PART 3: CONGENITAL ADRENAL HYPERPLASIA (CAH)
ADRENAL PHYSIOLOGY
There are three pathways in adrenal gland to synthesize adrenal hormone: aldosterone, cortisol, and androgens.
- Zona Glomerulosa (Pathway 1) → Aldosterone
- Zona Fasciucalata (Pathway 2) → Cortisol
- Zona Reticularis (Pathway 3) → Androgens
CLINICAL FEATURES OF ADRENAL INSUFFICIENCY
Aldosterone Deficiency
- Hyponatremia and urinary sodium wasting
- Hyperkalaemia
- Dehydration, shock
- Hypotension
- Acidosis
- Vomiting and diarrhea
Cortisol Deficiency
- Hypoglycaemia
- Inability to withstand stress
- Hyperpigmentation
- Muscle weakness and fatigue
Androgen Deficiency
- Ambiguity in males only
- (Unaffected females)
Androgen Excess
- Virilization in females
- Ambiguity in females
- (Unaffected males)
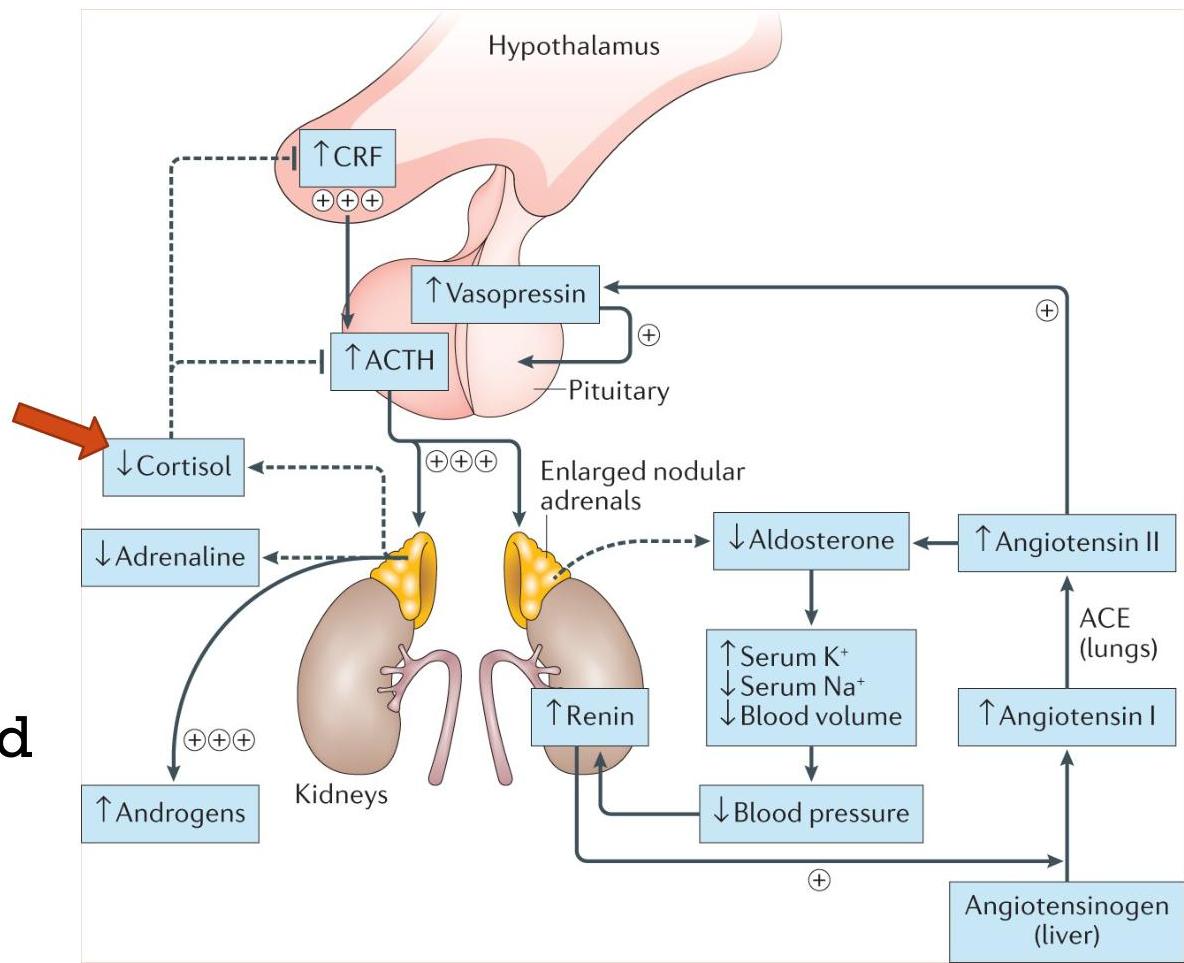
CONGENITAL ADRENAL HYPERPLASIA (CAH) OVERVIEW
It is an autosomal recessive disorder caused by enzymatic defects in cortisol synthesis. As a result, defect in pathway of adrenal hormone synthesis results.
