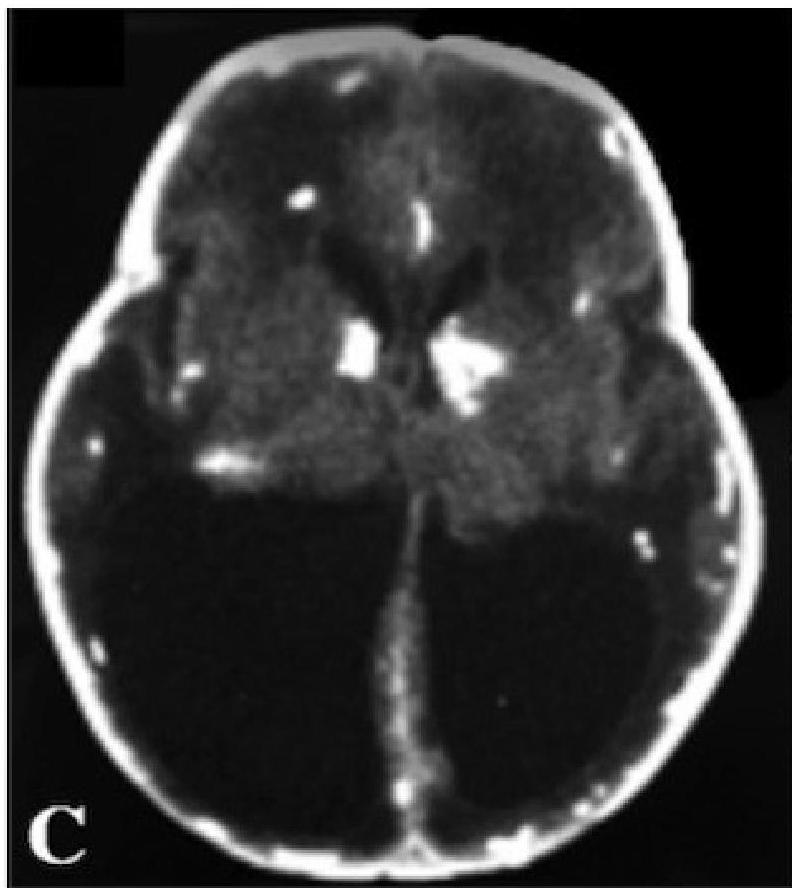
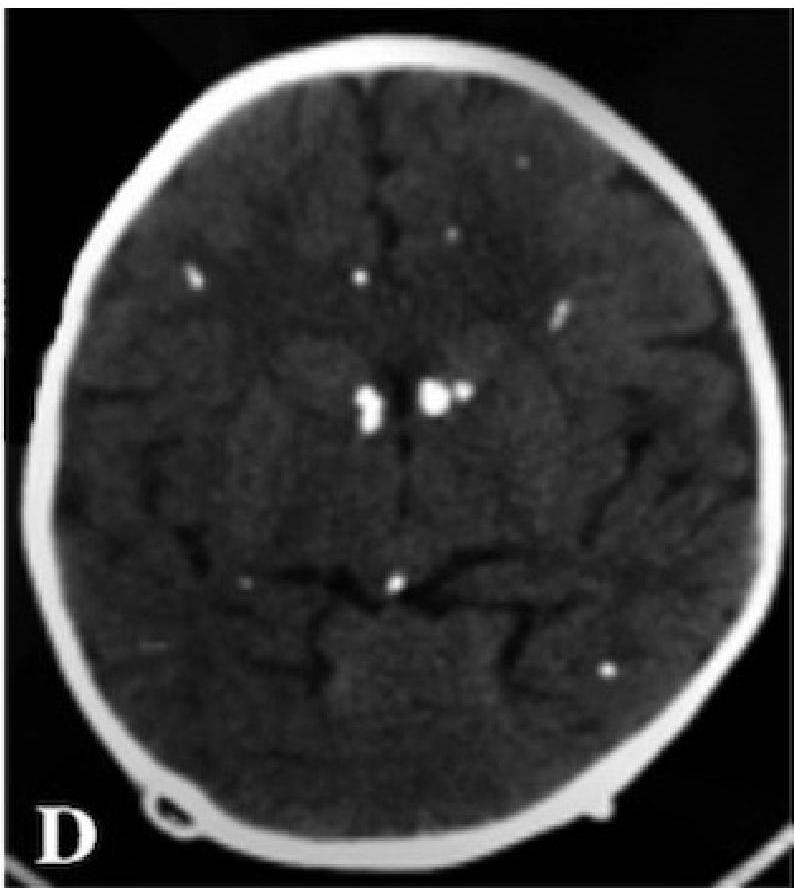
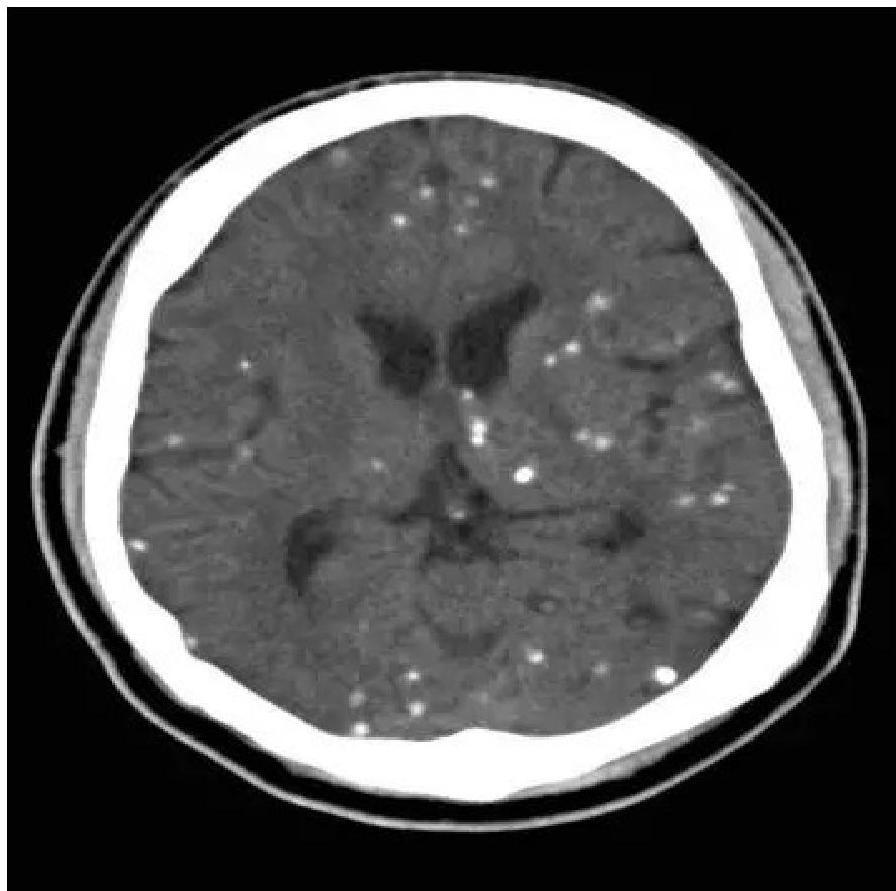
- Hydrocephalus.
- Intracranial calcification (diffuse, not periventricular like CMV).
- Other symptoms include fever, rash, HSM, microcephaly, seizures, jaundice, thrombocytopenia and lymphadenopathy.
