HEART FAILURE
HEART FAILURE DEFINITION
It is a clinical syndrome that reflects the inability of the heart to meet the metabolic requirement of the body.
This definition includes both types of HF in children:
- High cardiac output failure (Over-circulation failure).
- Pump failure.
HF FUNCTIONAL CLASSIFICATION
Excessive Work Load
- Volume Overload: VSD, A.R.
- Pressure Overload: A.S, P.S, M.S.
Disorders of Myocardium
- Systolic dysfunction (reduced ventricular contractility): impaired ejection of blood from ventricle.
- Diastolic dysfunction (impaired ventricular filling and noncompliance): resulting in high ventricular filling pressures.
Disorders of Rhythm
- Tachyarrhythmia / Bradyarrhythmia.
CAUSES OF HF IN INFANTS AND CHILDREN
Ventricular Dysfunction
Systolic Dysfunction / Diastolic Dysfunction
- Structurally normal heart:
- Cardiomyopathy / Myocarditis.
- Myocardial ischemia / MI (e.g., ALCAPA, KD, familial hypercholesterolemia).
- Arrhythmogenic (e.g., SVT, VT, CHB).
- Drug/toxin exposure (e.g., Adriamycin for ALL).
- Noncardiac causes: Sepsis, Renal failure, Respiratory disorders (e.g., bronchopulmonary dysplasia, cystic fibrosis, interstitial lung disease, SLE).
- Complex congenital heart disease: e.g., children born with complex CHD who undergo surgical repair or palliation in early childhood.
Preserved Ventricular Contractility Z
Volume Overload
- Left-to-right shunting: VSD, ASD, PDA.
- Valvular insufficiency: AR, MR, PR.
- Noncardiac causes: AV Malformation, fluid overload (KF).
Pressure Overload
- Left-sided: AS, COA, Systemic hypertension.
- Right-sided: PS, Pulmonary hypertension.
Note: Depending on severity and chronicity, pressure overload may result in either systolic or diastolic dysfunction.
Common Causes Detailed (By Etiology)
CHD (Congenital Heart Disease)
- Pressure overload:
- Aortic stenosis
- Coarctation of aorta
- Interrupted aortic arch
- Pulmonary stenosis
- Pulmonary vein stenosis
- Volume overload:
- Left-to-right shunts
- Aortic regurgitation
- Mitral regurgitation
- Ebstein anomaly with severe tricuspid regurgitation
- Both volume and pressure overload:
- Hypoplastic left heart
- CHD with single ventricle physiology
- Ischemia:
- Coronary anomaly
- Perioperative injury/ischemia
Cardiomyopathy
- Primary Cardiomyopathies:
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Restrictive cardiomyopathy
- Arrhythmogenic RV dysplasia
- LV noncompaction cardiomyopathy
- Secondary Cardiomyopathies:
- Inflammatory: Myocarditis
- Infections: HIV, rheumatic fever, Chagas disease
- Drug-or-toxin related: Anthracycline, iron overload
- Arrhythmias: Tachyarrhythmia, congenital heart block
- Ion channel disorder
- Neuromuscular disorders
- Nutritional deficiency: Carnitine deficiency
- Sepsis
- Stress
- Endocrine: Thyrotoxicosis
- Severe anemia
- Systemic arteriovenous fistula
- Genetic syndromes (Noonan) even without CHD
- Infant of diabetic mother
- Storage disorders: Pompe disease
- Mitochondrial myopathies
- Chronic renal failure
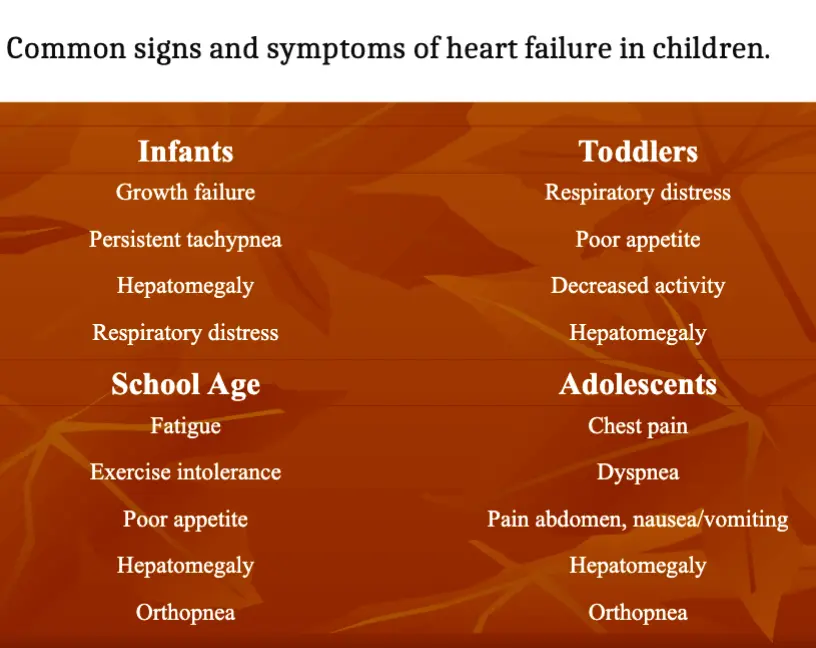
SYMPTOMS OF HF
Symptoms in Infants
- Tachypnea.
- Diaphoresis during feeds.
- Easy fatigability.
- Irritability.
- Decreased volume of feeds, and poor weight gain.
- Undernutrition may result in delayed motor milestones.
- Growth failure.
- Hepatomegaly.
- Respiratory distress.
Symptoms in Toddlers / Young Children
- GIT symptoms (abdominal pain, nausea, vomiting, and poor appetite).
- Poor weight gain.
- Easy fatigability.
- Recurrent or chronic cough with wheezing.
- Respiratory distress.
- Decreased activity.
- Hepatomegaly.
Note: These symptoms are often mistaken for gastroenteritis, reflux, asthma, and behavioral issues.
Symptoms in School Age / Older Children / Adolescents
- Exercise intolerance.