- Deficient cortisol causes a rise in corticotropin releasing hormone (CRH) and adrenocorticotropic hormone (ACTH), which stimulates adrenal hyperplasia.
- Whenever any of the mentioned enzyme is absent (according to the type), adrenal androgen and steroid precursors prior to the enzyme defect accumulate.
Types:
- 21-OH deficiency (most common)
- 11β-OH deficiency (second most common)
- 17α-OH deficiency
SPECIFIC CAH TYPES
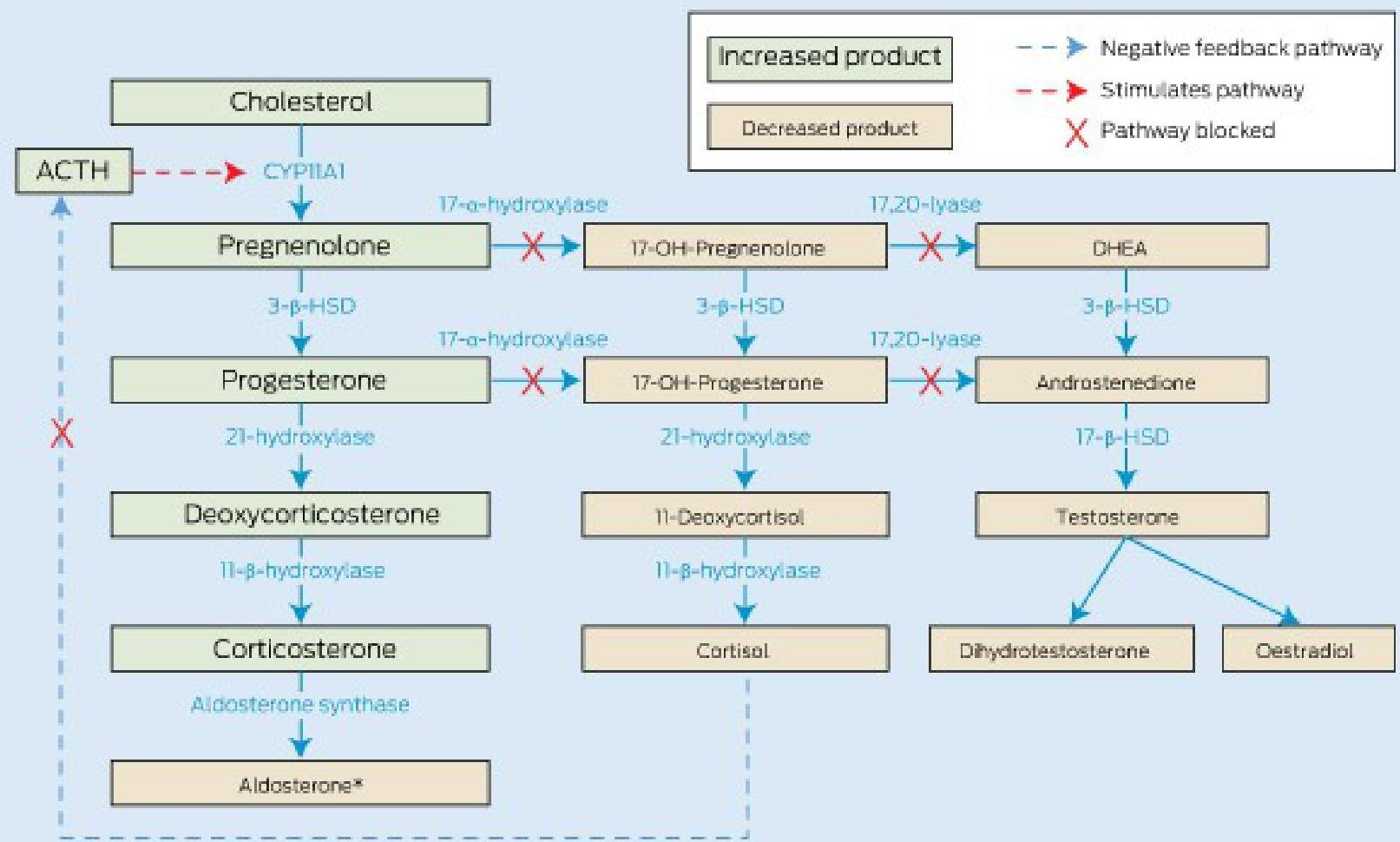
1. 21-HYDROXYLASE DEFICIENCY
Hallmark: ↑ 17-hydroxyprogesterone
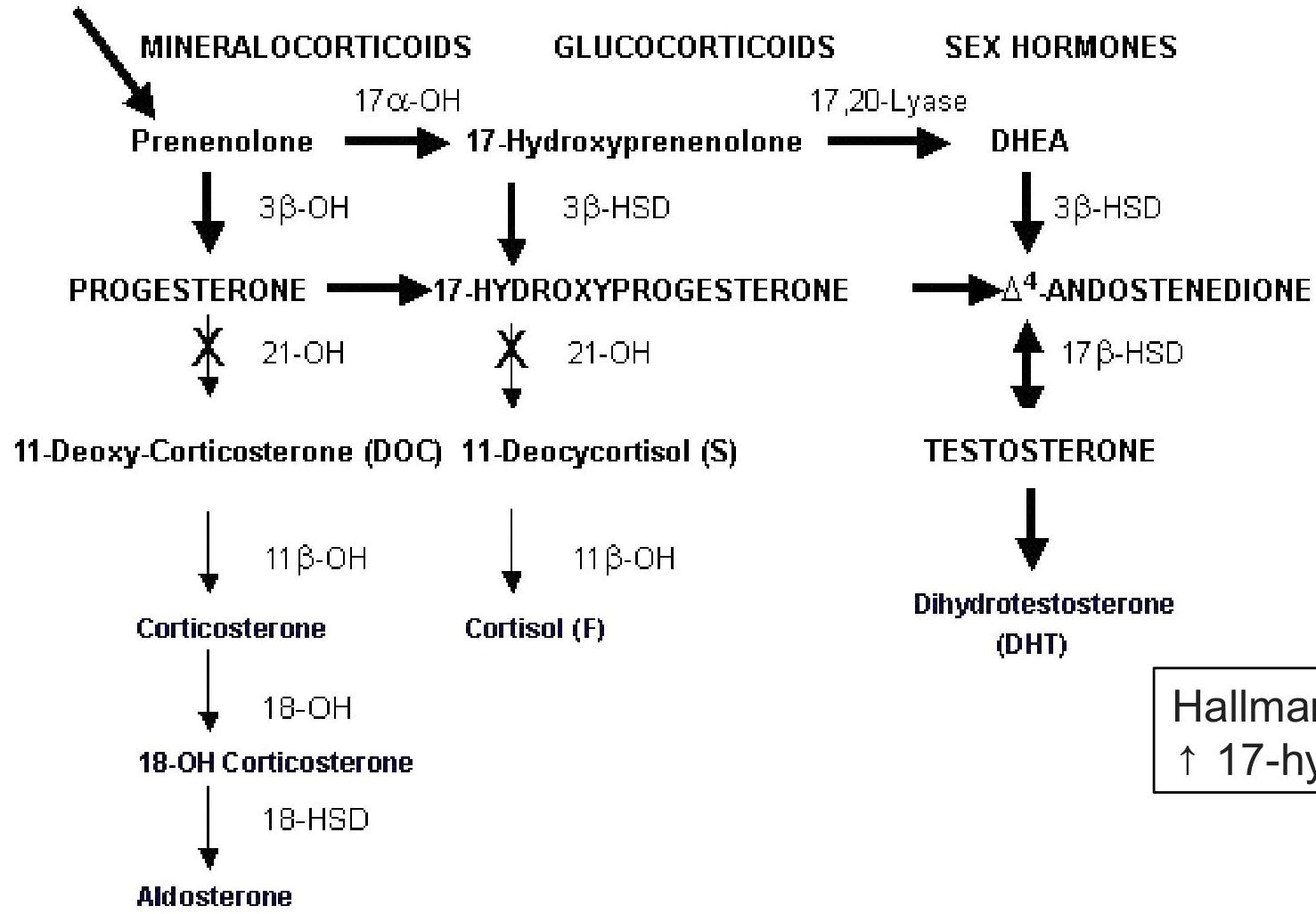
Pathophysiology: Deficient 21-hydroxylase activity:
- Impairs the conversion of 17-hydroxyprogesterone (17-OHP) to 11-deoxycortisol causing deficiency of cortisol.