- Initially asymptomatic infants are still at high risk of developing abnormalities especially chorioretinitis.
Visual Evidence - Chorioretinitis of congenital toxoplasmosis
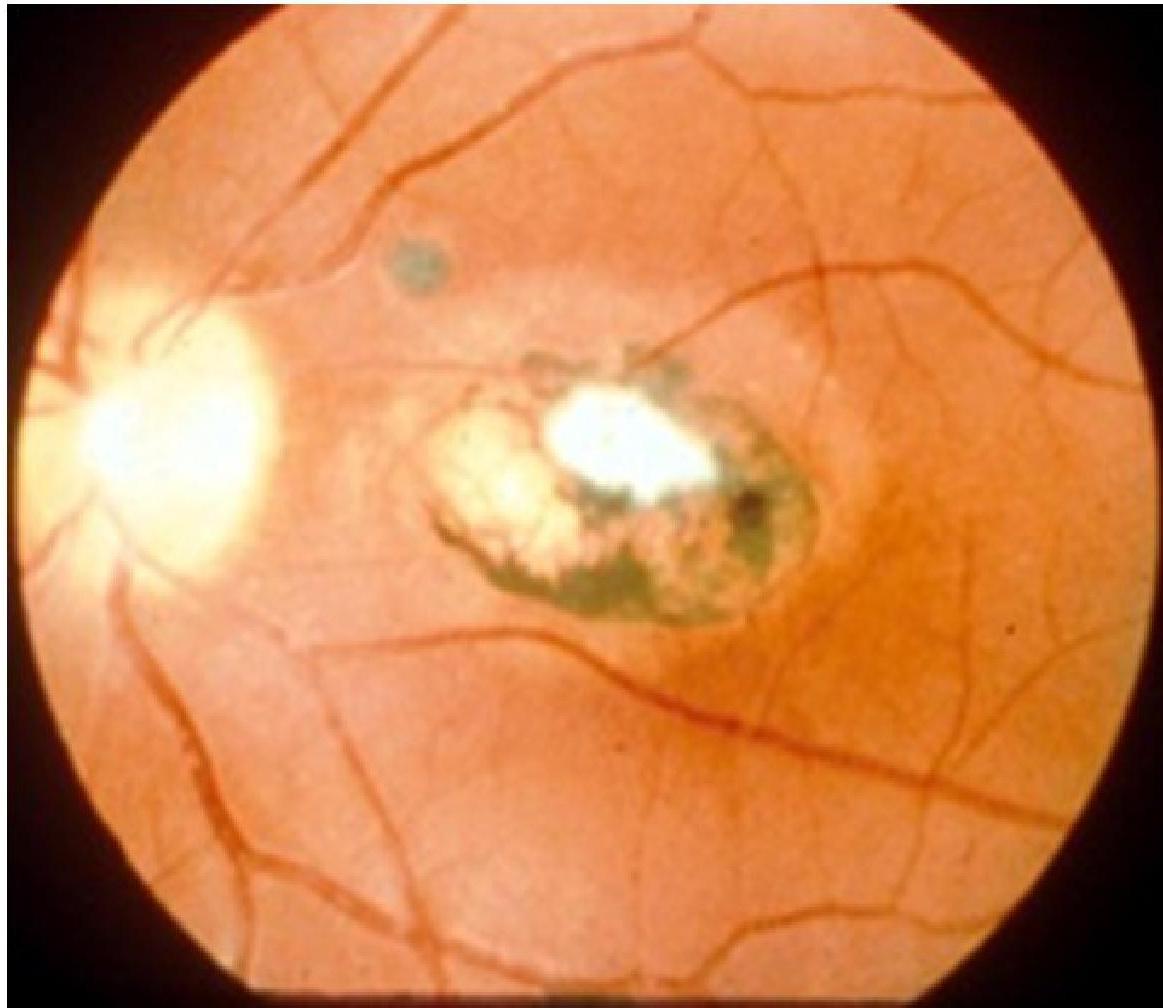
Congenital Toxoplasmosis
Diagnosis
- Maternal IgG test indicates past or chronic infection.
