DIABETES MELLITUS TYPE 1
Dr Faten Zaidan
Pathophysiology
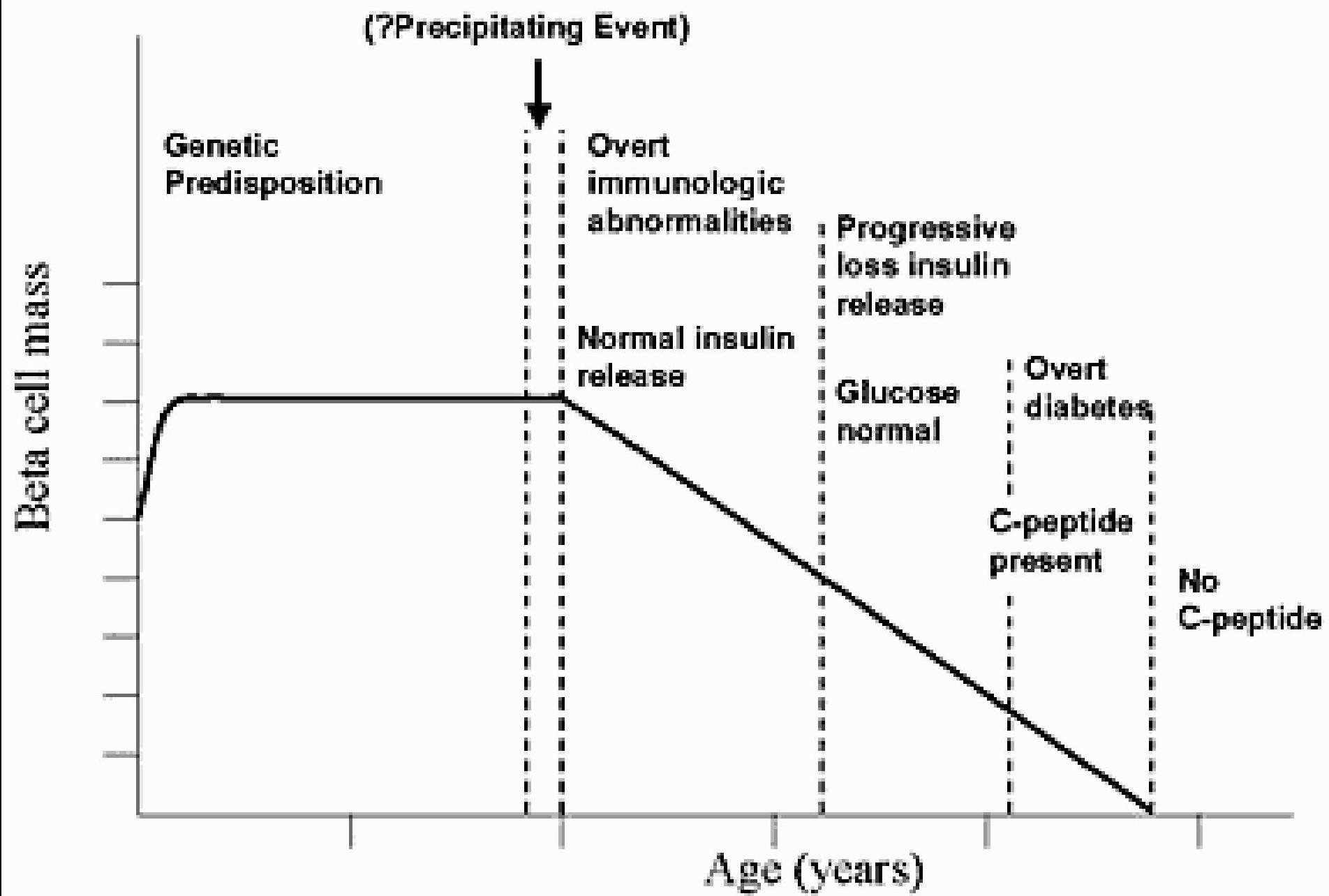
- Immune or non-immune destruction (autoantibodies) of insulin secreting beta cells of pancreas leading to severe or absolute deficiency of insulin and required exogenous insulin
- First there will be partial deficiency of insulin:
- decreased lipogenesis, energy expenditure, weight loss, fatigability, classic triad
- As more insulin is getting deficient reaching into absolute insulin deficiency: there will be increased lipolysis and production of ketone bodies resulting in DKA
DM type I may also be idiopathic, syndromic or due to infections
”Stages” in Development of Type 1A Diabetes
Secondary Causes of DM
- Cystic fibrosis – related diabetes
- Trauma – pancreatectomy
- Pancreatitis
- Congenital rubella
- Cytomegalovirus
- Endocrine tumors
- Neonatal diabetes
- Genetic syndrome such as Down Syndrome, Prader Willi, Turner, Klinefelter
- Medications such as l-asparaginase, phenytoin, diazoxide, nicotinic acid, etc
Initial Clinical and Laboratory Findings in New-Onset Type 1 Diabetes
Table 1 – Initial clinical and laboratory findings in new-onset type 1 diabetes in children and adolescents
| Clinical findings | |
|---|---|
| Fatigue | |
| Weight loss | |
| Polyuria | |
| Polydipsia | |
| Secondary nocturnal enuresis | |
| Blurred vision | |
| Urinary tract infection | |
| Vaginal candidiasis | |
| Abdominal pain | |
| Vomiting | |
| Ketone breath | |
| Kussmaul respiration | |
| Laboratory findings | |
| Hyperglycemia | |
| Glucosuria | |
| Ketonuria | |
| Metabolic acidosis | |
| Elevated blood urea nitrogen level | |
| Elevated serum β-hydroxybutyrate level | |
| Low C-peptide level | |
| Elevated antibody levels (anti-glutamic acid decarboxylase, anti-islet cell, anti-insulin) |
Diagnostic Criteria
- Symptoms of diabetes
- Blood test:
- Random plasma glucose 200 mg/dl (11.1 mmol/l), OR
- Fasting plasma glucose 126 mg/dl (7 mmol/l), OR
- 2-hour plasma glucose 200 mg/dl during an oral glucose tolerance test.
