PART 1: HYPOTHYROIDISM
CONGENITAL HYPOTHYROIDISM (CHT)
Most children with congenital hypothyroidism (CHT) are not symptomatic at birth; therefore, we do a newborn screening test through a Guthrie card. You will see high TSH.

A) Etiology: Congenital Hypothyroid
It is due to defective thyroid development as a result of:
- Thyroid agenesis or hypoplasia
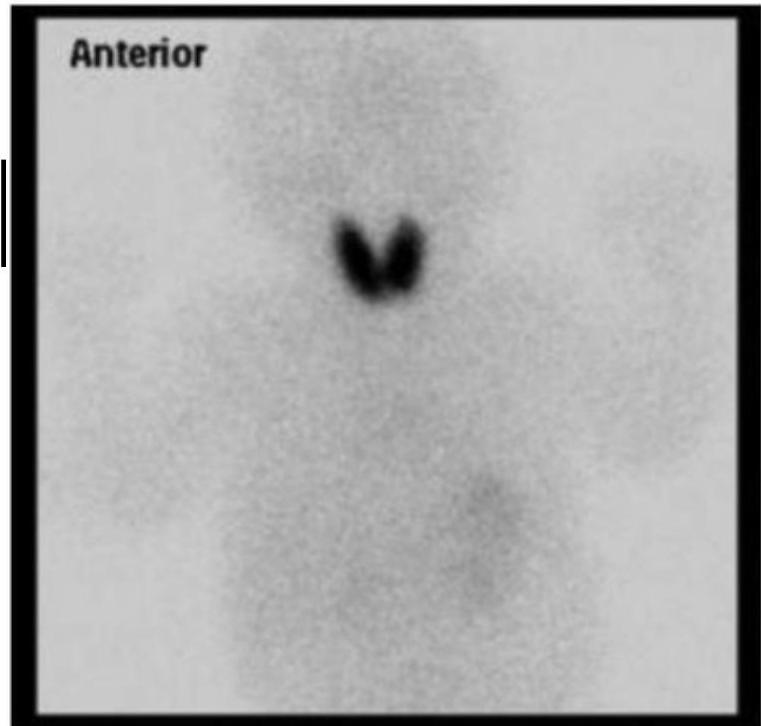
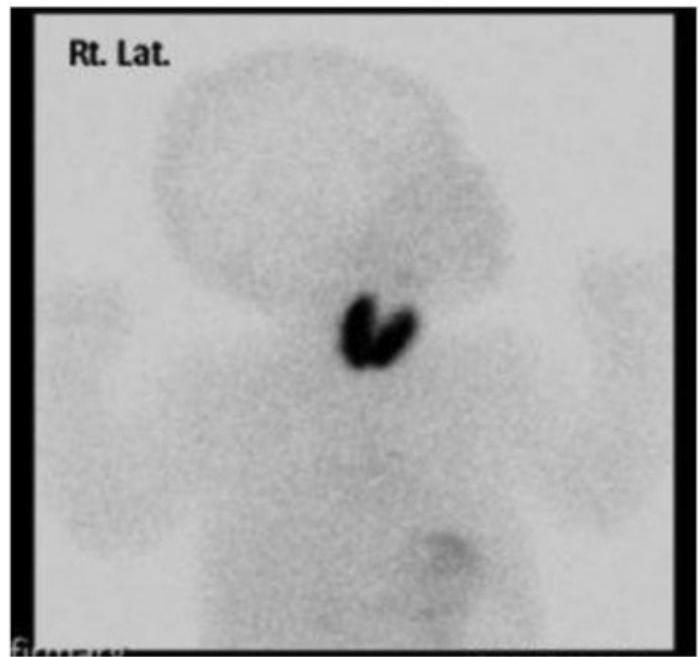
- Ectopic thyroid gland
- Dyshormonogenesis (gene mutations for thyroid hormones enzymes and proteins)
B) Etiology: Acquired Hypothyroidism
It usually presents in the older child, and it may be due to:
- Iodine deficiency (transient)
- Autoimmunity (Hashimoto’s thyroiditis)
- Thyroidectomy or irradiation
- Maternal anti-thyroid drugs (transient) (e.g., methimazole and propylthiouracil)
- Diseases of the pituitary and hypothalamus (central)
CLINICAL PRESENTATION
Neonates
Most infants are asymptomatic at birth because of the transplacental passage of maternal T4.