- Fetal diagnosis:
- Amniotic fluid PCR for T. gondii DNA.
- Ultrasound: hydrocephalus, intracranial calcifications, HSM growth restriction.
- Neonatal diagnosis:
- Serology (persistent IgG after 12 months = congenital infection).
- IgM (produced by infant, not maternal).
- Neuroimaging (CT/MRI).
- Ophthalmic exam.
Management
- Prevention: Educate pregnant women: Avoid raw/undercooked meat; Wash fruits/vegetables; Avoid handling cat litter or use gloves. Screening policies.
- Management during pregnancy: Spiramycin (reduces vertical transmission).
- If fetal infection confirmed: pyrimethamine + sulfadiazine + folinic acid (after 18 weeks gestation).
- In neonates: Combination therapy: pyrimethamine + sulfadiazine + folinic acid for 1 year.
- Supportive: Corticosteroids if severe chorioretinitis or very high CSF protein; anticonvulsants, shunt for hydrocephalus.
Syphilis
- Congenital syphilis is an infection caused by Treponema pallidum bacteria, transmitted vertically from mother to fetus via the placenta or rarely at birth through contact with maternal genital lesions.
- Risk of transmission is highest in primary and secondary maternal syphilis, decreasing with latent disease.
- Pathogenesis: Treponema pallidum crosses the placenta after ~16 weeks of gestation. Fetal infection leads to inflammation, tissue destruction, and scarring. Can result in miscarriage, stillbirth, or congenital infection.
Clinical Features
- Congenital syphilis is classified into early (<2 years) and late (>2 years).
Early Congenital Syphilis (<2 years)
- At birth may be absent (many infants appear normal).
- Manifestations:
- Snuffles (syphilitic rhinitis) is the most characteristic early feature of congenital syphilis, highly infectious.
- Maculopapular or bullous rash with desquamation (palms / soles).
- Hepatosplenomegaly, Lymphadenopathy.
- Bone changes: periostitis, osteochondritis → pseudoparalysis.
- Anemia, jaundice, thrombocytopenia.
- Failure to thrive.
Visual Evidence (Early) - snuffles in congenital syphilis

Periostitis of long bones seen in neonatal syphilis

Late Congenital Syphilis (>2 years)
- Results from untreated or inadequately treated cases.
- Classic triad:
- Interstitial keratitis.