- Fatigue.
- Anorexia, poor appetite, abdominal pain, nausea/vomiting.
- Wheezing, dyspnea.
- Edema.
- Palpitations, chest pain.
- Syncope.
- Orthopnea.
- Hepatomegaly.
Note: A high index of suspicion is needed to distinguish HF from other far more common pediatric illnesses (e.g., pneumonia, sinusitis, otitis media, viral illnesses, gastroenteritis, and asthma [50%]).
SIGNS OF HEART FAILURE
Signs of Impaired Myocardial Function
- Cardiac enlargement.
- Tachycardia.
- Gallop rhythm.
- Cold extremities, pallor, weak pulses.
- Low BP, skin mottling, capillary refill.
- Sweating.
- Growth failure.
- Pulses paradoxis-alternans.
Signs of Pulmonary Congestion
- Tachypnea (most common).
- Hyperpnea.
- Wheezing / Rales (Older children).
- Cyanosis.
- Dyspnea and signs of respiratory distress.
- Cough.
Signs of Systemic Venous Congestion
- Hepatomegaly (the most common finding).
- Neck vein distension.
- Facial edema.
- Peripheral edema.
- Ascites and splenomegaly (may be present in severe right HF).
- Jugular venous distension (not generally observed in infants and young children).
Other Findings for Underlying Etiology
- High BP limited to arms and weak pulses in legs are suggestive of COA.
- A systolic murmur may be seen in HOCM, AS, VSD, MR.
- Precordial examination may reveal a “thrill” in patients with VSD.
- A longstanding cardiomyopathy may have a “heave” with a laterally displaced point of maximal impulse.
ADAPTIVE MECHANISMS
- Ventricular Dilatation/Hypertrophy.
- Adrenergic Mechanisms.
- Erythrocyte Oxygen Transport.
- Regional Circulations (Pulmonary, Renal, GIT, Skin, Liver).
- Natriuretic Peptide (ANP/BNP): Vasodilation, natriuresis, and diuresis.
- Vasopressin Hormone.
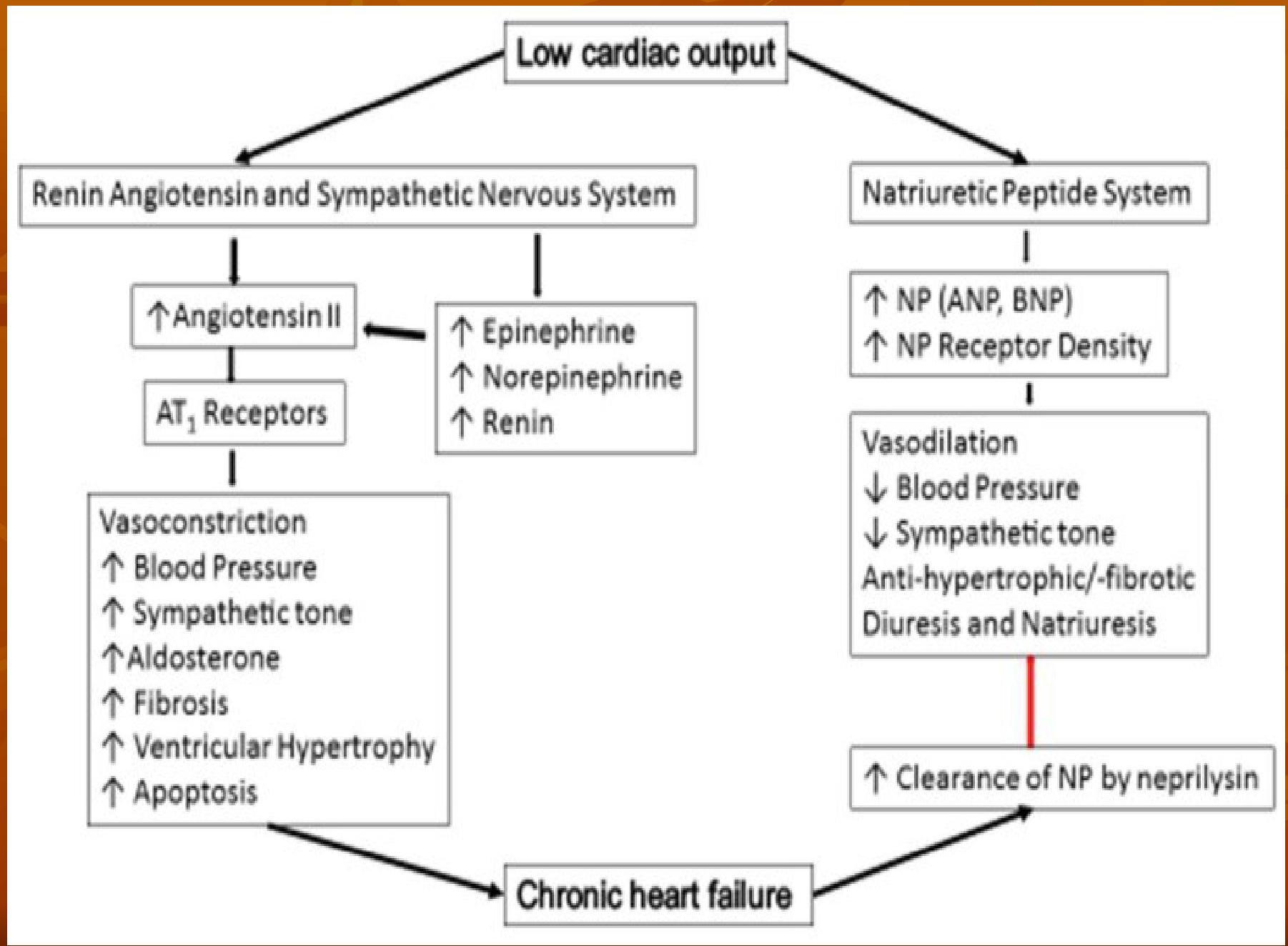 Pathophysiology of chronic heart failure
Pathophysiology of chronic heart failure
CLASSIFICATION OF SEVERITY
Modified Ross Classification (Children < 6 years)
- Class I: Asymptomatic.