HbA1c >= 6.5%
- For monitoring therapy
- For diagnosing DM
Impaired Glucose Tolerance Test
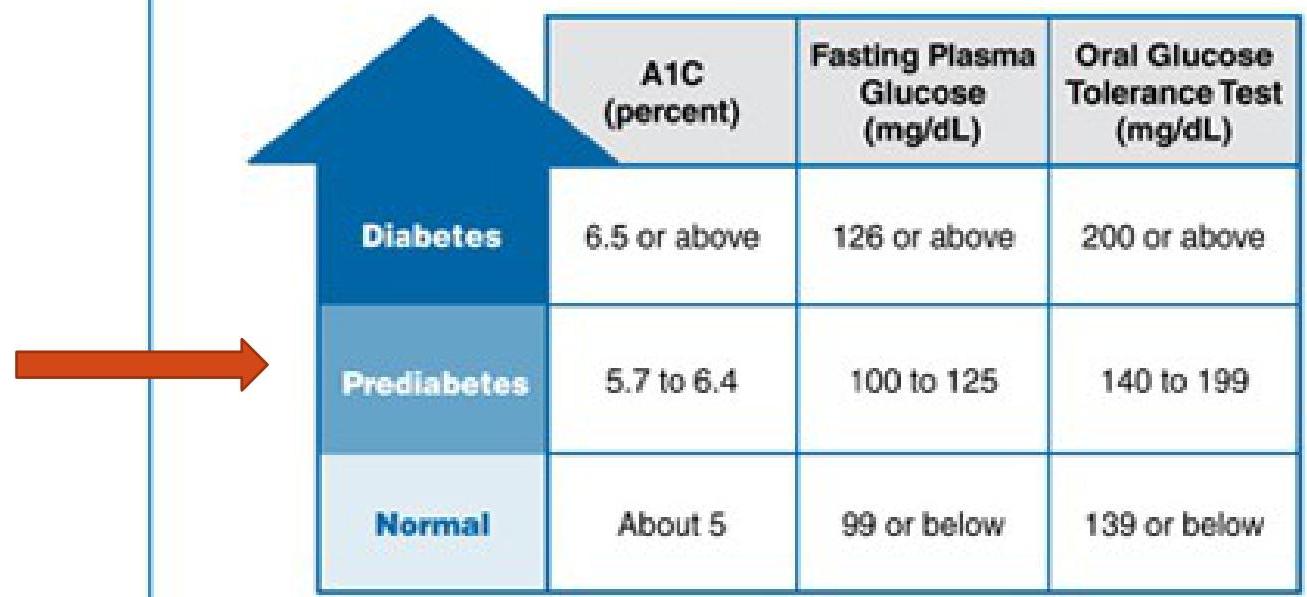
Blood Test Levels for Diagnosis of Diabetes and Prediabetes
Definitions: mg = milligram, dL = deciliter
For all three tests, within the prediabetes range, the higher the test result, the greater the risk of diabetes.
Conversion:
- To convert mmol/l into mg/dl, multiply by 18
- 7 mmol/l × 18 = 126 mg/dl
- 11.1 mmol/l × 18 = 200 mg/dl
Approach for Newly Diagnosed DM I
Blood investigations:
- Random blood glucose
- Blood ketones