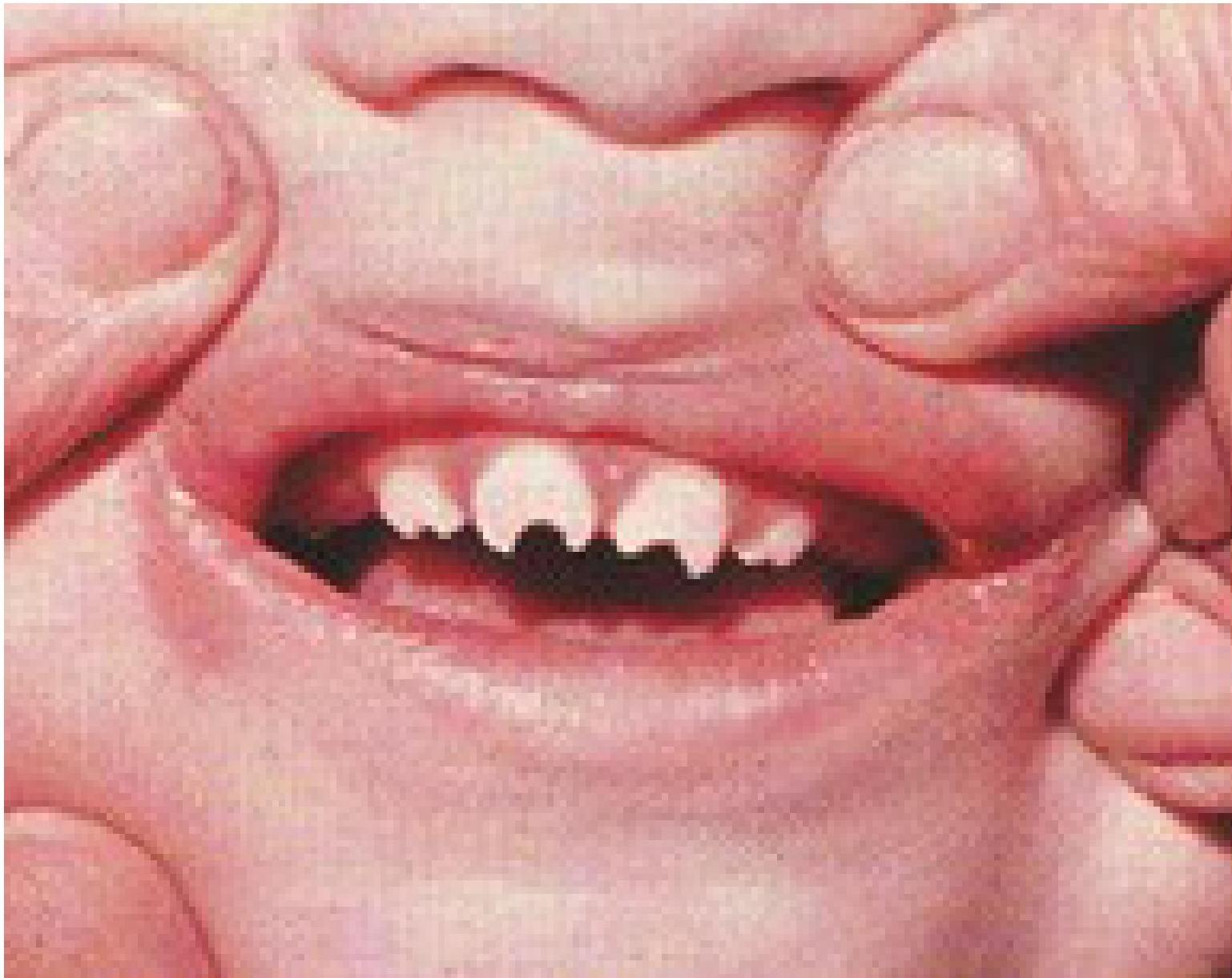
- Hutchinson teeth (peg-shaped, notched upper central incisors).
- Sensorineural deafness.
- Other stigmata:
- Frontal bossing, saddle nose deformity.
- Saber shins, Clutton’s joints (painless knee effusion).
- Enlarged sternoclavicular joint.
Visual Evidence (Late) - Hutchinson teeth – late result of congenital syphilis
Diagnosis and Treatment
- Maternal testing: VDRL, RPR (Rapid Plasma Reagin test), others – treponemal tests.
- Neonatal testing:
- Serology: VDRL/RPR (for IgG and IgM); Treponemal tests.
- PCR or dark-field microscopy of lesions.
- CSF: for neurosyphilis.
- Radiology: metaphyseal changes, periostitis.
- Complications: Miscarriage or stillbirth, Neonatal death, Severe physical deformities.
- Treatment: First-line: Penicillin G (the only effective treatment in pregnancy and infants).
- Infants with proven/highly probable disease → IV crystalline penicillin for 10 days.
- Asymptomatic infants with uncertain exposure → Benzathine penicillin IM (single dose).
- Penicillin allergy: Desensitization + penicillin (no alternatives during pregnancy).
- Prevention: Screening of all pregnant women (at first visit, third trimester, and delivery in high-risk areas). Early maternal treatment prevents transmission.
Rubella
- Congenital Rubella Syndrome (CRS) results from maternal rubella infection during pregnancy, especially in the first trimester.
- Rubella virus is a togavirus (RNA virus).
- Fetal infection risk and severity, depend on gestational age at maternal infection.
- Epidemiology: Rubella is rare in countries with MMR vaccination.
- Risk of fetal infection:
- First 12 weeks: up to 90%.
- 13–16 weeks: ~25%.
- After 20 weeks: very low risk.
Pathophysiology
- Virus crosses placenta → interferes with organogenesis.
- Causes cell necrosis, vasculitis, and impaired cell division, leading to congenital anomalies.
Clinical Features of CRS
- Classic Triad:
- Sensorineural deafness (most common permanent feature).
- Congenital heart disease (PDA, pulmonary artery stenosis, VSD).