- Class II: Mild tachypnea or diaphoresis with feeding in infants; dyspnea on exertion in older children.
- Class III: Marked tachypnea or diaphoresis with feeding in infants. Prolonged feeding times with growth failure; Marked dyspnea on exertion in older children.
- Class IV: Symptoms such as tachypnea, retractions, grunting, or diaphoresis at rest.
NYHA Classification (Children > 6 years)
- Class I: Asymptomatic.
- Class II: Slight or moderate limitations of physical activity.
- Class III: Marked limitation of physical activity.
- Class IV: Symptoms at rest.
INVESTIGATIONS
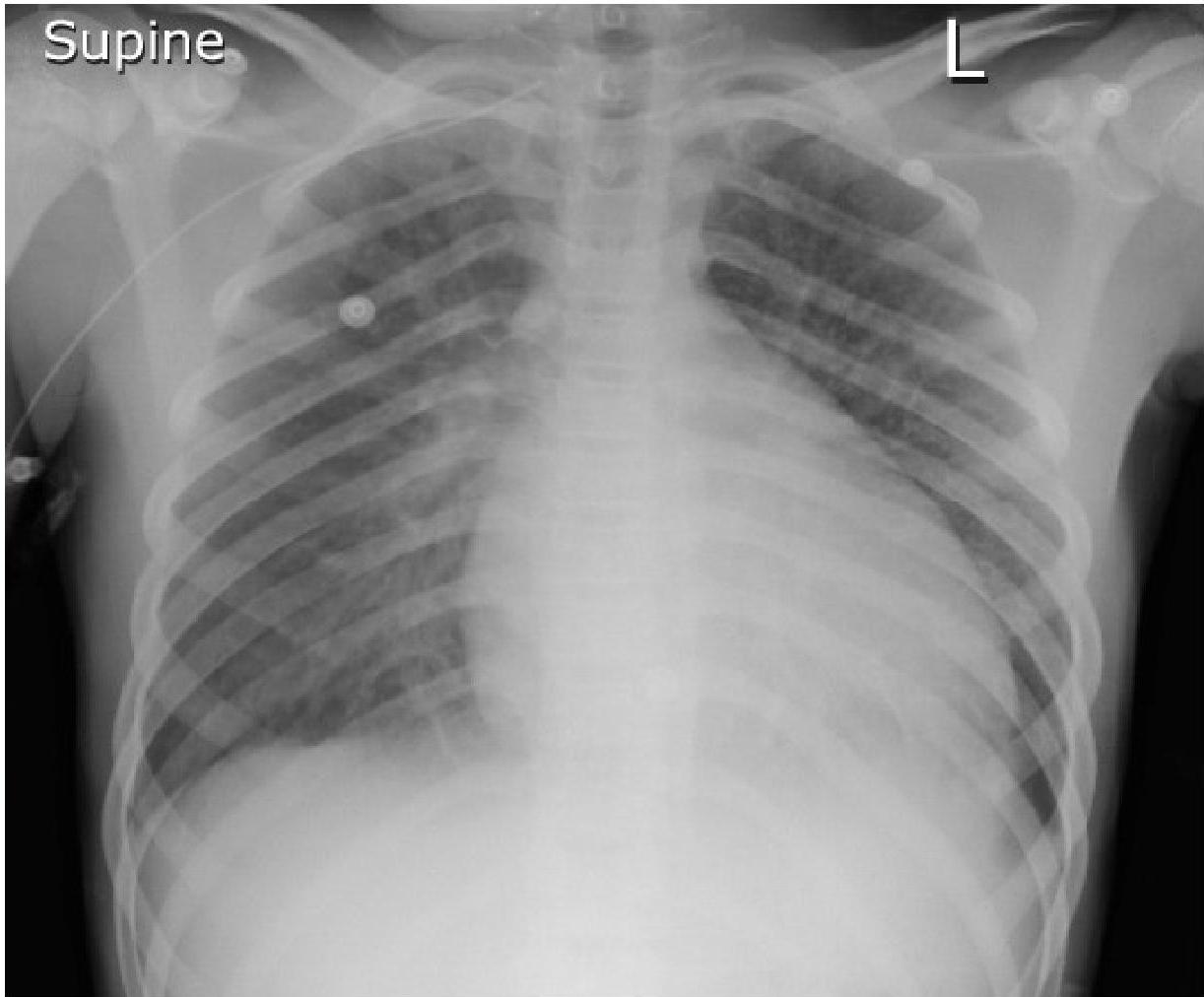
Chest Radiography
- Cardiomegaly: Left-to-right shunting defects, Dilated cardiomyopathy, Myocarditis, and Pericardial effusion.
- Pulmonary congestion/pulmonary edema.
- Pleural effusion.
- Pericardial effusion.