- Urea and electrolytes (to assess dehydration and electrolyte disturbance)
- Blood gas (to assess for acidosis)
- Thyroid function test
- Celiac screen
- Diabetes related autoantibodies: GAD autoantibodies and islet cell antibodies
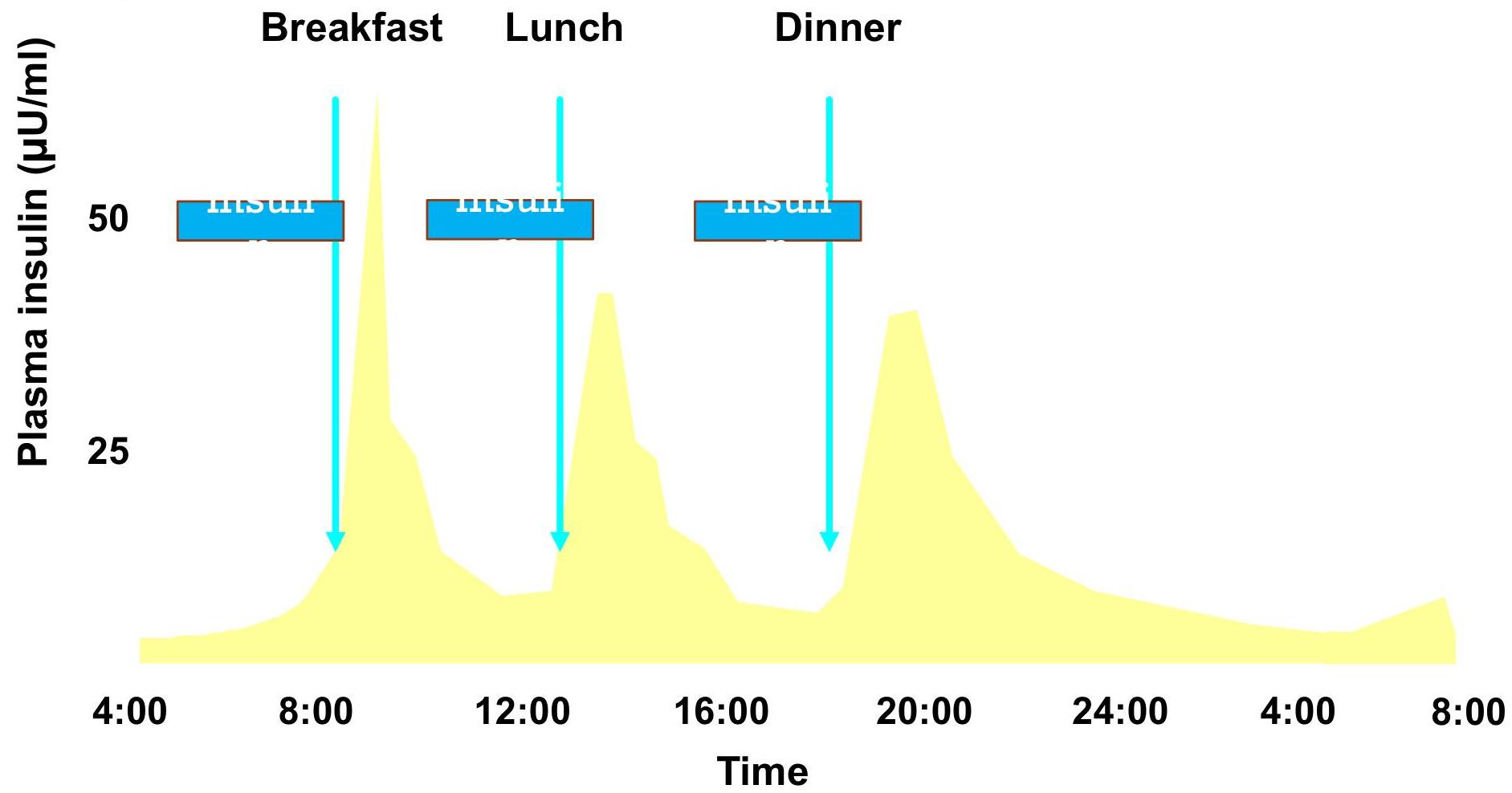
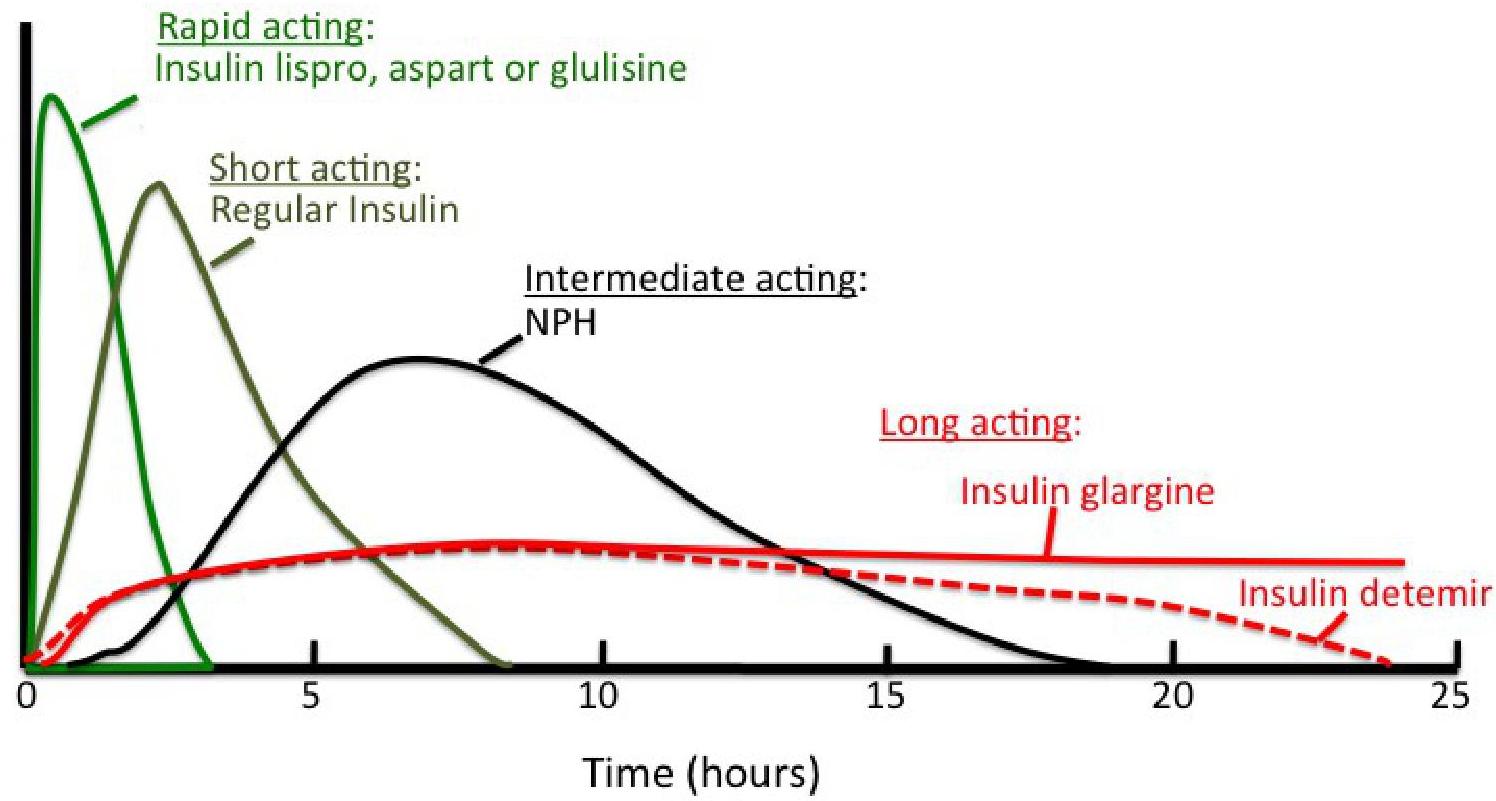
Physiological Serum Insulin Secretion Profile
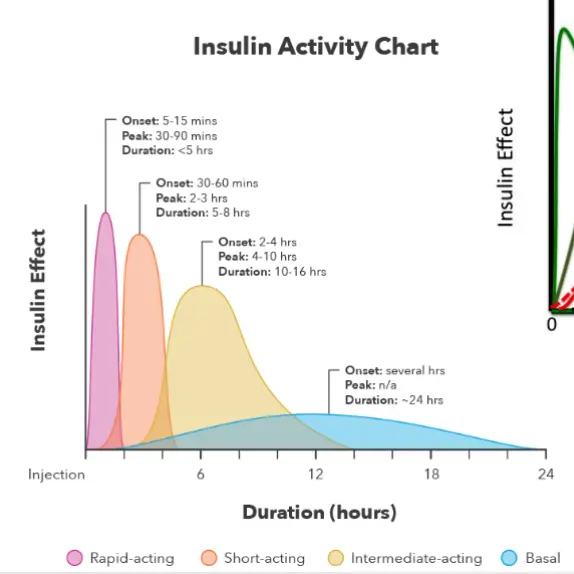
Types of Insulin Injections
Several Methods for Insulin Injections
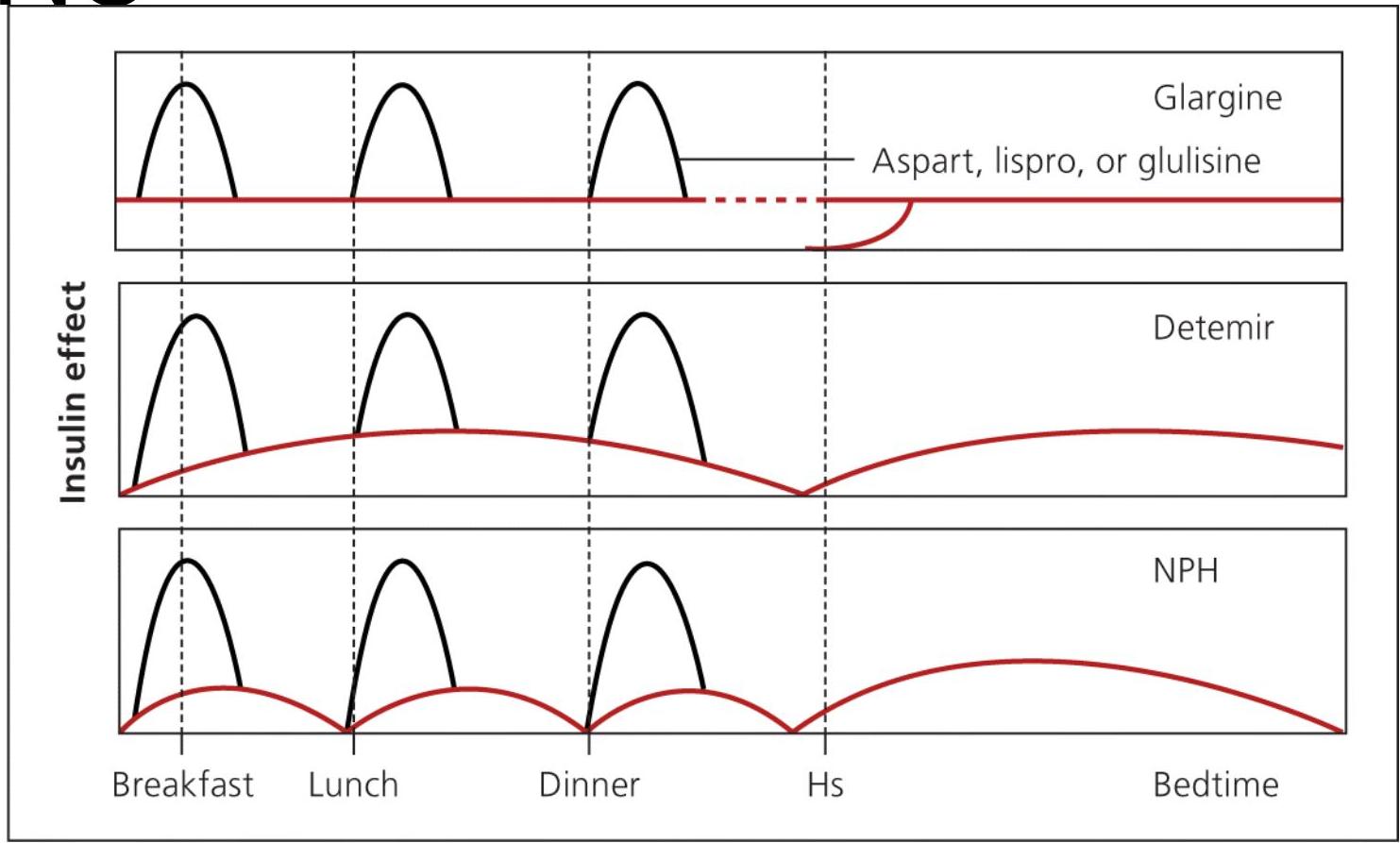
- Method A: once-daily glargine
- Method B: twice-daily detemir
- Method C: twice-daily NPH along with a short-acting analogue insulin before each meal
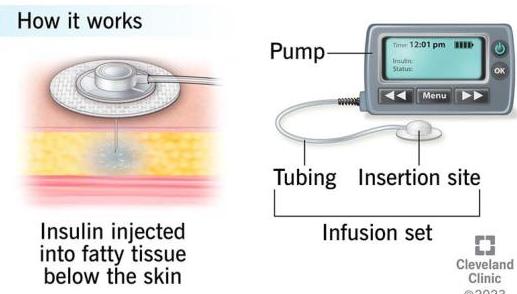
Insulin Pump
- Insulin pumps are programmed to automatically deliver certain amounts of fast-acting insulin that is stored in the pump’s reservoir. Insulin is delivered to the body through a tube attached to a small plastic needle, which is inserted under the skin
Insulin doses administered by an insulin pump are separated into:
- Basal rates: Basal insulin is delivered continuously throughout the day. It keeps blood glucose levels in range between meals and overnight.