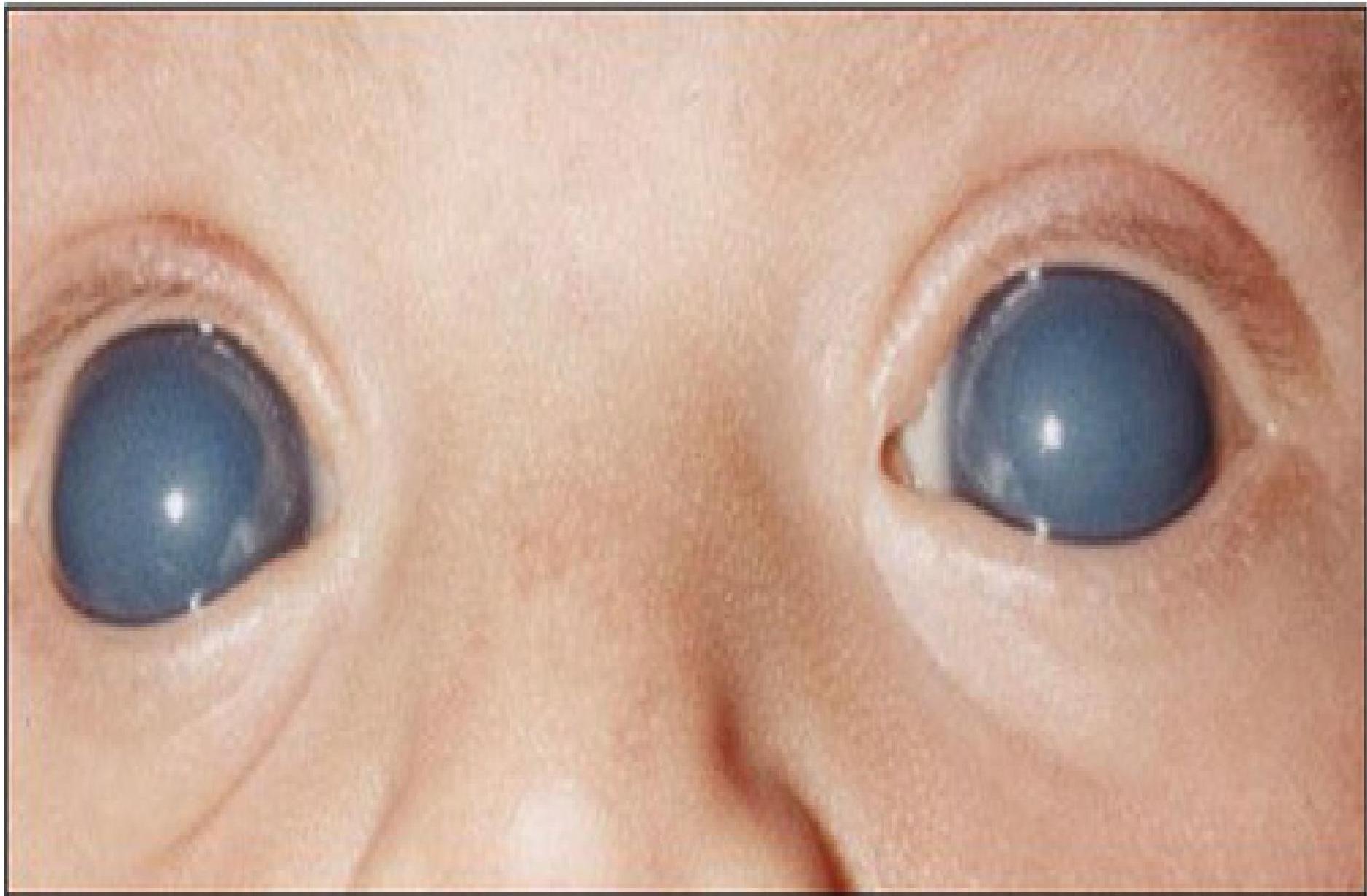
- Eye defects (cataracts, glaucoma, retinopathy, microphthalmia).
- Other Manifestations: Growth restriction, low birth weight, microcephaly, developmental delay, seizures.
- Systemic: HSM, thrombocytopenic purpura (“blueberry muffin rash”).
- Bone: Bone radiolucencies (long bones).
