HIRSCHSPRUNG’S DISEASE
(CONGENITAL AGANGLIONIC MEGACOLON)
DR. ELFADIL EISA IDRIS SULIMAN Associate professor of Pediatrics and child health
- Is a developmental disorder of the enteric nervous system characterized by the absence of ganglion cells in the mucosa and mesenteric plexus.
- It is the most common cause of intestinal obstruction in neonate.
- Males more affected than females 4-1.
- There is an increase familial incidence.
- May be associated with other congenital defects e.g. Urogenital, cardiovascular, microcephaly, cleft palate, hydrocephalus and may be associated with Down syndrome, nephroplastoma ..etc.
Pathology
- Absence of ganglion cells in the bowel wall extending proximally from the anus for a variable distance. This leads to inadequate relaxation, decreased motility and bowel hypertrophy in the affected bowel segment and of the internal anal sphincter.
- Hirschsprungs disease can lead to intestinal obstruction.
- The aganglionic segment is limited to the rectosigmoid (the most common site of agangliosis) in 80% of patient.
- Approximately 10 - 15% of patients have long segment disease, and the disease extends proximal to the sigmoid colon.
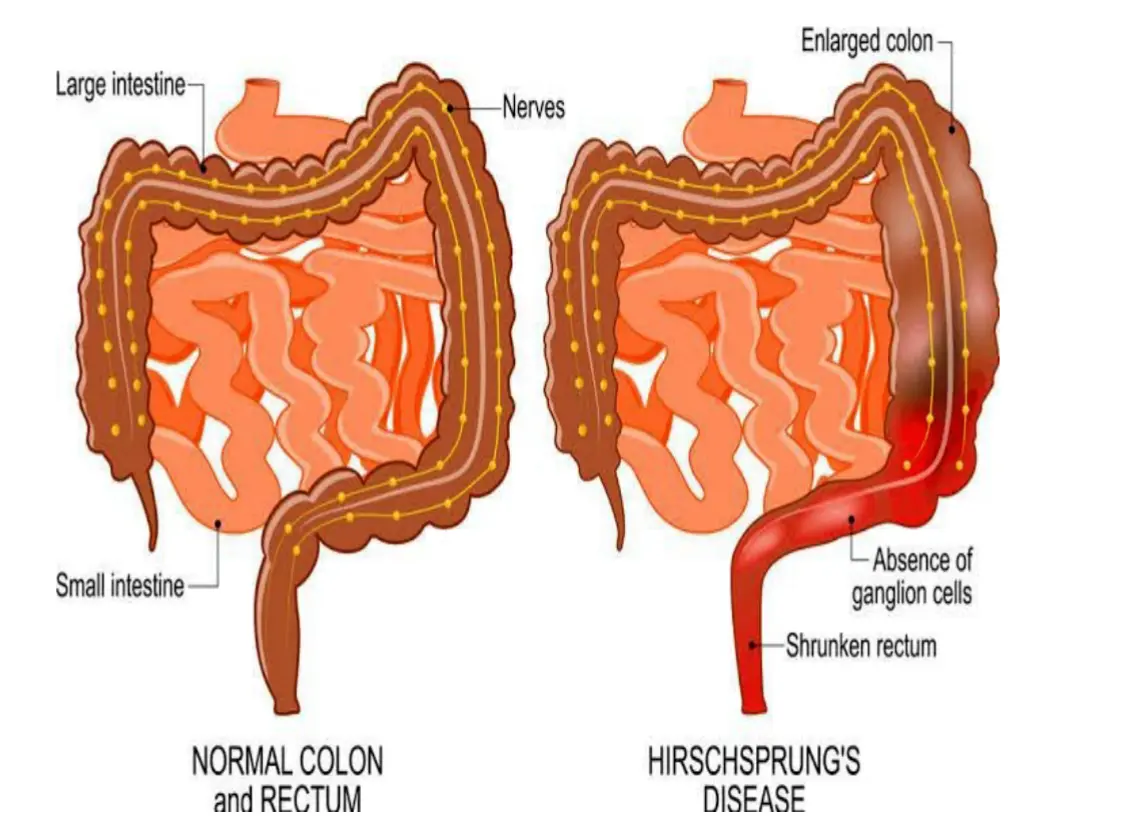
NORMAL COLON and RECTUM | Nerves | Naturally active cells | Nervous system | Enlarged colon | Absence of ganglion cells | Shrunken rectum | HIRSCHSPRUNG’S DISEASE
Clinical manifestations
In newborns:
- Delayed passage of meconium > 48 hours after birth in mature infants. It is rare in premature infants.
- Bilious vomiting.