- Bolus Doses to Cover Carbohydrate in Meals: When the patient eats a meal, an additional insulin dose called a bolus is required to cover the carbohydrates in each meal. The patient should insert the amount of carbohydrates in the meal by using the buttons on the insulin pump, as well as measure their blood sugar levels. The pump responds by providing options of insulin doses that are proportional to the amount of carbohydrates in the meal and the patient’s current blood sugar levels. It is then up to the patient to give the pumping order.
- Correction or Supplemental Doses: The patient inserts their current blood sugar levels, then chooses the appropriate dose by giving the pumping order.
Advantages of Using an Insulin Pump:
- It improves the patient’s quality of life and makes it easier for them to live with the disease
- Fewer injections and needles
- Tighter control over blood sugar levels (it reduces the risk of low blood sugar and improves average blood sugar levels)
- Easier and more efficient insulin delivery (with the press of a button)
Disadvantages of Using an Insulin Pump:
- Higher risk of skin infections and skin irritation
- It requires the patient to check their blood sugar level at least four times a day
- It can cause diabetic ketoacidosis due to pump malfunction if the tube gets blocked
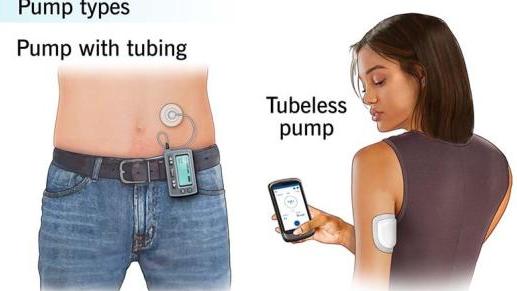 Insulin pumps
Insulin pumps
Blood Glucose Target in DM Patients
Blood glucose targets are:
- On waking: 4-7 mmol/l
- Before meals: 4-7 mmol/l Z
- After meals: 5-9 mmol/l
Injection Technique
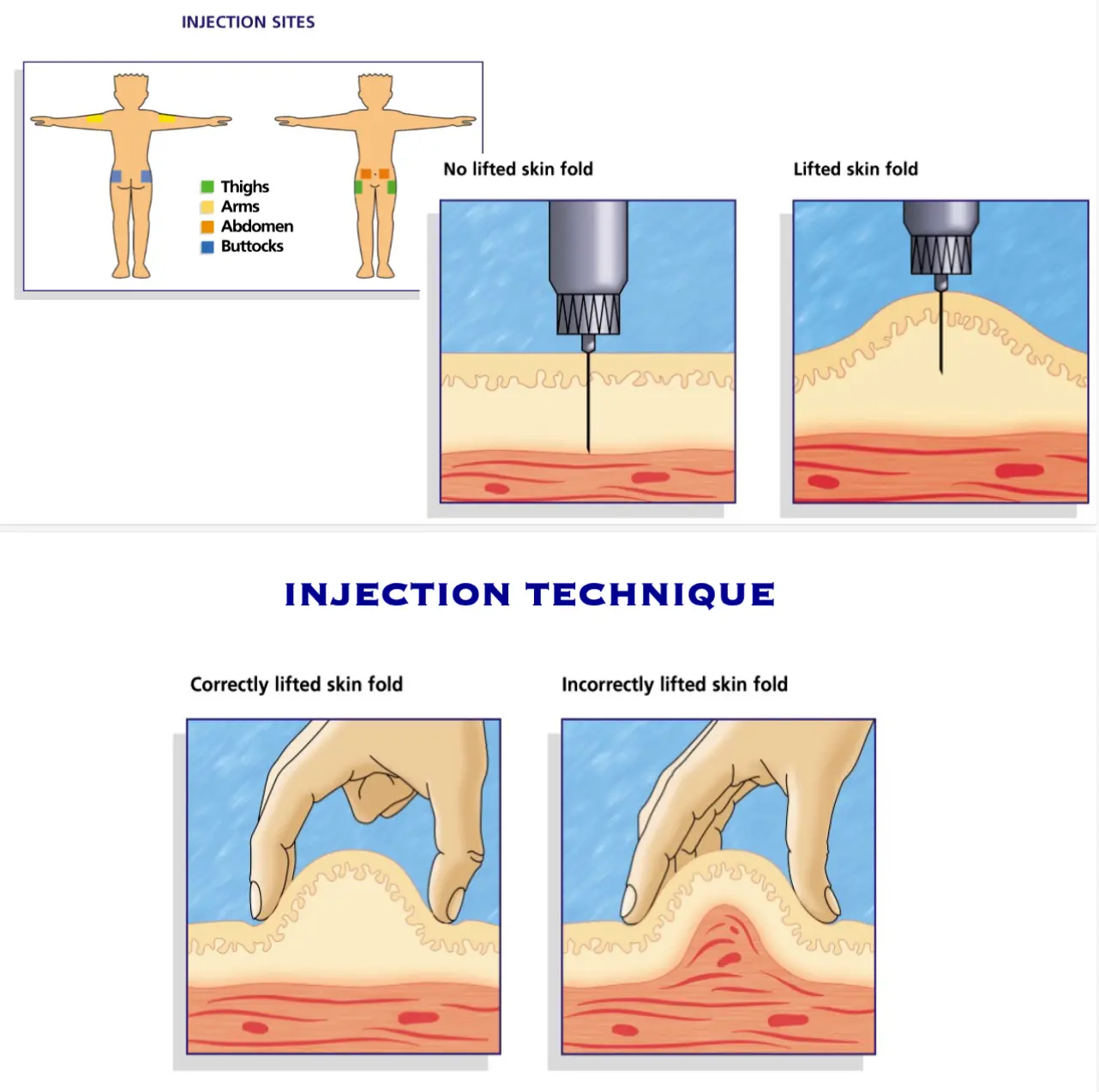
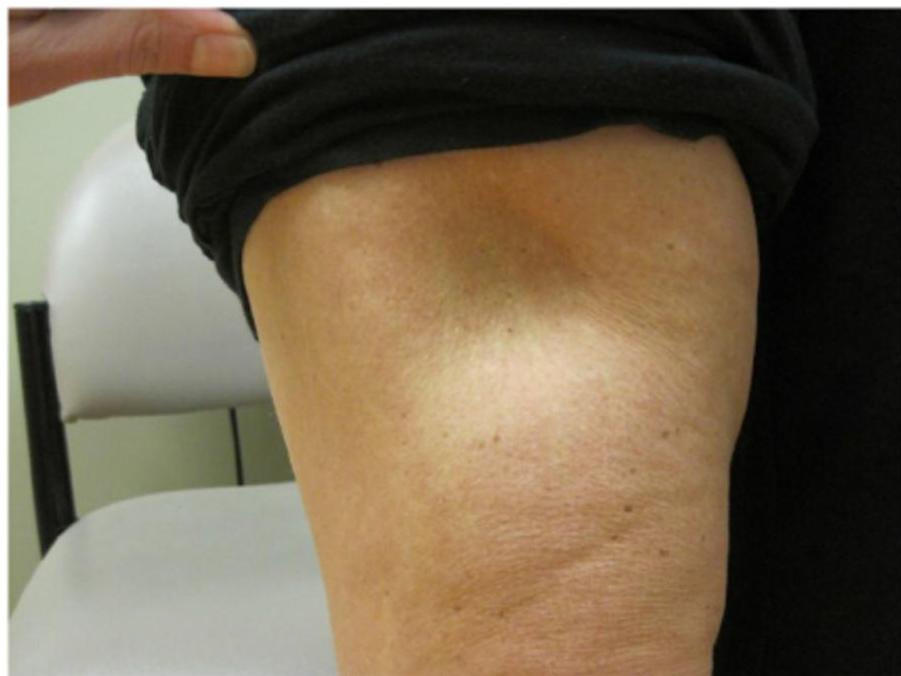
Complications to Insulin Injections
- Lipoatrophy (adverse immunological side effect of insulin)
- Lipohypertrophy (benign tumour-like swelling of fatty tissue at injection site secondary to lipogenic effect of insulin)
- Local Allergic reaction (erythema and pruritis)
Education and Counselling
Children with new-onset type 1 diabetes and their families require intensive diabetes education by a multidisciplinary pediatric diabetes healthcare team (endocrinologist, nutritionist, general pediatrician):
Insulin Action and Administration, Dosage Adjustment
- Fasting blood glucose reflects the action of the basal insulin and if patient has a pattern of high fasting blood glucose, then the basal insulin dose will need to be increased to bring the glucose level into target range
- The premeal blood glucose reflects the action of the insulin analogue injected in the preceding meal
- Start insulin as multiple daily insulin injections or as a continuous subcutaneous insulin infusion 0.5-0.78 units/kg/day
Patient and Family Education:
- Patients and their families should be taught to monitor glucose and blood ketones levels, assess carbohydrates content of food and use insulin:carbohydrate ratio to decide the premeal insulin dosage