Blueberry muffin spots


Bilateral cataract in congenital rubella
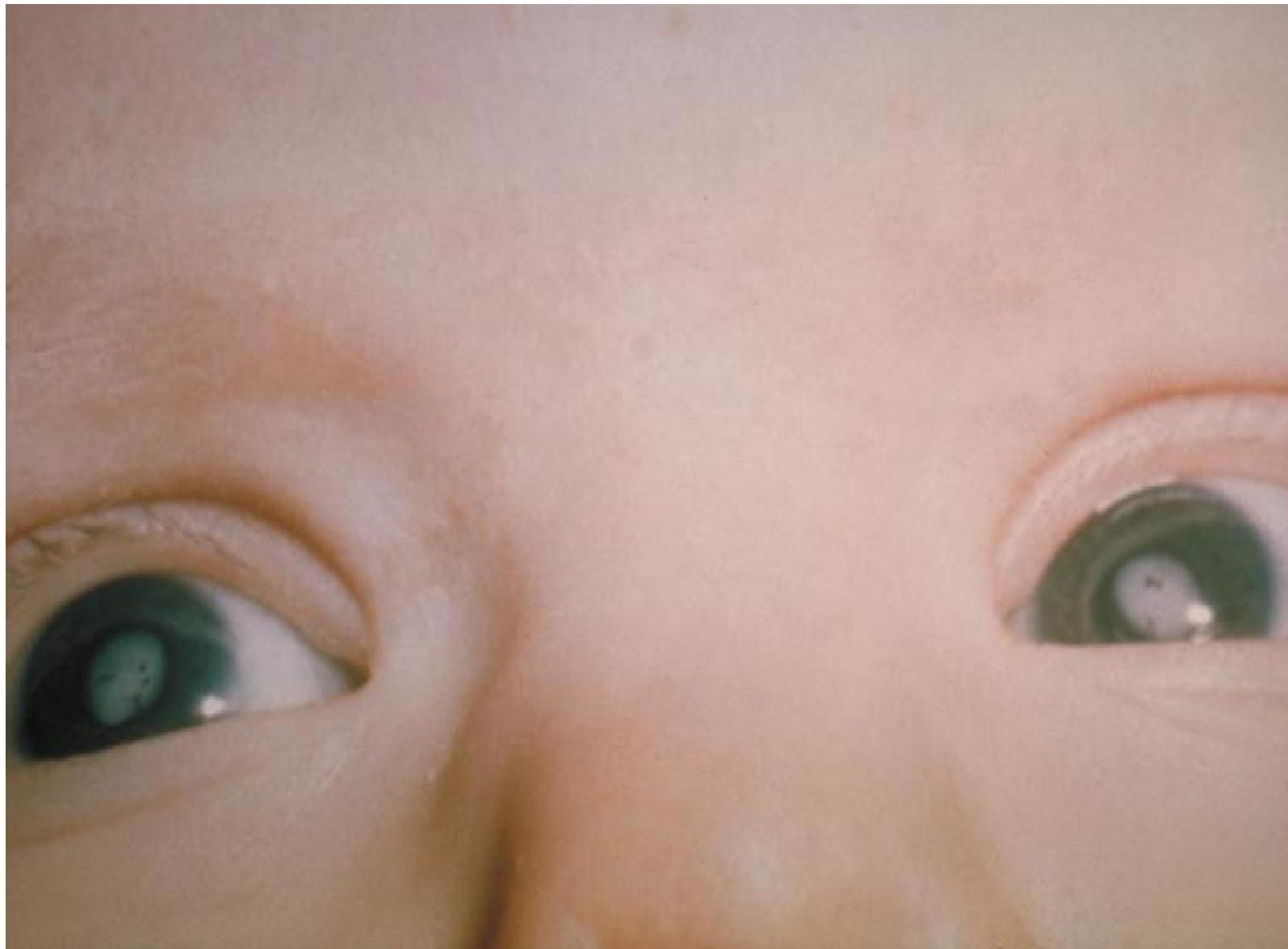
Bilateral glaucoma in congenital rubella
Diagnosis and Management
- Lab tests: Rubella-specific IgM in neonate; Persistence of IgG beyond 6 months; PCR for rubella RNA.
- Management: No specific antiviral treatment. Supportive & multidisciplinary: Cardiology for CHD, Ophthalmology for cataracts/glaucoma, Audiology for deafness, Early developmental support.
- Prevention: MMR vaccination (live attenuated vaccine): Contraindicated in pregnancy. Women of child bearing age should be immune before conception. Pregnant non-immune women exposed to rubella → consider immunoglobulin, but protection is limited.
Cytomegalovirus (CMV)
- Cytomegalovirus (CMV) is a member of the Herpesviridae family.
- It is the most common congenital viral infection worldwide.
- Incidence: ~0.2–2% of all live births.
- Major cause of sensorineural hearing loss (SNHL) and neurodevelopmental impairment.
- Transmission: Maternal primary infection during pregnancy → highest risk to fetus.
- Routes: (a) Transplacental (most significant); (b) Intrapartum (contact with infected genital secretions); (c) Postnatal (through breast milk).
- Risk of transmission: 30–40% in primary maternal infection, lower in reactivation.
Pathophysiology
- CMV infects multiple organs → especially CNS, liver, and hematopoietic system.