- Abdominal distention relieved by digital rectal examination.
Older children:
- Vomiting.
- Constipation.
- Chronic abdominal distinction.
- Failure to thrive and growth failure.
Hirschsprung’s disease
Swollen, distended abdomen.



- Failure to pass stool lead to dilation of the proximal bowel and abdominal distention, so intraluminal pressure increase resulting in decrease blood flow and deterioration of the mucosal barrier.
- Stasis leads to proliferation of bacteria which can lead to enterocolitis (clostridium difficile, staph aureus and anaerobes) with associated diarrhea, sepsis & sings of bowel obstruction.
- In older children the abdomen is distended with a large fecal mass palpable in the left lower abdomen.
- Rectal examination: Demonstrates empty rectum and when the finger is removed, there may be an explosive discharge of foul - smelling feces and gas.
- Urinary retention with enlarged bladder and hydronephrosis can occur secondary to urinary obstruction.
Differential diagnosis in neonate
- Meconium plug syndrome (blockage in the colon).
- Meconium ileus (blockage in the small intestine, specifically the ileum).
- Intestinal atresia.
Diagnosis
- Clinical picture.
- FH.
- Erect abdomen X-ray.
- Barium enema: Shows a transitional zone where a market change in caliber occurs, with the dilated normal colon above and the narrowed aganglionic below (should not be done in patient suspected of having enterocolitis → perforation).
- Proximal Dilated Bowel (Normoganglionic)
- Transition Zone (hypoganglionic)
- Contracted Distal Bowel (aganglionic)


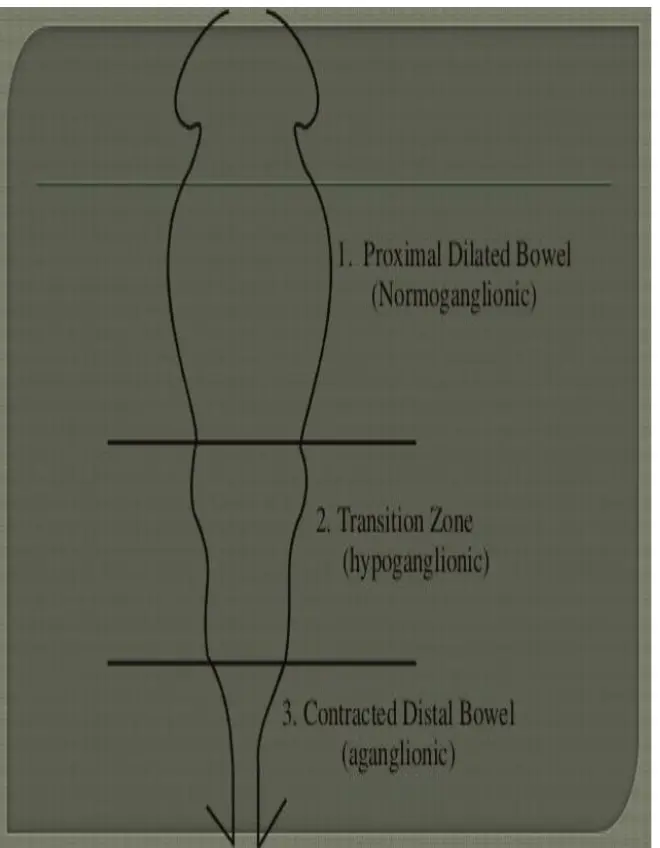
The transition zone is in the mid-descending colon.
- Anorectal manometry: It shows an absence of normal relaxation of the internal sphincter, with a reduction in the intraluminal pressure in the anal canal when the rectum is distended with a balloon.
- Rectal biopsy (gold standard for diagnosis):
- a) Suction rectal biopsy: Reduced mucosa and submucosa ganglion cells. It can be easily performance at the bedside.
- b) Full thickness rectal biopsy: The definitive diagnosis is confirmed by full-thickness rectal biopsy, demonstrates absence of ganglionic cells.
- The diagnostic yield of the full-thickness rectal biopsy is significantly better than suction biopsy.
Histological findings
- Absent ganglion. Acetylcholinesterase staining shows hypertrophied nerve trunks, throughout the lamina propria and muscularis propria layers of the bowel wall.
Management
- NPO, NGT and IV fluid.
- Correction of electrolytes.
- Antibiotics before the operation.
- Removal of the part of the colon that lacking nerve (aganglionic colon) and connected the healthy bowel to the rectum (pull-through operation).
Post operation complication
- Constipation.
- Recurrent enteroclitis.
- Stricture.
- Prolapse.
- Perianal abscess.
- Fecal soiling.