- Patients and their families should learn how to manage both hypo and hyperglycemia, prevent development of DKA and manage days when other illnesses develop (sick day rules)
- If hypoglycemic, give oral sugar containing fluids. If unconscious, give glucagon 30 mcg/kg
- If hyperglycemic and ketones present in urine, give extra regular insulin 0.1 units/kg/dose every 4-6 hours Z
- All children and their families should be taught about the need for healthy eating and carbohydrate counting skills at diagnosis. Healthy, balanced diet consist of: z
- 50-60% of total calories from carbohydrate
- <30% from fat
- 10-20% from protein
- Families should be taught on how to use the information to adjust insulin dosages to achieve the glycemic target
- Exercise is essential for all and is to be encouraged and supported z
Sick Day Rules
Illness affects diabetes by two ways:
- Lack of appetite: Frequent monitoring and sugar-containing oral fluids to avoid hypoglycemia is required. Insulin may be decreased but NEVER STOPPED
- hyperglycemia and ketosis may be developed: Supplement with extra rapid or regular insulin 0.1 unit/kg/dose every 4-6 hours
Guidelines:
- Follow local guidelines given to patient and family by diabetes team
- Ensure drinking enough fluids to avoid dehydration
- Never stop or omit insulin—though dose may need adjusting
- Check blood glucose every 2 hours
- Check blood ketones regularly
- Administer correction doses of insulin to bring any high blood glucose in target
- If blood glucose and blood ketones are high and the child is vomiting, they need urgent admission to hospital as the child is in DKA
Autoimmune Disease
There is higher risk in developing other autoimmune diseases in DM I patients compared to general population:
| Autoimmune cond. inc. z | Indications for screening | Screening test | Frequency |
|---|---|---|---|
| Autoimmune thyroid disease - most common | All children with type 1 diabetes | Serum TSH level + thyroperoxidase antibodies | After diagnosis and every 2 years thereafter |
| Positive thyroid antibodies, thyroid symptoms or goiter | Serum TSH level + thyroperoxidase antibodies | Every 6–12 months | |
| Addison’s disease - uncommon | Unexplained recurrent hypoglycemia and decreasing insulin requirements | 8 AM serum cortisol + serum sodium and potassium | As clinically indicated |
| Celiac disease - 2nd | Recurrent gastrointestinal symptoms, poor linear growth, poor weight gain, fatigue, anemia, unexplained frequent hypoglycemia or poor metabolic control | Tissue transglutaminase + immunoglobulin A levels | As clinically indicated |
Others:
- Autoimmune liver disease
- Thyrotoxicosis
Complications
Risk of long-term complications is reduced by improved glycemic control:
- Diabetic nephropathy
- Diabetic retinopathy
- Diabetic neuropathy
- Ischemic heart disease
- Hypertension