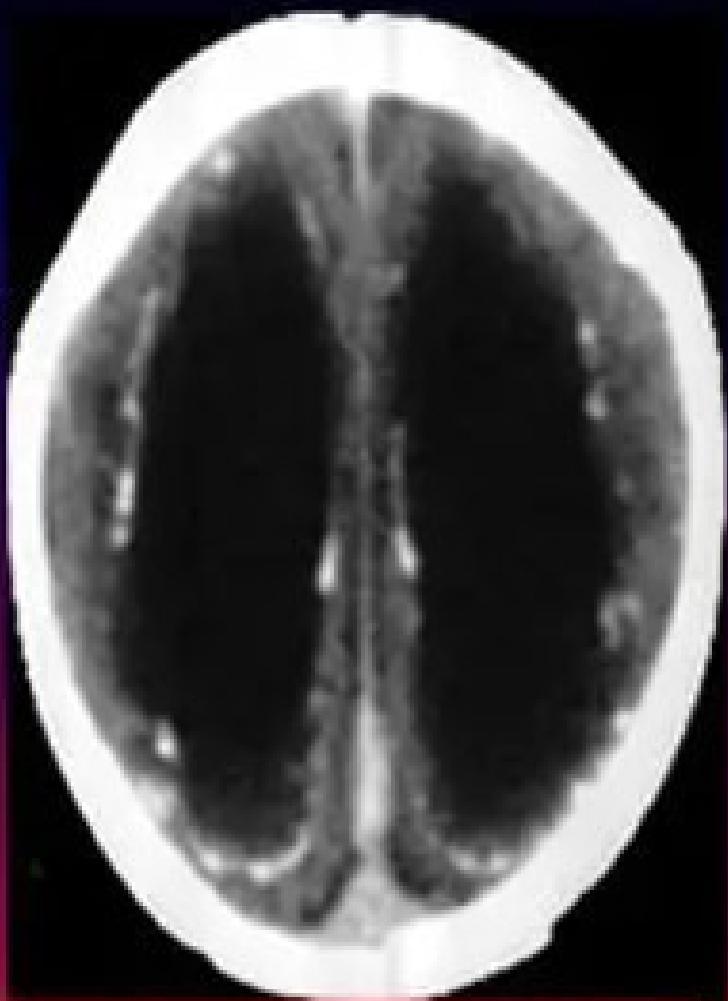
- Leads to: Inflammation, Cellular destruction, Calcification (especially in periventricular areas of the brain).
Clinical Features
- Only 10–15% of infected neonates are symptomatic at birth (> 85 % are asymptomatic at birth).
- Symptomatic congenital CMV at birth:
- Growth restriction (IUGR).
- Neurological: Microcephaly, Seizures, Intracranial calcifications (classically periventricular).
- Hepatic: Hepatosplenomegaly, Jaundice, elevated liver enzymes.
- Hematologic: Thrombocytopenia → “blueberry muffin” rash.
- Other: Chorioretinitis, Sensorineural hearing loss (may present later).
- Asymptomatic at birth but at risk of sequelae: - Sensorineural hearing loss (most common long-term complication), - Neurodevelopmental delay, - Vision impairment.
Ventriculomegaly and calcification of congenital CMV
Diagnosis and Management
- Diagnosis: Confirmed by detection of CMV DNA (by PCR) in urine, saliva, or blood collected within the first 3 weeks of life (Gold standard test).
- Imaging: Cranial ultrasound/CT → periventricular calcifications, ventriculomegaly.
- Labs: Thrombocytopenia, elevated transaminases.
Differential Diagnosis Other congenital infections (TORCH):
-
Toxoplasmosis → diffuse intracranial calcifications.
-
Rubella → cataracts, PDA, deafness.
-
Syphilis → snuffles, bone lesions.
-
HSV → vesicular lesions, encephalitis.
-
Management: Supportive care for complications (platelet transfusion, anti-epileptics, nutritional support).
-
Antiviral therapy: Oral valganciclovir (or IV ganciclovir if severe). Indicated for symptomatic infants (especially CNS involvement). Duration: usually 6 months.
-
Early intervention (audiology, physiotherapy).
-
Prognosis:
- Symptomatic infants: high risk of mortality (10–30%) and severe disability
- long-term sequelae eg: sensorineural hearing loss, intellectual disability, cerebral palsy, vision loss.
- Asymptomatic: ~10–15% may develop hearing loss later.
-
Prevention:
- No vaccine available.
- Good hygiene in pregnant women (handwashing after handling diapers). Avoiding sharing food/drinks with toddlers.
Congenital Herpes Simplex Virus (HSV)
- Congenital HSV infection occurs when a neonate acquires HSV (type 1 or type 2) during the perinatal period, rarely prenatally.
- HSV-2 is more common (70–80%) than HSV-1 in congenital or neonatal infections.
- Epidemiology: Incidence: ~1 in 3,000 to 1 in 20,000 live births.
- Transmission: Intrauterine (rare, <5%): transplacental; Peripartum (majority, ~85%): passage through birth canal; Postnatal (10%): direct contact with caregivers.
- Risk Factors: - Maternal primary genital HSV-2 infection in the third trimester, - Prolonged rupture of membranes, - Instrumental delivery (scalp electrodes, forceps), - Prematurity.
