DISORDER OF ESOPHAGUS
GASTROESOPHGEAL REFLUX (GER)
DR Mansour ALQurashi
Learning Objectives
- Definition.
- Incidence.
- Pathogenesis.
- Clinical Presentation.
- Diagnosis.
- Treatment.
DEFINITIONS
Gastroesophageal reflux (GER) refers to the retrograde passage of gastric contents into the esophagus, with or without regurgitation and/or vomiting
Gastroesophageal reflux disease (GERD) is present when reflux episodes are associated with complications
Regurgitation versus vomiting – The term “regurgitate” describes reflux to the oropharynx, and “vomit” describes expulsion of the refluxate out of the mouth but not necessarily repetitively or with force
Rumination – describes a distinct phenomenon in which food is voluntarily regurgitated into the mouth, masticated, and then re-swallowed. This disorder should be considered as a possible cause of GER but it has a behavioral etiology
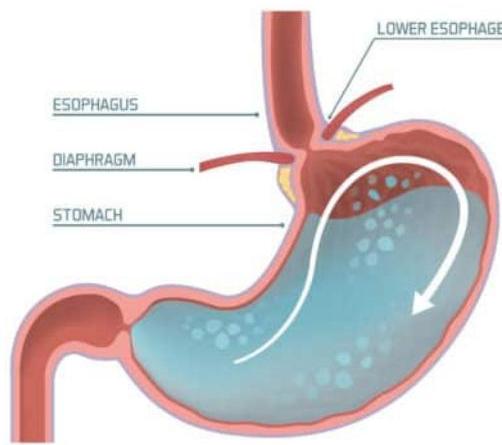
Pathophysiology
Gastroesophageal reflux (GER)
- It is a digestive disorder that affects lower esophagus sphincter (LES). The ring of muscle between esophagus and stomach.
GERD
-
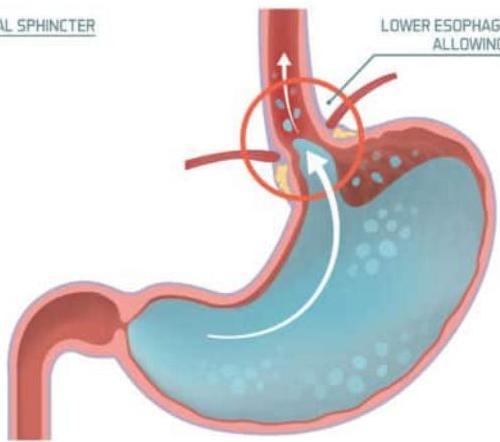
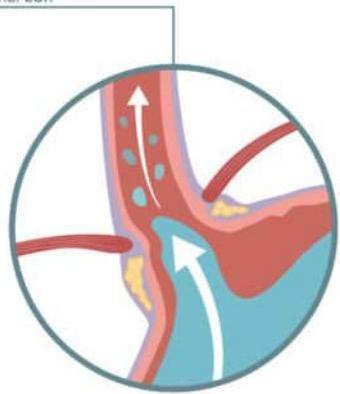
In pediatric gastroesophageal reflux disease (GERD), immaturity of lower esophageal sphincter function is manifested by frequent transient lower esophageal relaxations, which result in retrograde flow of gastric contents into the esophagus.
-
Return of the stomach contents back up into esophagus irritate the esophageal mucosa causing esophagitis.