- Peripheral and cerebrovascular disease
Outpatient Care:
- Visiting every 3 – 4 months
- HbA1C every 3 – 4 months
- Check clinically and biochemically for the associated condition eg. hypothyroidism once every 1 – 2 years
- Provide free access to service
- Continuous teaching
- Group activities
Screening for Complications: Z
| Complication | Indications & intervals for screening | Screening method |
|---|---|---|
| Nephropathy | • Yearly screening commencing at 12 years of age in those with duration of type 1 diabetes ≥ 5 years | • First morning (preferred) or random ACR • **Abnormal ACR **requires confirmation at least 1 month later with a first morning ACR, and if abnormal, followed by timed, overnight or 24-hour split urine collections for albumin excretion rate • Repeated sampling should be done every 3–4 months over a 12-month period to demonstrate persistence |
| Retinopathy | • Yearly screening commencing at 15 yrs of age with duration of DM ≥ 5 yrs • Screening interval can increase to 2 yrs if good glycemic control, duration of diabetes < 10 yrs, and no retinopathy at initial assessment | • 7-standard field, stereoscopic-colour fundus photography with interpretation by a trained reader (gold standard); or • Direct ophthalmoscopy or indirect slit-lamp fundoscopy through dilated pupil; or • Digital fundus photography |
| Neuropathy | • Postpubertal adolescents with poor metabolic control should be screened yearly after 5 years’ duration of DM - clinical | • Question and examine for symptoms of numbness, pain, cramps and paresthesia, as well as sensation, vibration sense, light touch & ankle reflexes |
| Dyslipidemia | • Delay screening post-diabetes diagnosis until metabolic control has stabilized • **Screen at ≥12 years **of age or <12 years of age with BMI > 95th percentile, family history of hyperlipidemia or premature CVD | • Fasting total cholesterol, high-density lipoprotein cholesterol, triglycerides, calculated low-density lipoprotein cholesterol |
| Hypertension | • Screen all children with type 1 diabetes at least twice a year | • Use appropriate cuff size |
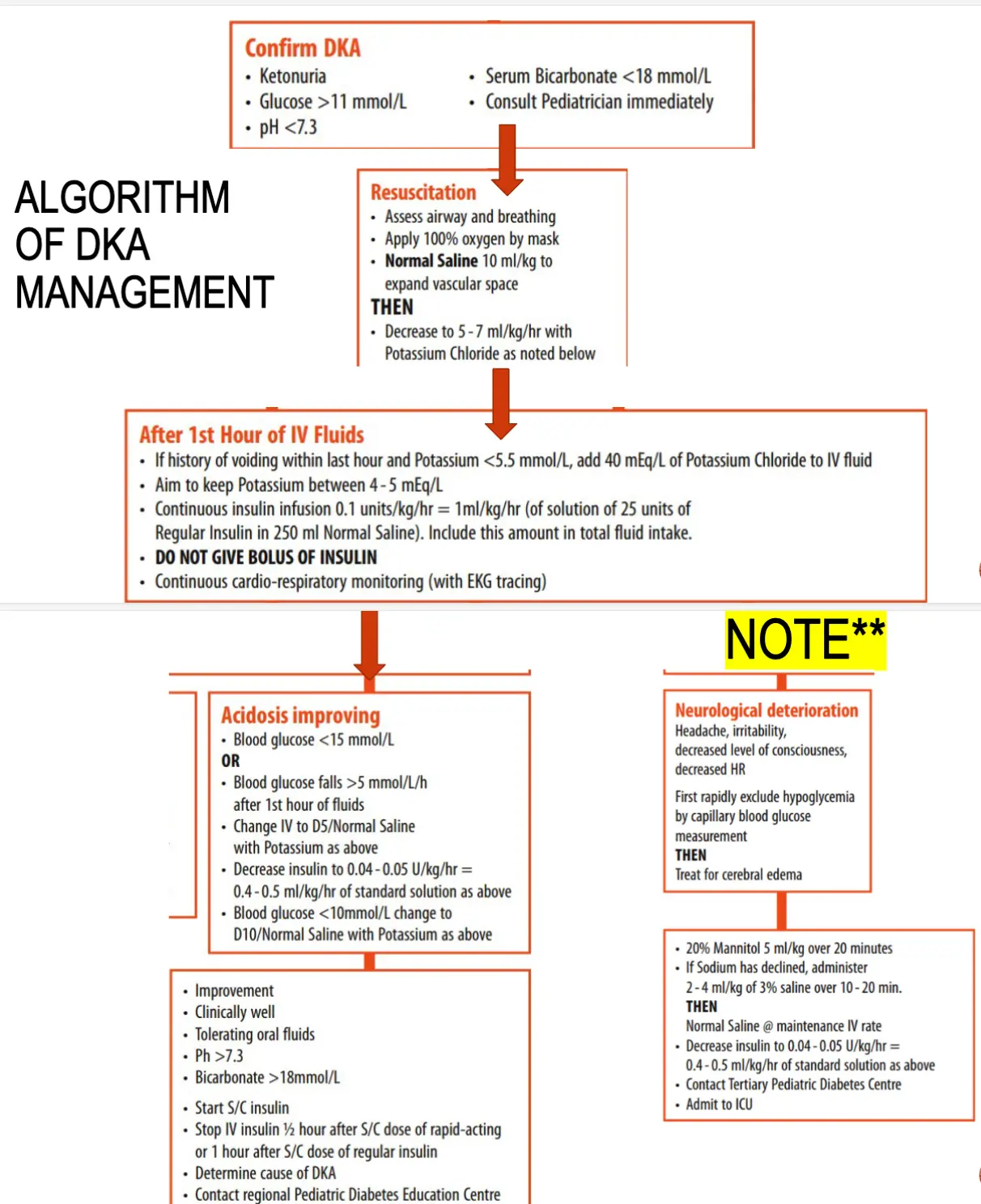
DKA (Diabetic Ketoacidosis) Management
Confirm DKA:
- Ketonuria
- Glucose >11 mmol/L
- pH <7.3
- Serum Bicarbonate <18 mmol/L
- Consult Pediatrician immediately
Algorithm of DKA Management
Resuscitation:
- Assess airway and breathing
- Apply 100% oxygen by mask
- Normal Saline 10 ml/kg to expand vascular space
THEN:
- Decrease to 5-7 ml/kg/hr with Potassium Chloride as noted below
After 1st Hour of IV Fluids:
- If history of voiding within last hour and Potassium <5.5 mmol/L, add 40 mEq/L of Potassium Chloride to IV fluid
- Aim to keep Potassium between 4-5 mEq/L
- Continuous insulin infusion 0.1 units/kg/hr = 1 ml/kg/hr Z (of solution of 25 units of Regular Insulin in 250 ml Normal Saline). Include this amount in total fluid intake.
