ACUTE MYOCARDITIS
Definition: Inflammation of the heart muscle resulting in myocardial dysfunction and heart failure.
- Infectious Etiologies: Coxsackie group B, adenovirus, parvovirus B19, EBV, CMV, HHV-6. z
- Other Etiologies: Autoimmune disorders, drug hypersensitivity (rare).
Clinical Manifestations
- History: Respiratory or GI illness within previous 2 weeks. Fever, myalgia, malaise several days prior to heart dysfunction.
- Presentation: Signs of HF (dyspnea, exercise intolerance, syncope, tachypnea, tachycardia, hepatomegaly).
- Prominent Features: Anorexia, abdominal pain, vomiting.
- Fulminant Myocarditis: Critically ill, hypotension, poor pulses, decreased perfusion, acidosis, altered mental status, edema, hepatomegaly, potential cardiovascular collapse. Malignant arrhythmias common.
Physical Examination
- Systemic/Pulmonary Congestion: Tachypnea, retractions, rales (elevated LA pressure).
- Ventricular Dysfunction: S3 and S4 gallops (biventricular).
- Murmurs: Functional MR, TR if severe dilation.
Investigations
Laboratory Tests
- Inflammatory Markers: ESR and CRP frequently elevated.
- CBC: Evidence of infection.
- Blood Gases: Metabolic acidosis (in fulminant cases/inadequate perfusion).
- Cardiac Biomarkers:
- Troponin T / CK-MB: Elevated (helpful to distinguish from chronic dilated CM).
- BNP: Elevated (distinguishes HF from primary pulmonary pathology).
- Viral Titers/PCR: A 4-fold increase in a specific titer from the acute to convalescent phase is strong evidence of infection.
Imaging & ECG
- Chest Radiograph:
- Abnormal in ~50%.
- Cardiomegaly, pulmonary vascular congestion, pleural effusions.
- Echocardiogram:
- Ventricular dysfunction, changes in LV geometry.
- Wall motion abnormalities, mitral regurgitation.
- ECG:
- Sinus tachycardia, PVCs, PACs, SVTs, VT. Rarely complete heart block. Z