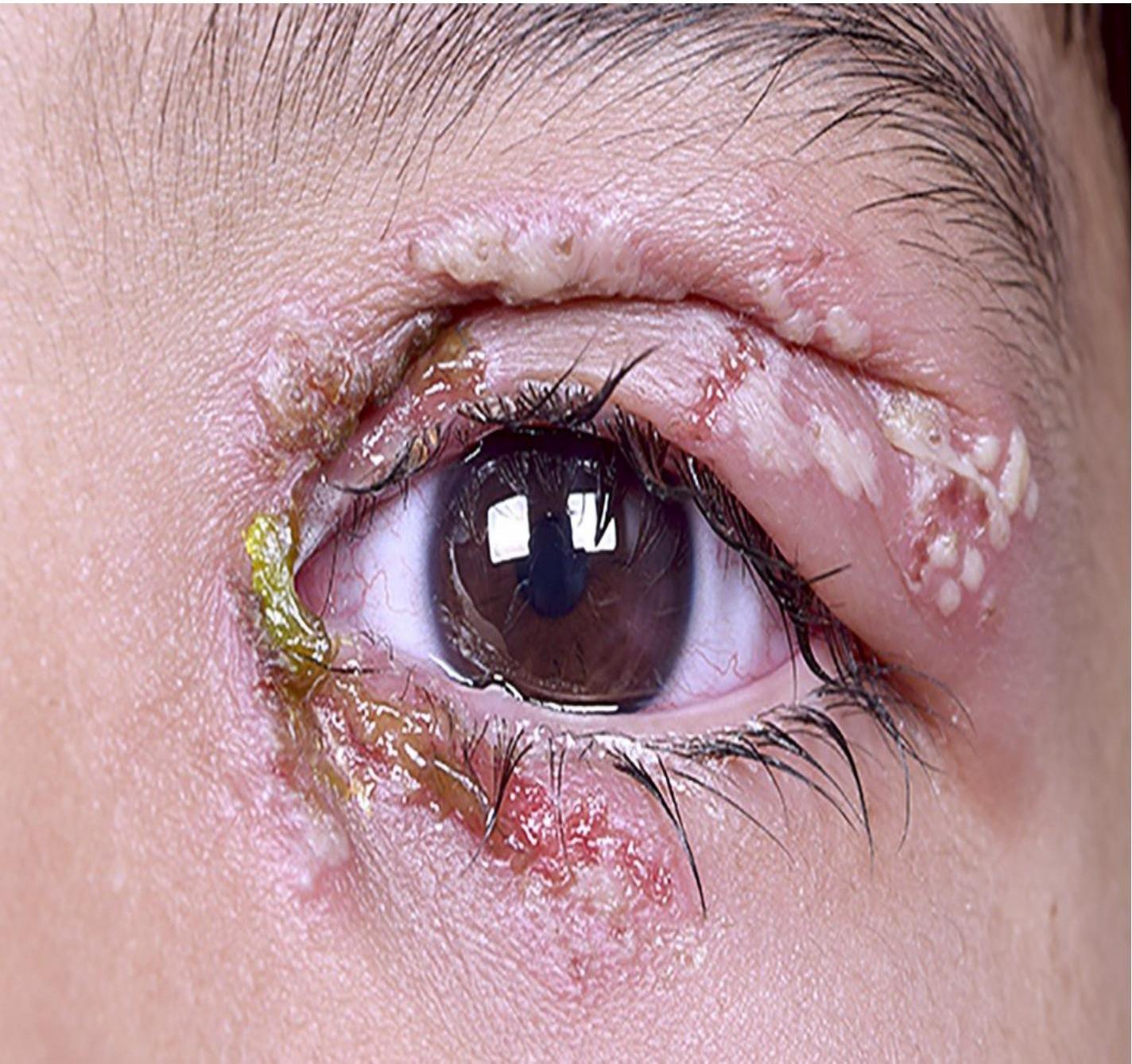
Clinical Presentations (appearing usually between day 5–14 of life)
- Skin, Eyes, Mouth (SEM disease):
- Vesicular lesions on skin.
- conjunctivitis, keratitis.
- oral ulcers.
- No CNS/systemic involvement. Accounts for ~45% of cases. Good prognosis with treatment.
- Central Nervous System (CNS disease):
- Lethargy, seizures, irritability, bulging fontanelle, poor feeding.
- Temporal lobe involvement in HSV encephalitis.
- CSF: pleocytosis, elevated protein, normal glucose. HSV PCR from CSF diagnostic. 30% mortality.
- Disseminated disease:
- Multi-organ involvement: liver, lungs, adrenals, CNS.
- Presents with sepsis-like picture (shock, hepatitis, coagulopathy).
- Accounts for ~25% of cases.
- Highest mortality (up to 90% untreated), high morbidity (neurological sequelae).



Diagnosis and Management
- Diagnosis: - PCR for HSV DNA from lesions, blood, CSF (gold standard). - Culture of lesions. - Elevated liver enzymes in disseminated disease. - Neuroimaging: temporal lobe involvement in HSV encephalitis.
- Management: - IV Acyclovir: mainstay of treatment. Dose: 60 mg/kg/day in 3 divided doses for 14–21 days (longer for CNS/disseminated). - Supportive care (anticonvulsants, ventilation, fluids). - Long-term suppressive oral acyclovir for 6 months may reduce recurrence and improve neurodevelopment.
- Prevention:
- Identify pregnant women with active genital HSV.
- Cesarean section recommended if lesions present at delivery.
- Avoid invasive monitoring during labor. Postnatal: avoid kissing/handling neonates with active cold sores.
- Prognosis:
- SEM disease: excellent if treated.
- CNS disease: 70% survivors with neurologic impairment.
- Disseminated disease: high mortality without treatment, ~30% with therapy.