PART 2: DISORDERS OF SEX DEVELOPMENT (DSD) & AMBIGUOUS GENITALIA
AMBIGUOUS GENITALIA
Ambiguous genitalia is a birth defect where the outer genitals do not have the typical appearance of either a boy or a girl. If a clinical decision about the child gender is difficult to make, the child has ambiguous genitalia. Definition may also include bilateral undescended testicles, as well as hernias in females especially if a gonad is palpable.
The term disorder of sex development (DSD) is the term used for intersex problems, identified by one of the following:
- Genetic differentiation: i.e., Fertilization.
- Gonadal differentiation:
- XY: The testes determining factor (SRY gene) will influence the gonad to differentiate to be a testicle.
- XX: The gonad differentiates to be an ovary.
- Phenotypic differentiation:
- Internal organs: The testosterone produced locally by the testicle will influence the male organs to develop (Wolffian tubes, epididymis, and seminal vesicles). The Mullerian inhibitory factor (MIF) produced locally by the testicle will inhibit internal female organs to develop.
- Vice-versa if the gonad is an ovary there is no testosterone, so the male structures regress and as there is no MIF, thus the Mullerian structures develop (fallopian tube, uterus, upper part of vagina).
CAUSES OF DISORDER OF SEX DEVELOPMENT (DSD)
A) 46 XX DSD
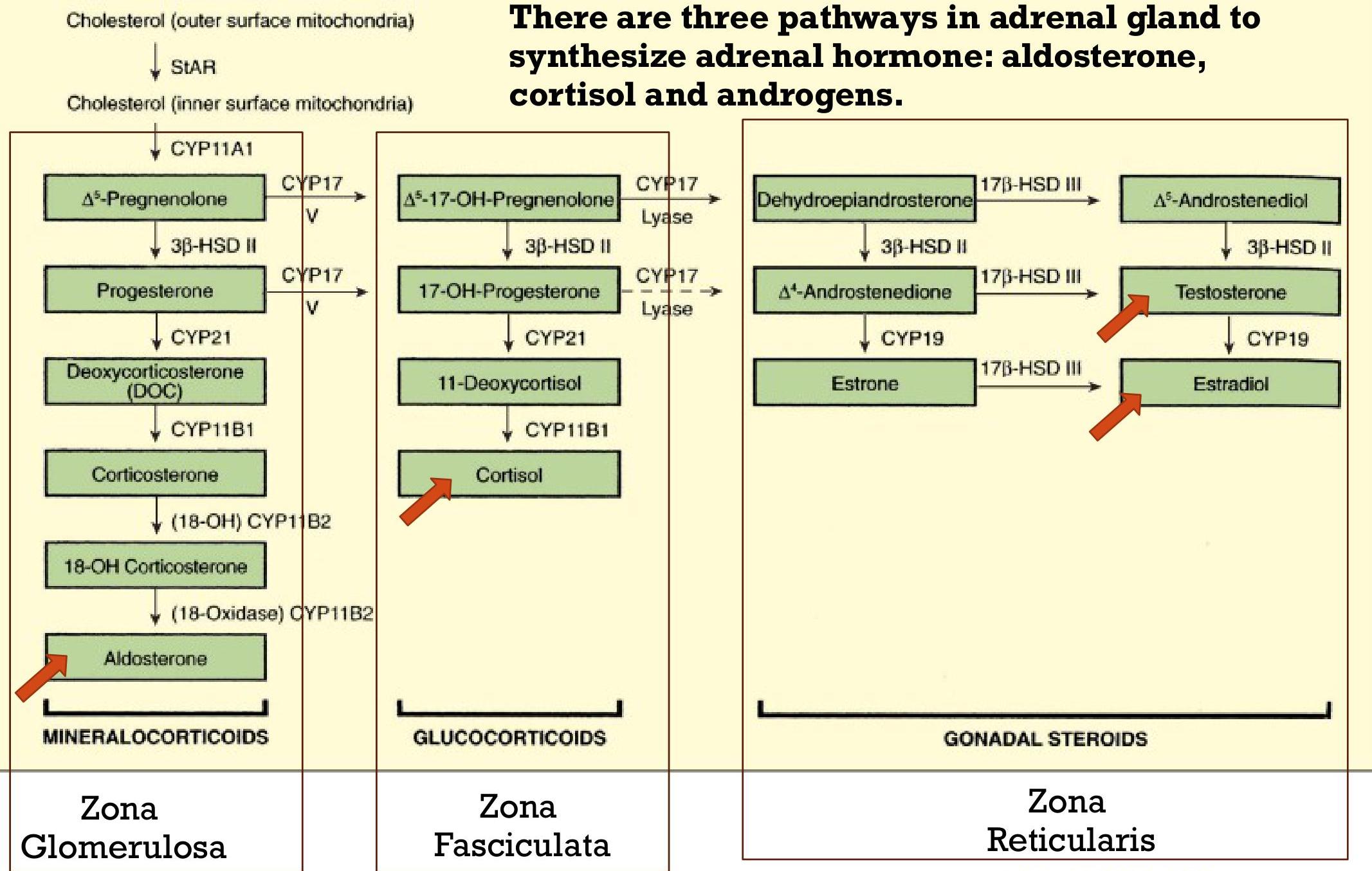
- Fetal: Congenital adrenal hyperplasia (CAH) due to defect in adrenal hormone synthesis secondary to deficiency in enzymes 21-hydroxylase or 11-hydroxylase, adrenal tumor.
- Maternal: External exposure to androgen, ovarian or adrenal cyst or tumor.
B) 46 XY DSD
- Pituitary: Panhypopituitism.
- CAH due to 5-alpha reductase deficiency.
APPROACH TO AMBIGUOUS GENITALIA
1. Brief History
- Similar family history.
- Previous history of neonatal death.
- FH of precocious puberty.
- Delayed puberty, anosmia (inability to smell).
- Irregular cycles.
- History of consanguinity.
- Maternal exposure to androgens or virilization.
2. Careful Examination
- General examination: For major defects especially midline defects or hyperpigmentation, hydration status, jaundice.
- Local Exam: Phallus-like structure (not penis or clitoris), Labioscrotal folds (not labia or scrotum).
- Inspect anus and examine hips.
3. Approach the Parents
- Talk to the family and tell them that you cannot decide, and you need to do certain investigations and advise them not to give a name.
- If you are not in a tertiary center, transfer the baby to one.
- If the child presentation is late and has a name already, continue as it is till you know the gender.
4. Investigations
- Ask for karyotype (XX or XY).
- Ask for an ultrasound and genitogram.
- Look for the defect or enzyme deficiency in adrenal hormone synthesis pathway.
- Monitor electrolytes (salt loss crises usually happen in the second or third week of life).
- VBG (Venous Blood Gas).
- Blood pressure.
- Glucose level.
5. Team Consultation
- Call urology and plastic surgery team for surgical correction.