- DO NOT GIVE BOLUS OF INSULIN
- Continuous cardio-respiratory monitoring (with EKG tracing)
NOTE: Acidosis improving
Acidosis Improving Criteria:
- Blood glucose <15 mmol/L
OR
- Blood glucose falls >5 mmol/L/h after 1st hour of fluids
- Change IV to D5/Normal Saline with Potassium as above
- Decrease insulin to 0.04 - 0.05 U/kg/hr = 0.4 - 0.5 ml/kg/hr of standard solution as above
- Blood glucose <10 mmol/L change to D10/Normal Saline with Potassium as above
Improvement Criteria:
- Clinically well
- Tolerating oral fluids
- pH >7.3
- Bicarbonate >18 mmol/L
- Start S/C insulin
- Stop IV insulin ½ hour after S/C dose of rapid-acting or 1 hour after S/C dose of regular insulin
- Determine cause of DKA
- Contact regional Pediatric Diabetes Education Centre
lastly admit to endocrinology team
Neurological Deterioration:
Symptoms: Headache, irritability, decreased level of consciousness, decreased HR
First rapidly exclude hypoglycemia by capillary blood glucose measurement
THEN:
Treat for cerebral edema:
- 20% Mannitol 5 ml/kg over 20 minutes
- If Sodium has declined, administer 2 - 4 ml/kg of 3% saline over 10 - 20 min
THEN:
- Normal Saline @ maintenance IV rate
- Decrease insulin to 0.04 - 0.05 U/kg/hr = 0.4 - 0.5 ml/kg/hr of standard solution as above
- Contact Tertiary Pediatric Diabetes Centre
- Admit to ICU
Hypoglycemia
Defined as: < 2.7 mmol/L (50 mg/dl)
Causes of Hypoglycemia:
- Behavioral in diabetic patient: Relative excess of insulin following missed meals, Exercise, Mismatch between insulin administered and food consumed
- Hyperinsulinemia
- Hypopituitarism
- Growth hormone deficiency
- Cortisol deficiency
- Ketotic hypoglycemia
Clinical Presentation of Hypoglycemia:
- Hunger
- Sweating
- Palpitations
- Lethargy and inattention
- Seizures
- Loss of consciousness
- Behavioral Problems
- Headache
- Drowsiness
- Irritation and Behaviour changes
- Blurred vision
- Difficulty concentrating
- Coma
Management of Hypoglycemia
- In mild to moderate hypoglycemia, where individual can swallow, immediate oral liquid containing glucose should be given: 10-15 g of glucose
- If unconscious, or reduced level of consciousness, IM glucagon should be administered
- Those who are at hospital and have IV access should be given a rapid bolus of 10% dextrose infusion (2 ml/kg) Z
How to Reduce Hypoglycemia:
- Regular glucose monitoring
- Education on management of exercise and sick days
- Good carbohydrate counting skills
Management Plan for Hypoglycemia
Hypoglycemia: Blood sugar < 3.3 mmol/l (60 mg/dl)
Collect blood sample for investigations (blood gas, insulin, BOHB, lactate, FFA)
Conscious & Asymptomatic:
- Send blood sample for glucose
- Offer feed or sugary drink for older children
- Recheck blood sugar by 15 min
Impaired Consciousness, Convulsion or Coma:
- Collect sample of blood for investigations
- IV glucose 10% dextrose normal saline:
- 5 ml/kg over 3-4 minutes followed immediately by D10 normal saline in maintenance IVF (6-9 ml/kg/minute)
- Repeat blood sugar after 15 minutes if there is No Response
- Repeat D10% dextrose bolus if still there is No response
- Increase rate and concentration of glucose infusion. If >12.5% of glucose infusion is needed to maintain normal blood sugar, insertion of central line is advisable. If still there is No response:
- Glucagon:
- <20 Kg: 0.5 mg SC/IM/IV; may repeat in 15 minutes if necessary
- >20 Kg: 1 mg SC/IM/IV; may repeat in 15 minutes if necessary
- Glucagon:
- Repeat blood sugar every 15 minutes
- Once blood sugar is controlled, oral feeding should be started
- Glucose infusion should be gradually discontinued
- Try to find the cause of hypoglycemia
- Consult pediatric endocrinologist