- Impairs the conversion of progesterone to deoxycorticosterone causing deficiency of aldosterone.
- There will be overproduction of androgens due to increased level of ACTH resulting in hyper virilization.
Clinical Features:
- Hyperpigmentation especially of genital area.
- Salt Wasting: Hyponatremia and Hyperkalemia (occurring later at 2-3 weeks of age). Z
- Note: This happens in male babies as they will not be early diagnosed because of the normal external organs. They present with dehydration, hyponatremia, hyperkalemia, and shock. Z
- Hypoglycemia (occurring later at 2-3 weeks of age).
- Genitalia:
- In Females: Ambiguity. The development of the uterus, ovaries, and fallopian tubes is unaffected by the androgens. However, the degree of virilization varies, ranging from mild clitoromegaly to complete fusion of labioscrotal folds, with severe clitoromegaly simulating a phallus (Ambiguous Genitalia).
- In Males: A male infant with this defect appears normal at birth, therefore they present later at age of 2-3 weeks with dehydration, HPONATREMIA, HYPERKALEMIA, and shock due to deficiency in aldosterone. z
Labs:
- High 17 (OH) progesterone
- High androstenedione
- High ACTH
- Electrolyte imbalance
- Low glucose level
Treatment: In acute setting:
- Aggressive fluid administration for hypotension and acidosis. z ressus
- Hydrocortisone stress dose (50-100mg/kg stat dose IV). Z
- Dextrose bolus/infusion to treat hypoglycaemia. z
After stabilizing patient: 4. Admission under Endocrinology team. 5. Long-term therapy consists of providing oral hydrocortisone. To avoid adrenal insufficiency, threefold higher doses of glucocorticoids are given during stressful states, such as febrile illnesses and surgery. 6. Fludrocortisone supplement as mineralocorticoid alternative. Dose and response is monitored with serum sodium, potassium, and plasma renin activity levels. 7. Sodium chloride supplementation as needed. 8. Plastic Surgery consultation for Surgical correction of ambiguous external genitalia may be considered. Z 9. Annual assessment of linear growth and skeletal age.
2. 11β-HYDROXYLASE DEFICIENCY
Hallmark:
- Increased 11-deoxycortisol
- Increased 11-deoxycorticosterone (DOC)
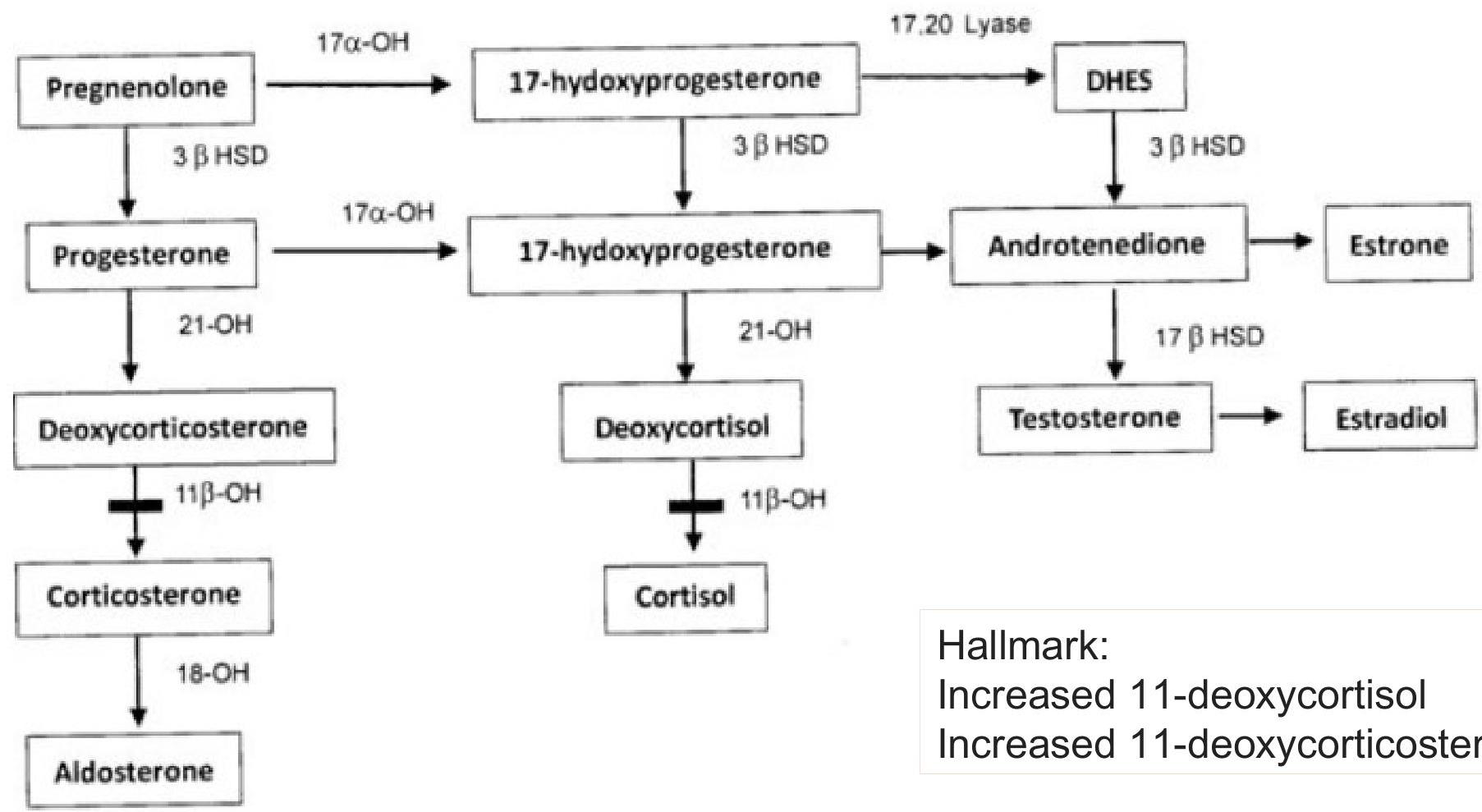
Pathophysiology: Deficiency in 11β-hydroxylase prevents the conversion of:
- 11-deoxycortisol to cortisol
- 11-deoxycorticosterone to corticosterone