ACID REFLUX Infographic
ACID REFLUX
MEDICINE AND HEALTHCARE INFOGRAPHIC
MEDICAL TREATMENT AND PREVENTION
GASTRIC DISEASE
HEALTHY STOMACH
GERD STOMACH
ACID REFLUX
Epidemiology
- GER is commonly seen in infancy (peak at age 1-4 months)
- Approximately 85% of infants vomit during the 1st week of life, and 60-70% manifest clinical GER at age 3-4 months
- Symptoms disappear without treatment in 60% of infants by age 6 months, when these infants begin to assume an upright position and eat solid foods
- Children with neurodevelopmental disabilities, (including cerebral palsy and Down syndrome), cystic fibrosis, obesity and hiatus hernia have an increased prevalence of GERD
- 2-8% of children 3-12 years have GERD
Table 2: Common Nonreflux Causes of Vomiting
| Infections | Neurologic |
|---|---|
| • Sepsis | • Hydrocephalus and shunt malfunctioning |
| • Meningitis | • Subdural hematoma |
| • Urinary tract infection | • Intracranial hemorrhage |
| • Otitis media | • Tumors |
| Obstruction | • Migraine |
| • Pyloric stenosis | Allergic |
| • Malrotation | • Dietary protein intolerance |
| • Intussusception | Respiratory |
| Gastrointestinal | • Posttussive emesis |
| • Eosinophilic esophagitis | • Pneumonia |
| • Peptic ulcer disease | Renal |
| • Achalasia | • Obstructive uropathy |
| • Gastroparesis | • Renal insufficiency |
| • Gastroenteritis | Cardiac |
| • Gall bladder disease | • Congestive heart failure and disease |
| • Pancreatitis | Recreational drugs and alcohol consumption |
| • Celiac disease | Pregnancy |
| • Pill esophagitis | Other |
| • Crohn disease | • Overfeeding |
| Metabolic/Endocrine | • Self-induced emesis |
| • Galactosemia | |
| • Fructose intolerance | |
| • Urea cycle defects | |
| • Diabetic ketoacidosis | |
| Toxic | |
| • Lead poisoning |
Clinical Presentation of GER
Vomiting:
- Recurrent
- Not forceful.
- Take large amount of milk.
- Strong sucking.
Examination in baby with GER
General appearance of the infant:
- Looks well, active
- Hydration status is normal
- Growth parameters: appropriate for age.
- Respiratory system: no signs of RD
- No evidence of esophagitis (fussiness, opisthotonic posturing)
Clinical manifestations of GERD in infant
- Aspiration: persistent cough / wheezing / chocking and recurrent pneumonias
- Failure to thrive: (Refusal to eat or frequent crying associating with feeding due to dysphagia)
- Esophagitis: Abd. Pain /fussy or forceful vomiting
- Apparent life threatening event (ALTE): apnea, pallor, cyanosis, plethora, floppiness, rigidity, choking and gagging
Complications
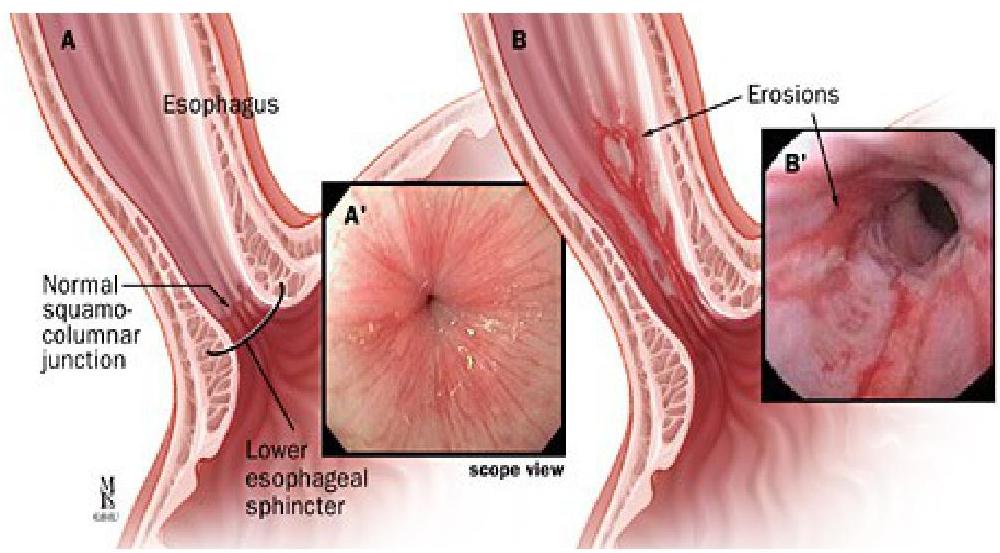
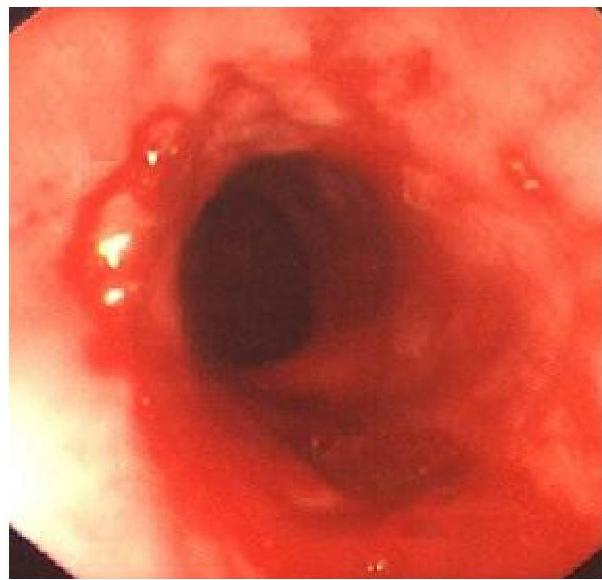
- Esophagitis.
