CONSTIPATION
Constipation is the infrequent or difficult passage of hard stools that may cause discomfort or distress.
For children (Rome IV Criteria), constipation is diagnosed if two or more of the following are present for at least 1 month (in infants or toddlers) or 2 months (in older children):
- ≤2 defecations per week.
- ≥1 episode of fecal incontinence per week (after toilet training).
- History of excessive stool retention.
- Painful or hard bowel movements.
- Large diameter stools.
- Presence of a large fecal mass in the rectum.
Common pediatric problem (affects ~3–5% of children).
Peak incidence: during toilet training and school age.
Causes
- Functional (or idiopathic) constipation. 90 – 95% of cases.
- Organic Constipation.
Functional (or idiopathic) constipation
Also known as fecal withholding. Can be differentiated from organic constipation by history and physical examination.
It is typically starts after the neonatal period, and is the most common cause of constipation beyond the neonatal period (90 – 95% of cases).
Usually there is intentional or subconscious withholding of stool.
Predisposing factors include
A) Psychosocial/ stress and behavioral factors such as:
- Initiation of toilet training.
- Birth of sibling.
- Changing the school.
- Starting daycare.
- Changing the home.
- Abuse.
- Holding stool due to fear or anxiety.
B) Dietary change:
- A diet low in fiber and insufficient fluid intake.
Pathophysiology & Clinical Manifestations
- The stool becomes firm, smaller and difficult to pass, resulting in anal irritation and often an anal fissure.
- Painful bowel movements leading to voluntary withholding of defecation.
Clinical manifestations:
-
Abdominal pain.
-
Painful defecation.
-
The patient struggles to defecate.
-
There is often a history of blood in the stool with the passage of a large bowel movement.
-
No features suggestive of organic cause.
-
Encopresis is common: Voluntary or involuntary passage of feces into inappropriate places, at least once per month for three consecutive month at the age of four years.
-
Abdominal examination often demonstrates a large volume of stool palpated in the supra pubic area, with abdominal pain.
-
Rectal examination demonstrates dilated rectum filled with stool without occult blood.
-
In severe cases (Loss of appetite, poor growth and urinary incontinence and recurrent urinary tract infection).
-
Poor school performance and attendance in case of soiling.
Investigation
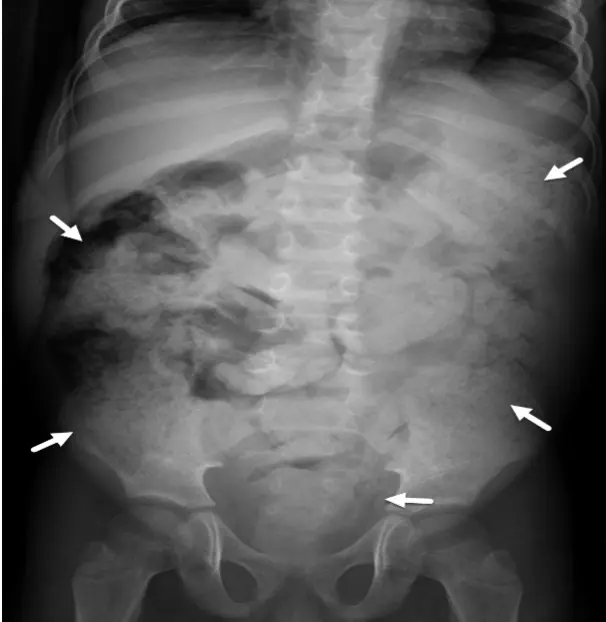
Abdominal X-ray and water soluble contrast enema shows large amount of stool in the colon. Stool may appear as mottled or glandular densities due to gas mixed with feces. Also it shows gas in the intestine and sometimes shows air fluid levels if there is obstruction.
Management of functional Constipation
-
Education and Counseling
-
Diet and life style:
- Adequate fluid intakes.
- High fiber diet.
- Encourage physical activities.
-
Behavioral management:
- Regular toileting, 5 - 10 minute on toilet after meals.
- Correct toilet position.
-
Medications:
- Disimpaction (if fecal mass present):
- Oral: Polyethylene glycol (PEG) is first-line.
- Rectal: Enemas (if oral not tolerated or failed).
- Glycerin suppository.
- Soap enema.
- Fleet enema (sodium citrate).
- Manual evacuation if all above fail (usually under general anesthesia).
- Disimpaction (if fecal mass present):
-
Maintenance Therapy:
- Osmotic laxatives: Lactulose, PEG.
- Stimulant laxatives (short-term): Senna.
- Continue for several months.
Organic constipation
Common causes include:
- Hirschsprung’s disease
- CF
- Celiac disease
- Hypothyroidism, hypercalcemia, hypokalemia
- Anal anatomic malformation
- Drugs (opioids)
- Intestinal obstruction
- Neurogenic constipation due to spinal cord anomalies or trauma and tethered cord
- Colonic obstruction or atresia
Red flags (suggestive of organic constipation)
- Early onset of constipation (first few weeks of life)
- Failure to thrive/growth failure
- Neuropathic bowel:
- Midline dimple, tuft of hair
- Decreased lower extremity tone and/or strength
- Urinary symptoms
- Anal stenosis (tight rectum)
- Hirschsprung’s disease:
- Family history of Hirschsprung’s
- Delayed passage of meconium for > 48 hr after birth in a term baby
- Abdominal distention
- Explosive stool and air from rectum on withdrawal of finger
- Signs of obstruction: bilious vomiting, severe abdominal distention
Clinical examination
Findings according to the cause eg:
- Weight or height affected.
- Course features (hypothyroidism).
- Abdominal distention fecal loading.
- Lower limbs weakness.
- Spinal examination abnormalities.
- Perianal area (fissure).
- Recatal examination, explosive stool in Hirschsprung disease.
Investigation
- X-ray, barium and abdominal ultrasound.
- TFT.
- Celiac screening.
- Sweat chloride test.
- Rectal biopsy.
Management
- According to the cause.