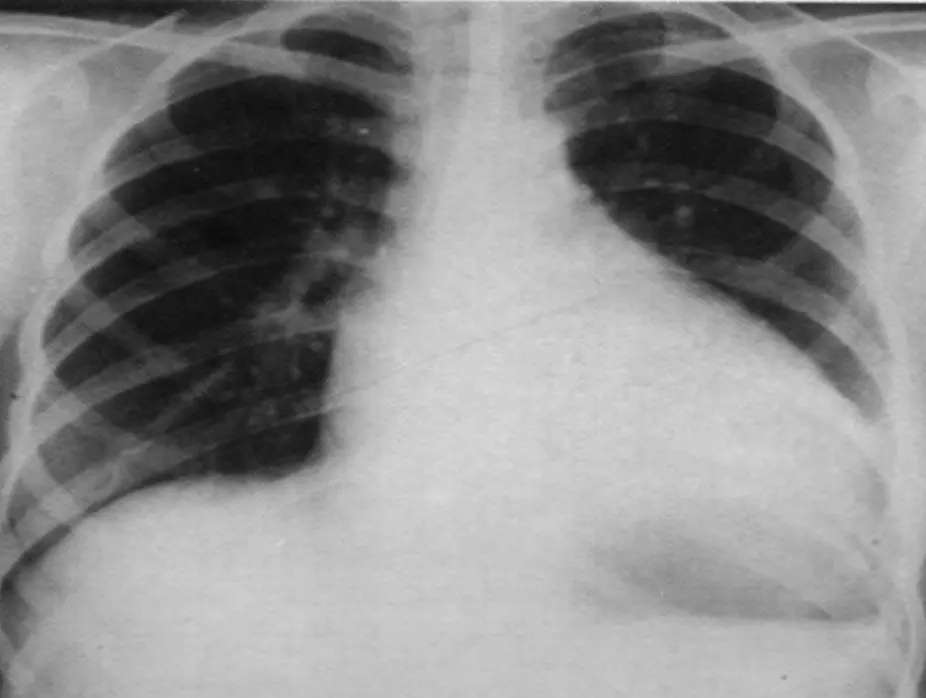
Chest radiograph of a 13-year-old boy with dilated cardiomyopathy
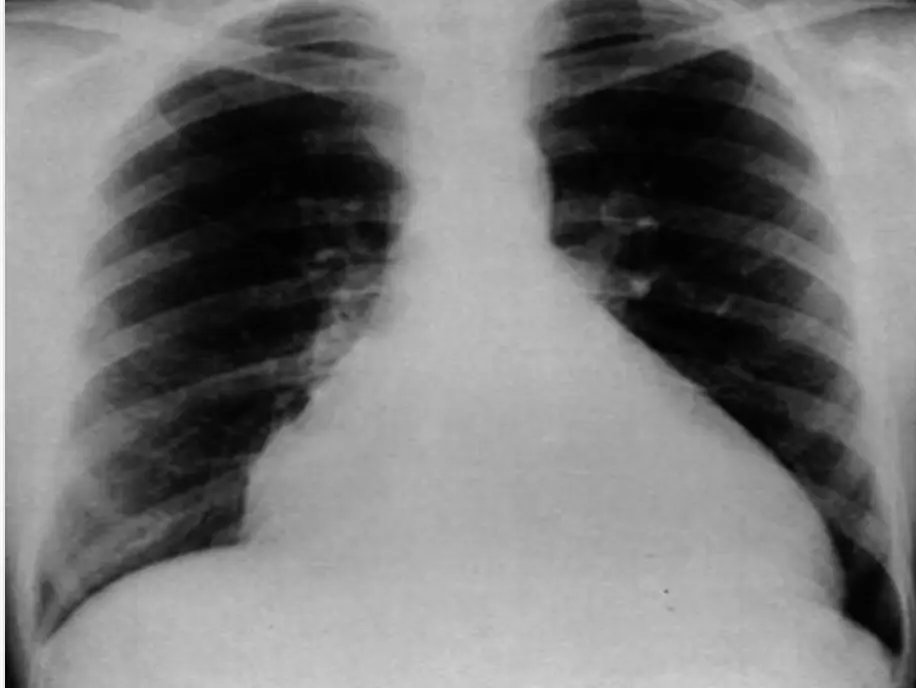
Chest radiograph in a 6-year-old patient with a large secundum atrial septal defect
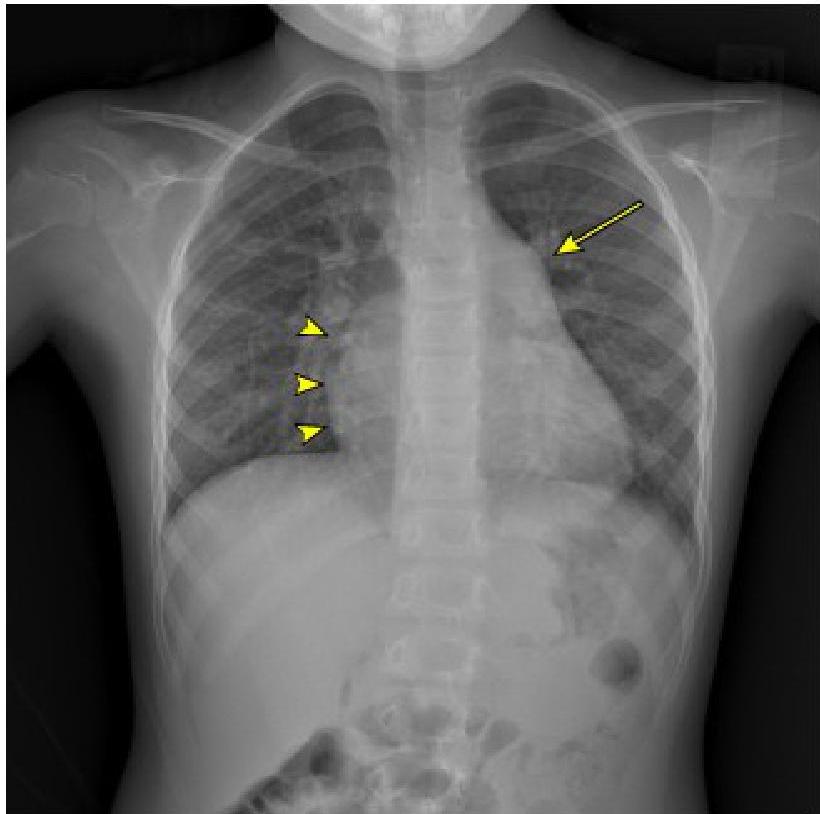 Demonstrates moderate cardiomegaly with increased convexity of the right side of the heart (arrowheads). There is a large pulmonary outflow tract (arrow) and increased pulmonary vascularity. Findings consistent with large left-to-right shunt.
Demonstrates moderate cardiomegaly with increased convexity of the right side of the heart (arrowheads). There is a large pulmonary outflow tract (arrow) and increased pulmonary vascularity. Findings consistent with large left-to-right shunt.
Electrocardiogram (ECG)
- Sinus tachycardia.
- ST segment and T wave abnormalities: Cardiomyopathy and myocarditis.
- Increased QRS voltage: Hypertrophic or dilated cardiomyopathy (VH).