- Hematemesis.
- 5% of untreated develop stricture.
- Laryngospasm, Apnea, Bradycardia.
- Barrett’s esophagus (metaplastic change).
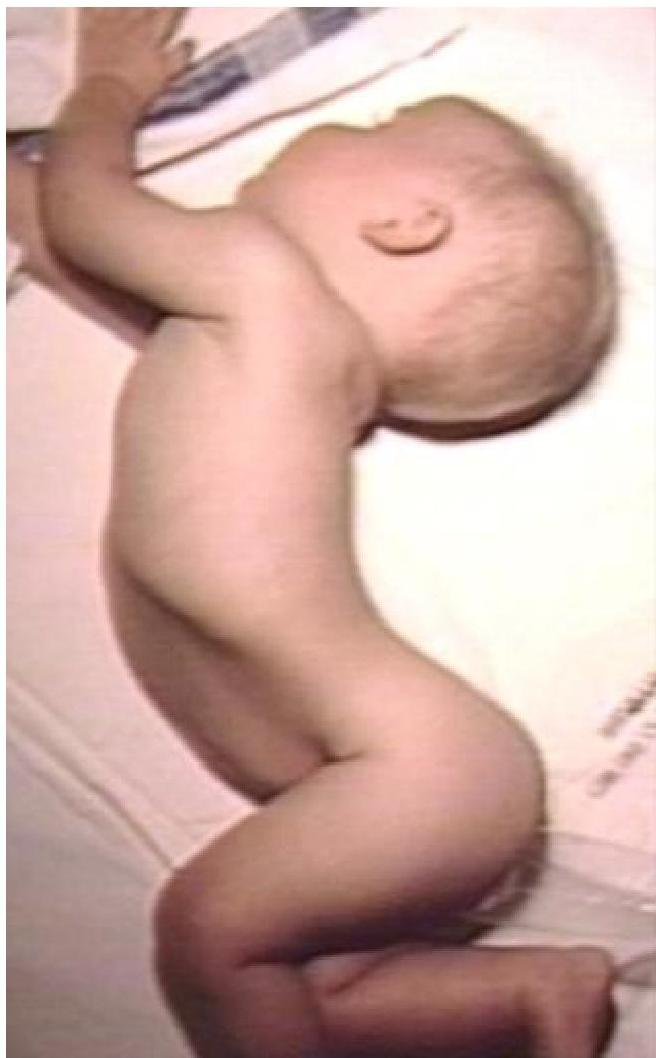
Sandifer Syndrome
Sandifer Syndrome: opisthontons, abnormal head position
Clinical manifestations of GERD in children
- Recurrent regurgitation that continues after two years of age
- Refusal of food, especially solids
- Frequent complaints of heartburn
- Dysphagia (difficulty swallowing)
- Severe or progressive asthma that is not responsive to standard therapy for asthma
- Recurrent pneumonia, particularly in children with neurologic dysfunction
- Chronic hoarseness or stridor
Diagnosis
History and physical examination
General investigations:
- CBC: Hb.
- S. Iron level.
- Stool Occult blood.
- Chest X-ray
Investigations
PH Probe Study
- Measures the acidity inside the esophagus over 24 H.