- ST-segment changes, inverted T waves, abnormal axis, hypertrophy, decreased voltages.
Chest radiograph of an adolescent with viral myocarditis
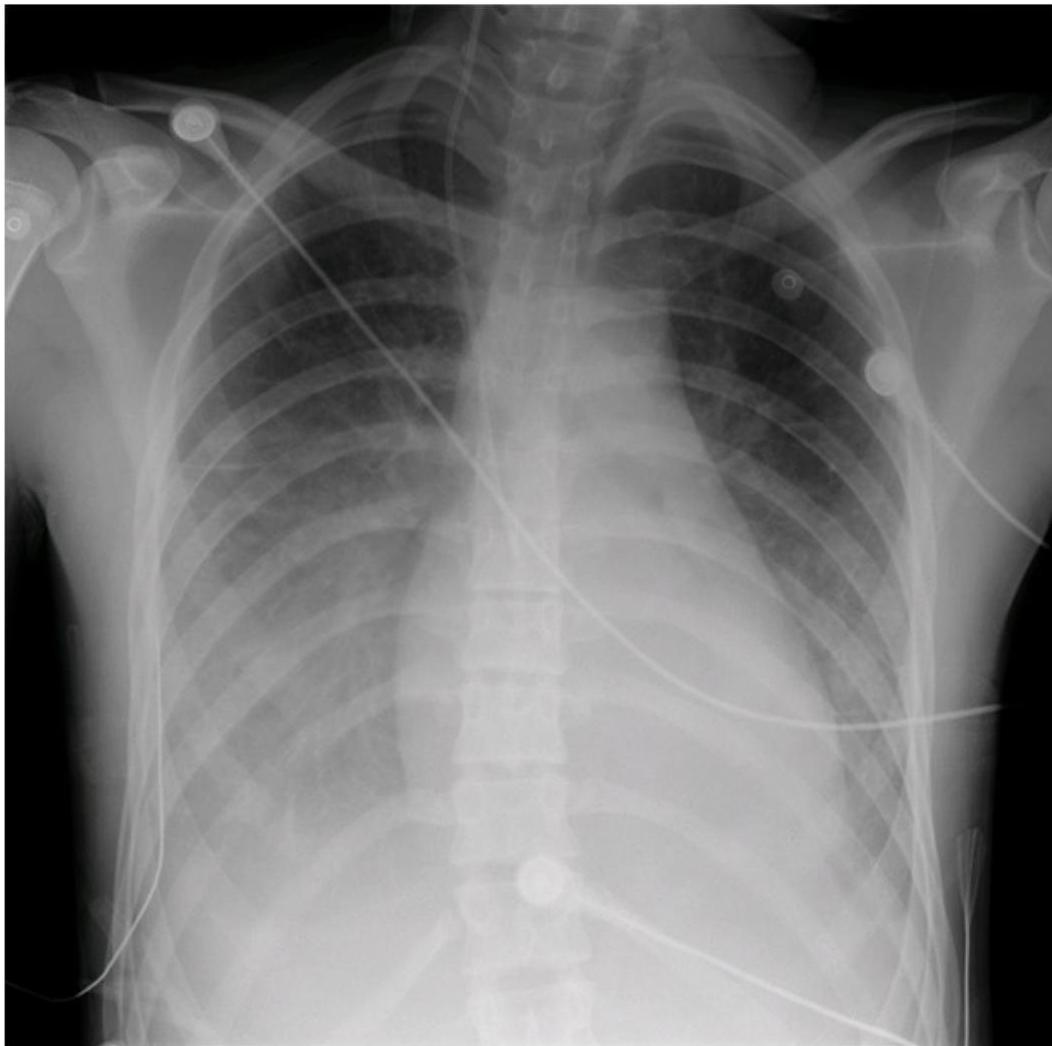 Mild cardiomegaly, bilateral pleural effusions, prominence of central pulmonary vessels, interstitial haziness, suggestive of pulmonary edema. Child was a previously healthy 15-year-old boy who presented with severe chest pain in the setting of a viral prodrome.
Mild cardiomegaly, bilateral pleural effusions, prominence of central pulmonary vessels, interstitial haziness, suggestive of pulmonary edema. Child was a previously healthy 15-year-old boy who presented with severe chest pain in the setting of a viral prodrome.
Chest radiograph of a child with fulminant viral myocarditis
 Bilateral lung opacities, sizable bilateral pleural effusions, borderline cardiomegaly. Child was a previously healthy 9-year-old girl who presented with progressive orthopnea, cough, and respiratory distress following 2 weeks of a viral prodrome. Child presented in severe distress and suffered cardiopulmonary arrest shortly after arrival to the emergency department. Management included inotropic support, diuretic therapy, placement of bilateral chest tubes, and intravenous immune globulin. She subsequently made a full recovery.
Bilateral lung opacities, sizable bilateral pleural effusions, borderline cardiomegaly. Child was a previously healthy 9-year-old girl who presented with progressive orthopnea, cough, and respiratory distress following 2 weeks of a viral prodrome. Child presented in severe distress and suffered cardiopulmonary arrest shortly after arrival to the emergency department. Management included inotropic support, diuretic therapy, placement of bilateral chest tubes, and intravenous immune globulin. She subsequently made a full recovery.