- Decreased QRS voltage: Pericardial effusion and myocarditis.
- Bi-atrial enlargement: Restrictive cardiomyopathy.
- Deep Q wave in inferior and lateral leads (I, aVL, and V5-V6) with ST segment and T wave changes: Suggestive of myocardial infarct (ALCAPA).
- Varying degrees of heart block: Rheumatic fever or neonatal lupus.
- Arrhythmias (Atrial, junctional, or ventricular tachycardia or PAC or PVC): As an underlying cause of ventricular dysfunction or a complication.
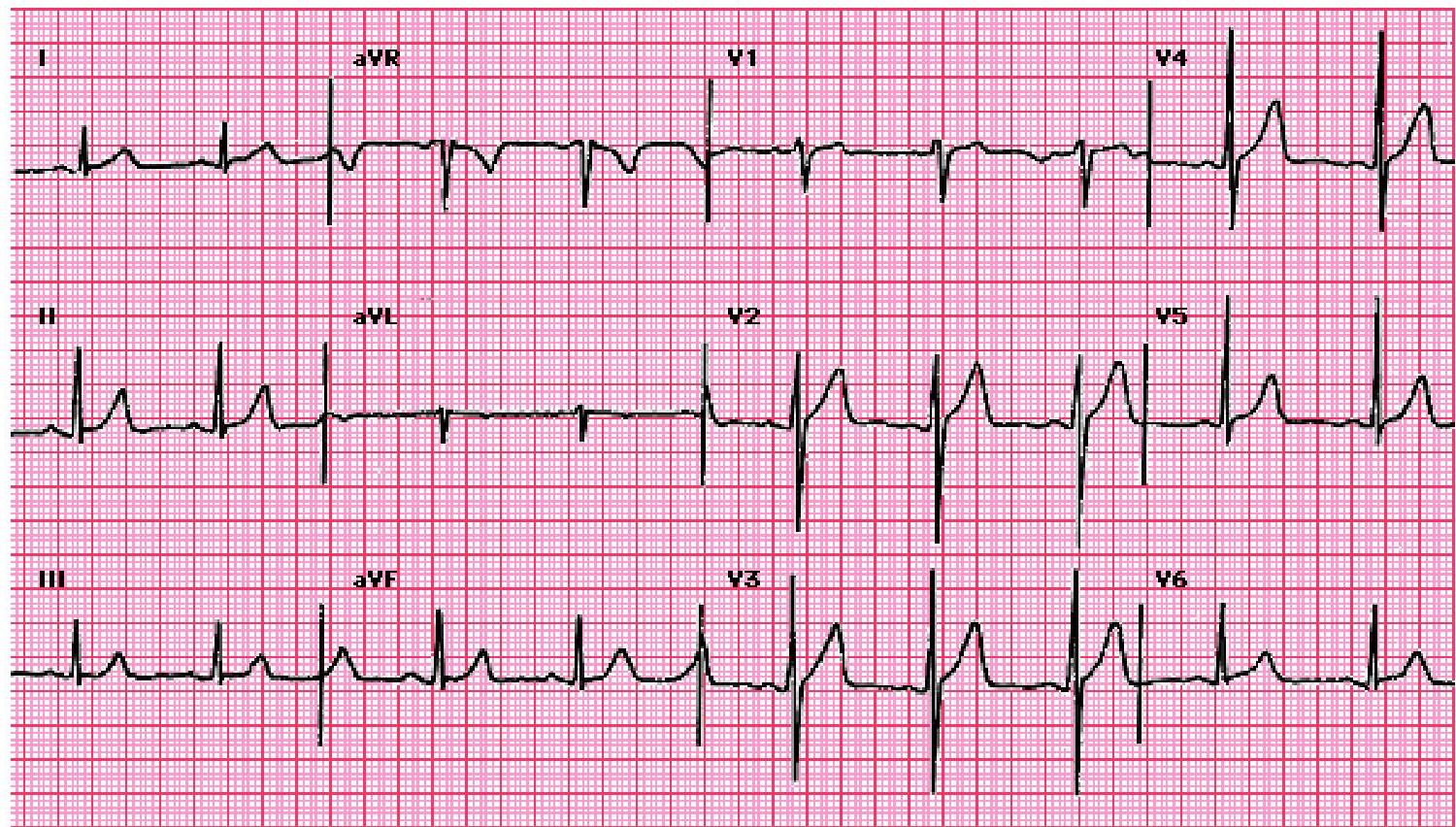
Left ventricular hypertrophy with strain pattern
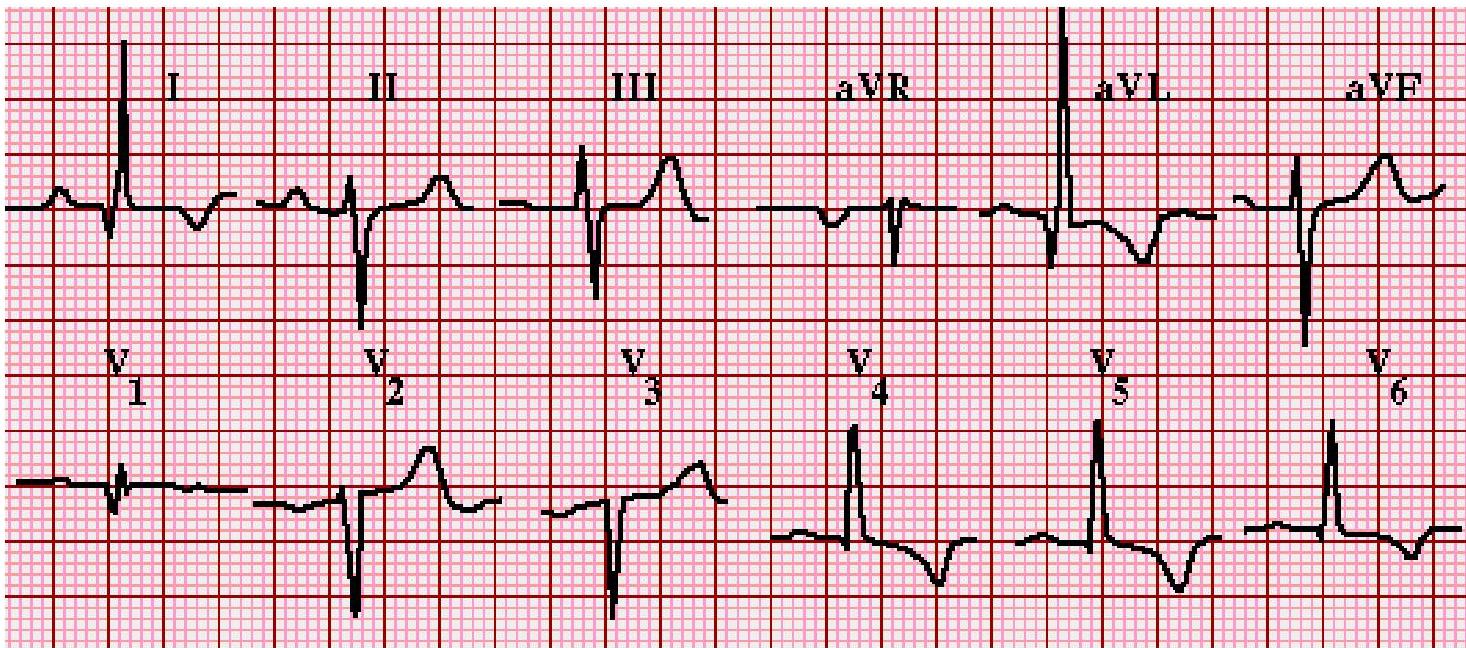 ST-T wave abnormalities secondary to LVH (“strain”) in anterolateral leads (I, aVL, V4-V6). Typical abnormalities include a horizontal or downsloping ST segment and T wave