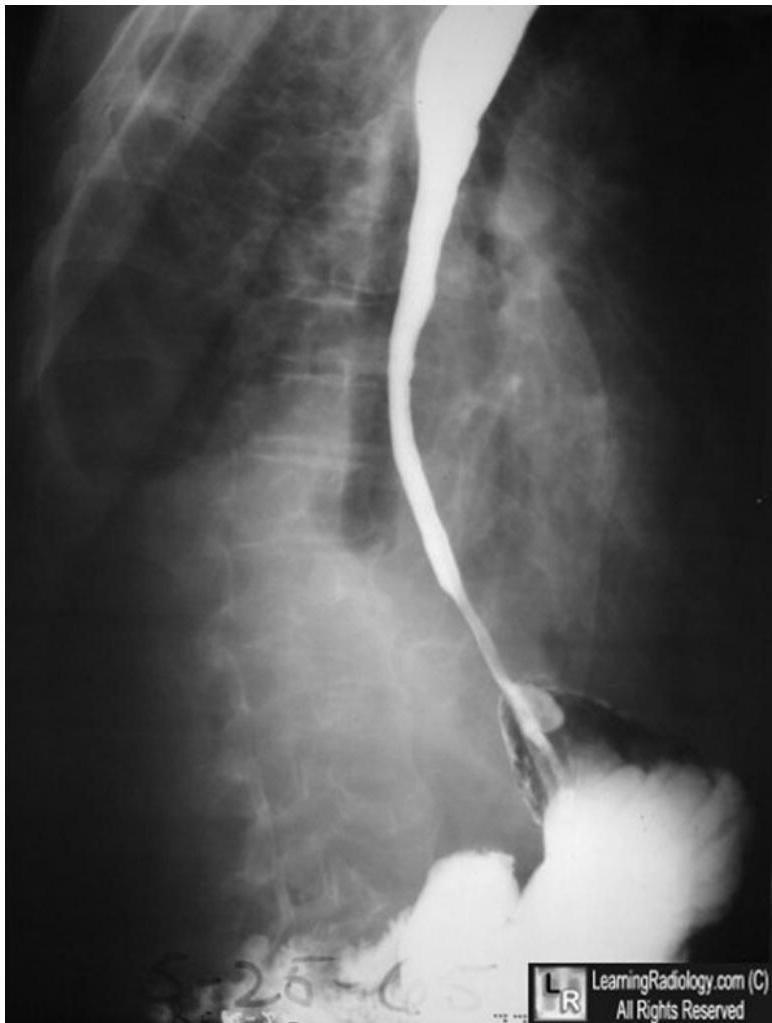
Barium swallow and follow through
- To detect any strictures, ulceration, to rule out intestinal obstruction, or to assess esophageal peristaltic wave.
Other Diagnostic Procedures
- Endoscopy (with biopsy): To look for erosions or ulcer of esophagus
- Esophageal manometry: Measures the pressure produced by the esophageal-muscles and wave propagation
- Gastric emptying study: Delayed gastric emptying can contribute to reflux into the-esophagus
- Milk scan: Looking for evidence of aspiration
Treatment
Non-pharmacological Management
- Feeding changes (frequent, small amount)
- Thickening milk by rice cereal or AR milk.
- Semi setting position.
- Brup after feeding.
- Avoid overfeeding.
Pharmacological Management
- Drugs to reduce stomach acidity.
- In children: Limit fluid intake at bedtime. Advice weight reduction for obese children.
Surgical Management
- Surgery if not responding to medication (Nissan Fundoplication).
Prognosis
- Most cases of GER in infants and very young children are benign, and 80% resolve by age 18 months
- Symptoms that persist after age 18 months suggest a higher likelihood of chronic GER
- In refractory cases of GER or when complications are identified (eg, stricture, aspiration, airway disease, Barrett esophagus), surgical treatment (fundoplication) is typically necessary
- The prognosis with surgery is considered excellent
Eosinophilic Esophagitis
Definition and Overview
- Chronic, immune/antigen-mediated, esophageal disease characterized clinically by symptoms related to esophageal dysfunction and histologically by eosinophil-predominant inflammation