Electrocardiogram in a 17-year-old female with myocarditis
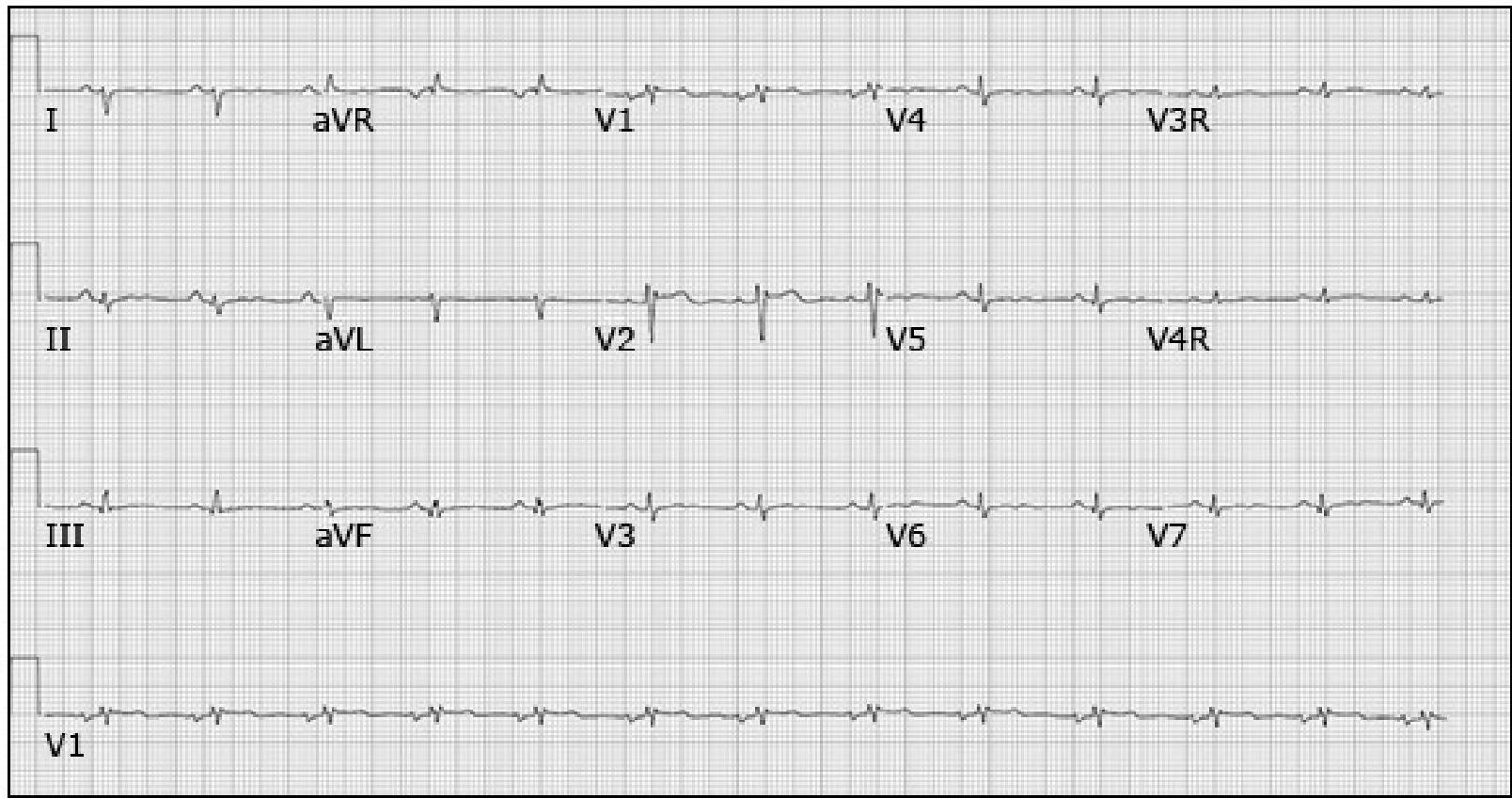 Demonstrating decreased QRS voltage with ST segment and T wave abnormalities.
Demonstrating decreased QRS voltage with ST segment and T wave abnormalities.
Diagnosis
Suspect in patients with new onset:
- Signs/symptoms of cardiac dysfunction.
- Rise in biomarkers (Troponin).
- ECG changes (injury/arrhythmia).
- Echo evidence of dysfunction without structural defect.
- Cardiac MRI: Increasingly used.
- Endomyocardial Biopsy.
Differential Diagnosis
- Acute heart failure.
- Structural heart disease.
- Cardiomyopathy.
- Respiratory distress (Pneumonia, Bronchiolitis).
Management
- Asymptomatic/Mild: Diuretics, Afterload reducing agents (ACE inhibitors).
- Severely Affected (PICU):
- IV agents (Dopamine, Dobutamine, Milrinone).
- Diuretics, ACE inhibitors.
- Antiarrhythmics if indicated.
- Intravenous Immunoglobulin (IVIG):
- High dose (2 g/kg over 24h) advised.
- Associated with greater ventricular fractional shortening and reduced morbidity/mortality.
- Mechanical Support: ECMO or VAD for severe compromise.
- Mortality: ~7%.
Natural Course
- Dilated Cardiomyopathy Phase:
- Occurs in a subset (prolonged autoimmune response / incomplete viral clearance).
- Management: Continue HF therapy; Cardiac Transplantation if needed.