inversions. In some cases, there is concavity to the ST segment, which has a final downward turn that blends into an inverted T wave.
ST-T wave abnormalities secondary to LVH (“strain”) in anterolateral leads (I, aVL, V4-V6). Typical abnormalities include a horizontal or downsloping ST segment and T wave inversions. In some cases, there is concavity to the ST segment, which has a final downward turn that blends into an inverted T wave.
Normal ECG
 Normal sinus rhythm at 75 beats/minute, PR 0.14s, QRS 0.10s, QRS axis ~75°.
Normal sinus rhythm at 75 beats/minute, PR 0.14s, QRS 0.10s, QRS axis ~75°.
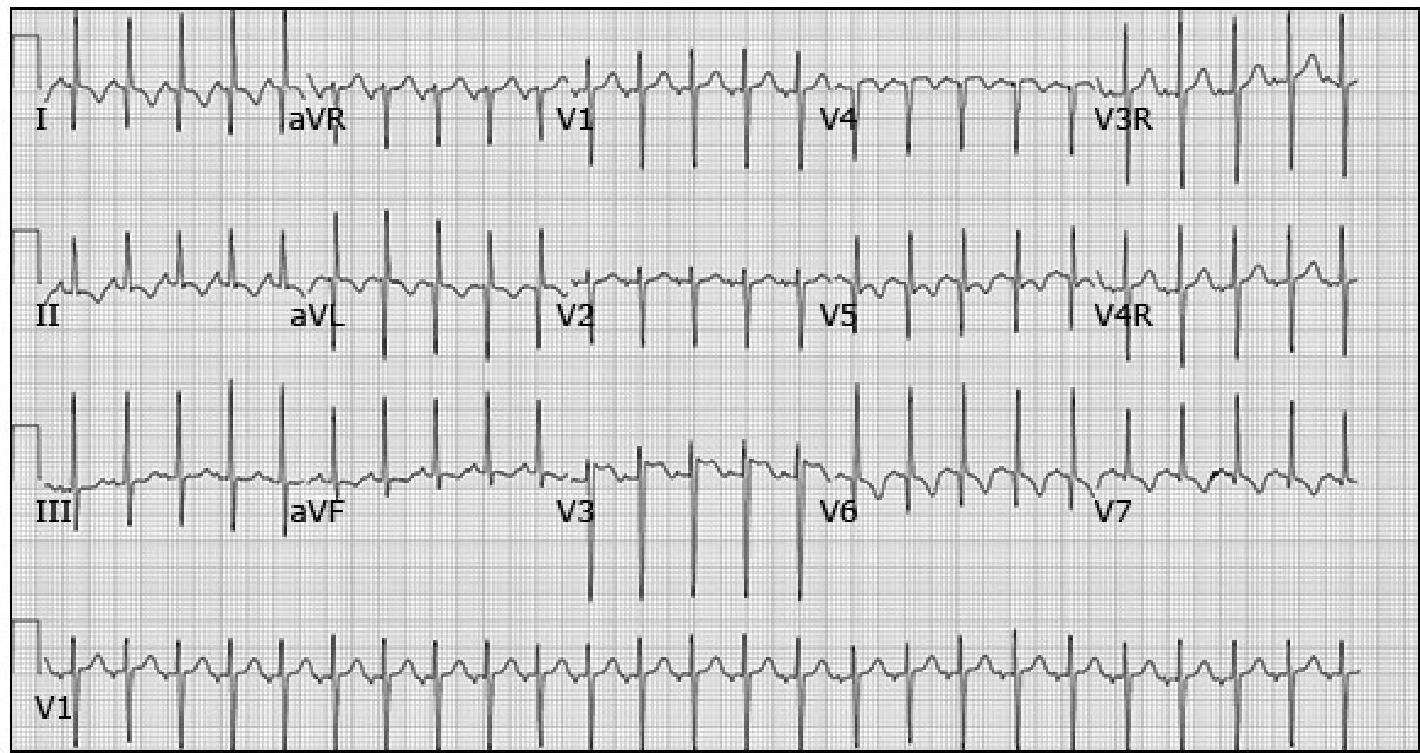
Electrocardiogram of 13-year-old boy with dilated cardiomyopathy
 Demonstrating increased QRS voltage with ST segment and T wave abnormalities.