- Incidence: 2 per 10,000 population
- More common in males
Clinical Manifestations by Age Group
In children:
- Feeding difficulties
- Gastroesophageal reflux symptoms
- Abdominal pain
In adults and teenagers:
- Dysphagia
- Food impactions
- Esophageal dysmotility may also be observed, suggesting possible eosinophil involvement of the muscular layers of the esophagus
- Endoscopic ultrasonography has shown expansion of the esophageal wall and all individual tissue layers
Association with allergic conditions:
- Strong association of EoE with allergic conditions such as food allergies, environmental allergies, asthma, and atopic dermatitis
Clinical manifestations in children (with median ages)
- Feeding dysfunction (median age 2.0 years)
- Vomiting (median age 8.1 years)
- Abdominal pain (median age 12.0 years)
- Dysphagia (median age 13.4 years)
- Food impaction (median age 16.8 years)
Diagnosis
The diagnosis is based upon:
- Symptoms
- Endoscopic appearance
- Histological findings
Diagnostic criteria — The diagnosis of EoE requires all of the following:
- Symptoms related to esophageal dysfunction
- Eosinophil-predominant inflammation on esophageal biopsy
- Exclusion of other causes that may be responsible for or contributing to symptoms and esophageal eosinophilia
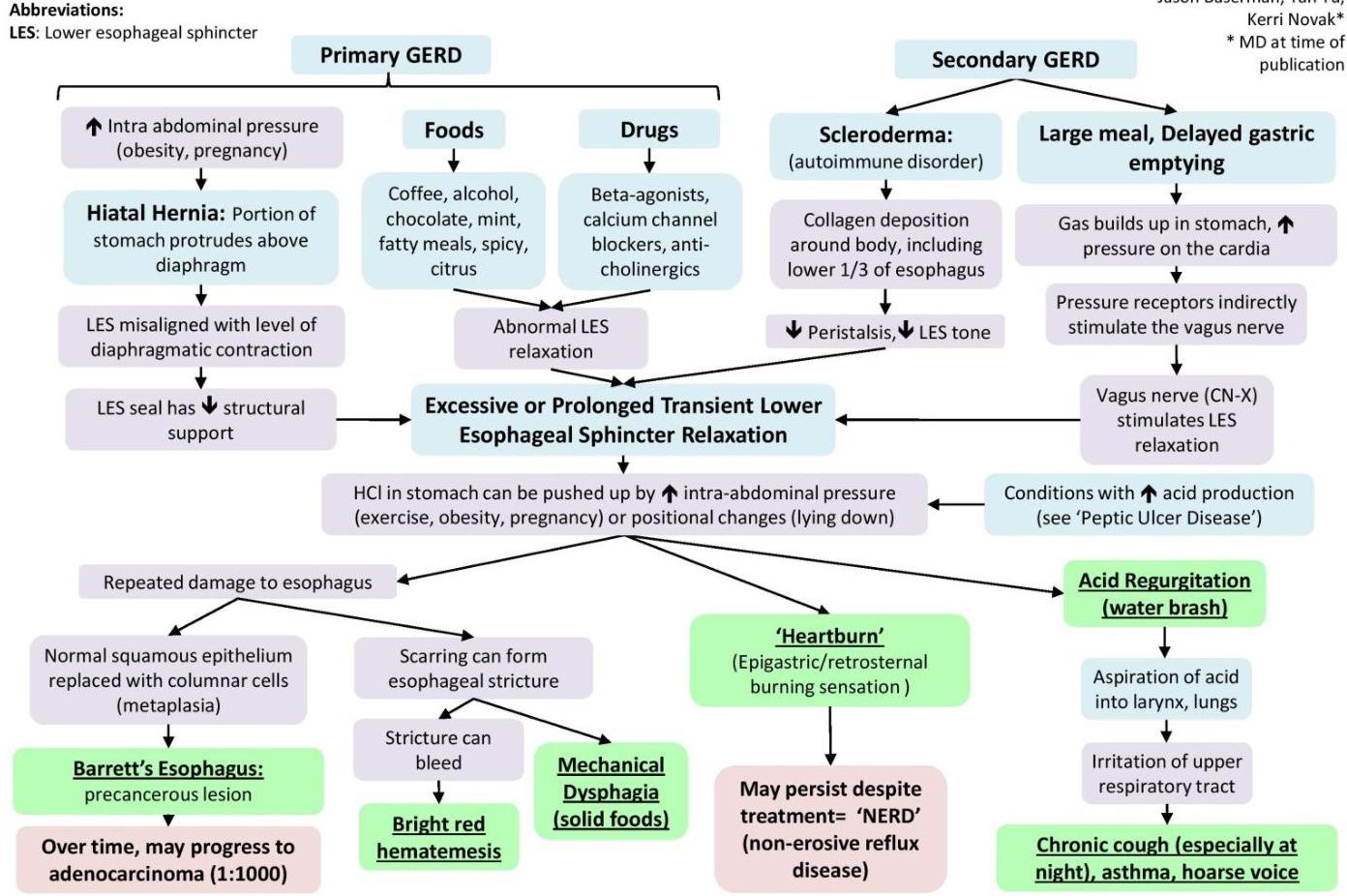
Pathogenesis Diagram
Gastroesophageal Reflux Disease (GERD): Pathogenesis & Clinical Findings
Author: Matthew Harding Reviewers: Dean Percy, Jason Baserman, Yan Yu, Kerri Novak* *MD at time of publication
Abbreviations:
LES: Lower esophageal sphincter