Clinical Features:
- Hyperpigmentation especially of genital area.
- Salt Wasting: Hyponatremia (occurring later at 2-3 weeks of age). This happens in male babies as they will not be early diagnosed because of the normal external organs.
- Hypoglycemia (occurring later at 2-3 weeks of age).
- Ambiguity in females.
- Normal external organs in males.
- HYPERTENSION and hypokalemia due to accumulation of deoxycorticosterone (DOC).
Labs:
- High ACTH
- Increased levels of 11-deoxycortisol and 11-deoxycorticosterone
- Electrolyte imbalance
- Hypoglycemia
- Increased sex steroid synthesis
3. 17α-HYDROXYLASE DEFICIENCY
Hallmark:
- ↓ 17 OH pregnenolone
- ↓ 17 OH progesterone
Clinical Features:
- Ambiguity in male
- Delayed puberty in both genders
- Hypoglycemia and hyperpigmentation
- HYPERTENSION and hypokalemia due to accumulation of deoxycorticosterone (DOC)
Labs:
- ↑ DOC
- ↑ Corticosterone
- ↑ Mineralocorticoids: hypernatremic hypokalemic
- ↑ ACTH
COMPARISON AND SUMMARY
Table: 11-beta vs 17-alpha Hydroxylase Deficiency
| 11-beta HYDROXYLASE | 17-alpha hydroxylase |
|---|---|
| Blood pressure increased | Blood pressure increased (implied) |
| Male: Normal genitalia, but Precocious puberty | Male: Ambiguous |
| Female: Ambiguous, hirsutism and virilisation | Female: Normal but amenorrhea |
| Androgen pathway will increase | Aldosterone pathway will increase |
| Severe hypokalemia | (Hypernatremic hypokalemic) |
Important Clinical Notes
- The dominant clinical features of congenital adrenal mineralocorticoid deficiency are hyponatremia and hyperkalemia, usually developing by 5–7 days after birth. (Mainly presented in boys because in girls the defect is detected at birth due to ambiguous genitalia).
- Vomiting, dehydration, and acidosis soon follow, as does hypotensive shock from glucocorticoid deficiency.
- Hyperpigme ntation of the scrotal skin will be present at birth resulting in delayed diagnosis.
- In females, the ambiguity of the external genitalia may be the first detected sign and it can be an obvious clue that it is congenital adrenal hyperplasia (CAH).
- Accelerated growth and skeletal maturation due to excess postnatal exposure to adrenal androgens may occur.
Diagnostic Differential Reminder:
- In Pyloric Stenosis: Vomiting of stomach contents results in Hypochloremic, Hypokalemic Alkalosis.
- In contrast to CAH, which has Hyponatremia, Hyperkalemia, and Acidosis.