Demonstrating increased QRS voltage with ST segment and T wave abnormalities.
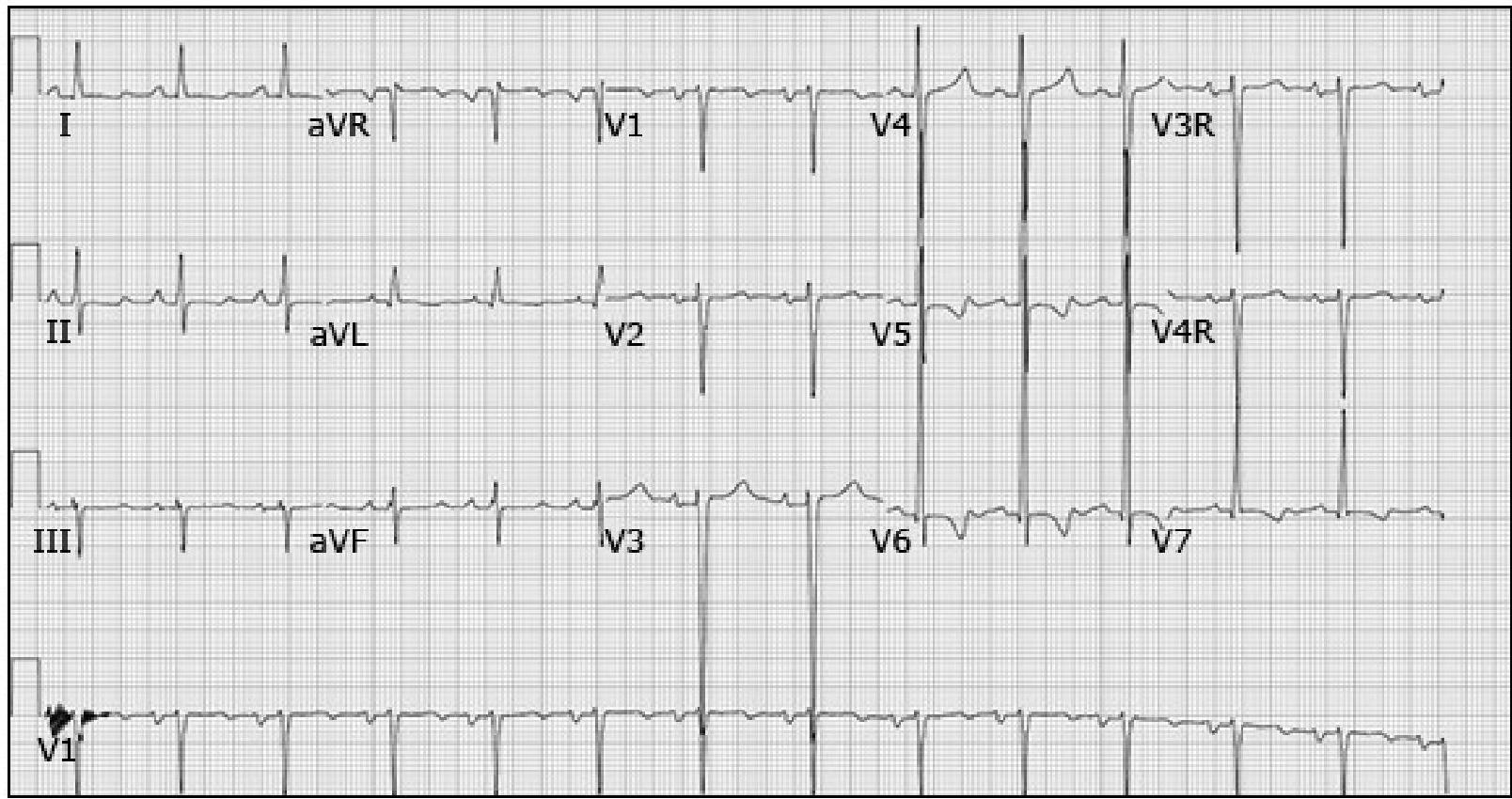
Electrocardiogram in a 10-week-old infant with ALCAPA
 Demonstrating deep Q waves in anterior and lateral leads (I, aVL, and V5-V6) with ST segment and T wave abnormalities.
Demonstrating deep Q waves in anterior and lateral leads (I, aVL, and V5-V6) with ST segment and T wave abnormalities.
First do x-ray then echocardiography espicially for pneumonia case suspected Z
Echocardiography
- Underlying structural congenital heart disease (CHD).
- Atrial and ventricular sizes (chamber size, wall thickness).
- LV and RV global and regional systolic function.
- LV diastolic function.
- Pericardial effusion.
- Estimation of RV and pulmonary artery pressures.
- Atrial or ventricular thrombi.
- Presence and amount of valvular stenosis and regurgitation.
Other Imaging and Testing
- Cardiac MRI: Accurate and detailed information regarding cardiac anatomy, ventricular function, myocardial inflammation, and infiltration by fat and fibrous tissues.
- Cardiac Catheterization: Coronary anatomy, endomyocardial biopsy, evaluate pulmonary vascular resistance (PVR) and vasodilator responsiveness.
- Holter Monitoring: If symptoms suggest arrhythmia.
- Exercise Testing: For children with cardiomyopathy to determine functional class and risk stratification.
Laboratory Observations
- Complete Blood Count and Iron Studies: Anemia may contribute to HF.
- Serum Electrolytes: Hyponatremia. Baseline electrolytes needed prior to initiating therapy with diuretics or ACE inhibitors.
- Urea and Creatinine: Kidney function impairment may be a contributing factor.
- Liver Function Tests: May be elevated due to hepatic congestion with right-sided HF.
- Blood Gases and pH: Acidosis.
- Glucose: Hypoglycemia.
- ESR: High ESR is a poor prognosis sign.
- Urinary Findings: Albuminuria.
Cardiac Biomarkers
- B-type Natriuretic Peptide (BNP) / NT-proBNP:
- Used to assess severity of HF and monitor response to therapy.
- Discriminates between cardiac and noncardiac causes (e.g., lung disease).
- Correlates with degree of shunting in ASD/VSD/PDA.
- In ventricular dysfunction, correlates negatively with ejection fraction.
- Correlates with functional class of HF and outcome.
- Troponin:
- Elevated in myocarditis and myocardial ischemia.
- In children with LV dysfunction, elevated troponin may suggest acute myocarditis rather than dilated cardiomyopathy.
HF DIFFERENTIAL DIAGNOSIS
- Respiratory Distress (Pulmonary Disorders):
- Neonates: TTN, RDS, meconium aspiration, pneumonia.
- Older infants/children: Pneumonia, bronchiolitis, asthma.
- Shock: Overwhelming sepsis, hypovolemia, IEM.
- Poor Weight Gain: Protein-milk allergy, cystic fibrosis, celiac disease.
- Peripheral Edema: Kidney failure, venous thrombosis.
MANAGEMENT
General Measures
- Reversible Contributors: Anemia, Hypertension, Renal failure, Acidosis, Malnutrition, Respiratory disorders (e.g., asthma, obstructive sleep apnea, interstitial lung disease), Thyroid disorders.
- Nutritional Support:
- Children with HF often have increased caloric needs due to an increased metabolic demand, often tire with feeding and their intake may be limited.
- Intermittent or continuous nasogastric or gastrostomy tube feeds may be required.
- Exercise and Physical Activity:
- Promoting safe physical activity is important.
- Recommendations tailored based on diagnosis and exercise capacity.
Medical Therapy
Goals & Strategy
- Goals: Relieve symptoms, slow progression, improve survival and quality of life.
- Unstable Patients: Presenting with shock require prompt treatment to restore perfusion.
- Structural Heart Disease (Preserved Function): Causing volume overload (e.g., VSD, ASD) or pressure overload (e.g., PS, AS), management is surgical or catheter-based interventions. Medical therapy is needed for stabilization or symptom relief while awaiting a more definitive intervention.
Therapy by Stage y
| HF Stage | Definition | Examples | Therapy Approach |
|---|---|---|---|
| Stage A (At Risk) | Patients at risk for HF who have normal cardiac function and chamber size. | • Exposure to cardiac toxic drugs. • Family history of heritable CM • Repaired or palliated CHD with normal ventricular function (e.g., ccTGA) • Duchenne muscular dystrophy. | HF-specific therapies generally not necessary. Predisposing conditions should be treated. |
| Stage B (Presymptomatic) | Evidence of systemic ventricular dysfunction on echo or other imaging who are asymptomatic (No past or present HF symptoms). | • History of anthracycline exposure with reduced LVEF • Repaired or palliated CHD with reduced ventricular function • Isolated LV noncompaction | ACE inhibitors (first choice). ARBs, beta blockers can be used. |
| Stage C (Symptomatic) | Evidence of systemic ventricular dysfunction on echo or other imaging who are symptomatic (including past or present HF symptoms). | • Symptomatic cardiomyopathy • Repaired or palliated CHD with symptomatic ventricular dysfunction | See detailed regimen below. |
| Stage D (Advanced) | Patients with end-stage HF requiring continuous infusion of inotropic agents, mechanical circulatory support, cardiac transplantation, or hospice care. | • End-stage state of any of the above examples. • There is marked impairment and symptoms at rest despite maximal medical therapy | Interventions: IV inotropes (milrinone), diuretics, Positive pressure ventilation, CRT, Heart transplantation. |
Stage C Regimen (Symptomatic Systemic Ventricular Dysfunction)
- Initial: ACE inhibitor or ARB plus Spironolactone.
- Fluid Overload: Oral Furosemide / Metolazone as needed.
- Persistent Dysfunction: Add Beta Blocker (e.g., Carvedilol / Metoprolol) after stabilization.
- Symptom Relief: Digoxin can be added if needed.
- Reassessment: Consider Angiotensin Receptor-Neprilysin Inhibitor (ARNI; Sacubitril-Valsartan) if tolerating full regimen.
- Severe Cases: If severe limitation, growth failure, intractable arrhythmias, or restrictive CM, consider early referral for Heart Transplant.
Other Measures
- Oxygen.
- Prostaglandin.
- Morphine.
- Noninvasive Ventilation: High-flow nasal cannula (HFNC), CPAP.
- Position.
- Bed rest.
Nonpharmacologic Interventions for Advanced HF
- Cardiac Resynchronization Therapy (CRT):
- For advanced HF unresponsive to medical therapy, esp. reduced EF (<35%) and LBBB pattern.
- LBBB/conduction delay worsens HF via dyssynchrony; CRT uses biventricular pacing to minimize this.
- Extracorporeal Membrane Oxygenation (ECMO):
- Total heart-lung bypass device.
- Used for Postcardiotomy shock or Acute Myocarditis.
COMPLICATIONS
- Thromboembolism: Risk of intracardiac thrombi, pulmonary embolus, cerebral embolic strokes, death (due to systemic ventricular dysfunction).
- Arrhythmias: Sustained atrial/ventricular tachyarrhythmias can rapidly impair hemodynamics.
- Sudden Cardiac Death (SCD):
- ICD (Implantable Cardioverter Defibrillator) indicated for patients at risk (ventricular arrhythmia, history of unexplained syncope, or recurrent sustained ventricular dysrhythmias).
PROGNOSIS & COUNSELING
- Mortality: Ranges from 6 - 15% among hospitalized children.
- Risk Factors for Mortality: Comorbid renal/respiratory failure, symptoms at diagnosis (DCM), neuromuscular disease, lower LV shortening fraction.
- Note: Myocarditis is associated with better survival compared to some other causes.
- Medical Management Success: Improves outcomes in 60% of NYHA/Ross Class II/III patients.
- Counseling Factors: Severity of underlying condition, control of arrhythmias, new therapy modalities, cardiac transplantation availability.
- Transplantation Stats:
- Mortality highest in first year post-transplant.
- Median survival ranges from 13 to 22 years.