- Prolongation of physiologic jaundice
- Poor feeding, especially sluggishness
- Somnolence and choking spells during feeding
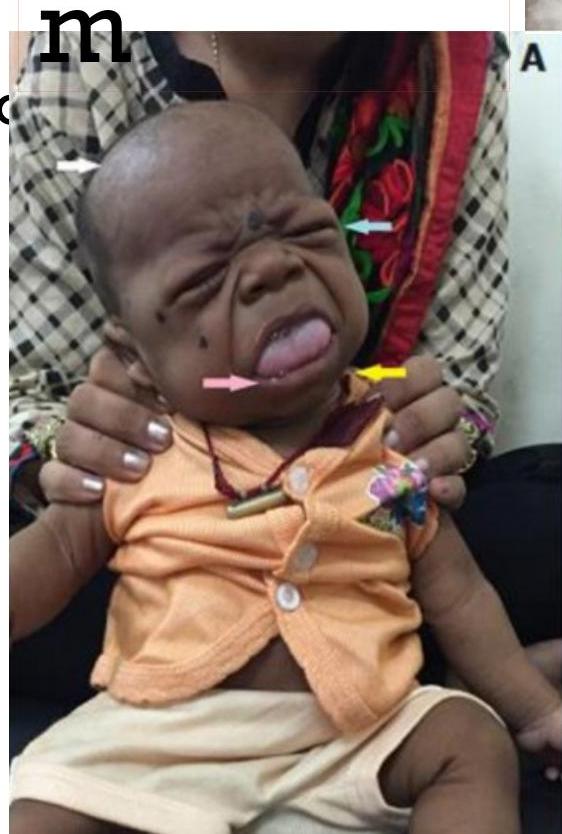
- Large protruded tongue
- Umbilical hernia
- Cold, mottled, dry skin
- Large anterior fontanelle
- Delayed developmental milestones
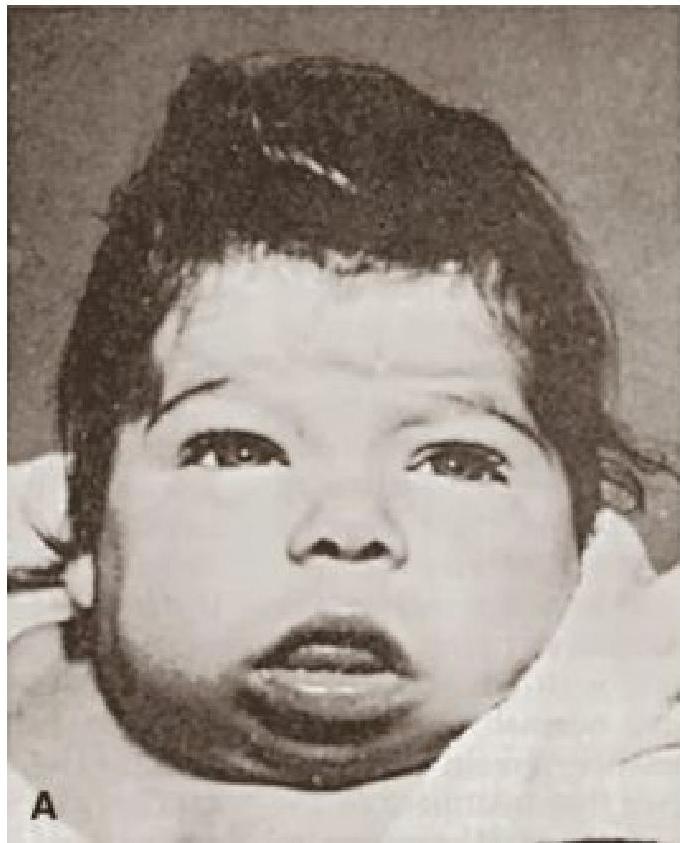
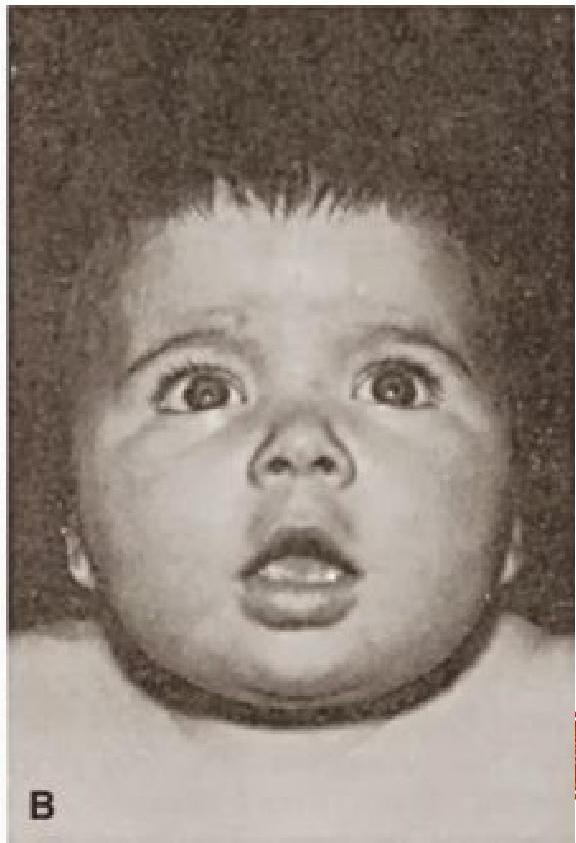
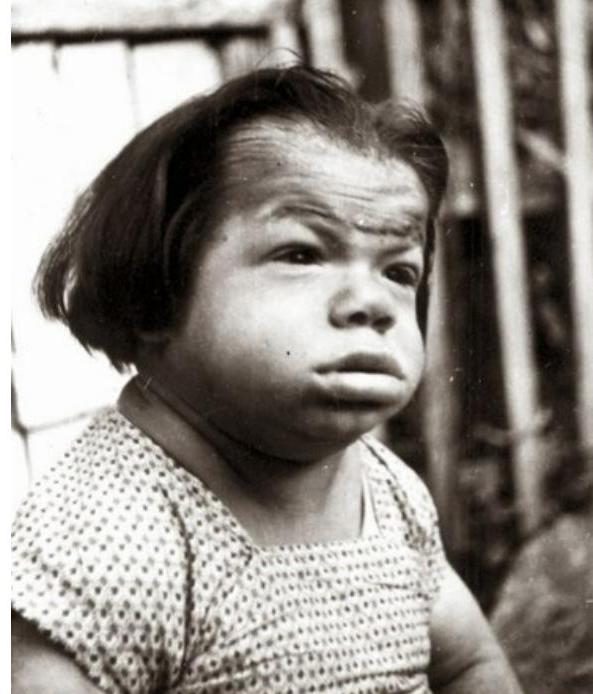
- Coarse facies


Older Children
Older children will present with:
- Suboptimal height velocity
- Excessive weight gain
- Constipation not responding to regular treatment
- Deteriorating school progress from slowed mentality
- Cold intolerance
- Delayed puberty
- Dry skin and sparse brittle hair
- Goitre
- Bradycardia
- Proximal muscle weakness

Manifestations by Pathophysiology
Decreased Metabolic Rate Symptoms & Signs:
- Fatigue and weakness
- Cold intolerance
- Dyspnea on exertion
- Weight gain
- Cognitive dysfunction
- Mental retardation (infant)
- Constipation
- Growth failure
- Bradycardia
- Delayed Speech
- Delayed relaxation of tendon reflexes
Matrix Protein Accumulation Symptoms & Signs:
- Dry skin
- Hoarseness
- Edema
- Coarse skin
- Puffy facies and loss of eyebrows
- Periorbital edema
- Enlargement of the tongue
Other Manifestations
- Decreased hearing
- Myalgia and paresthesia
- Depression
- Menorrhagia
- Arthralgia
- Pubertal delay
- Diastolic hypertension
- Pleural and pericardial effusions
- Ascites
- Galactorrhea
NEWBORN SCREENING AND DIAGNOSIS
- Newborn screening is crucial to make an early diagnosis and to initiate thyroid replacement therapy by younger than 1 month of age.
- Most thyroid-dependent brain maturation occurs in the first 2 years after birth.
- Part of the routine neonatal screening programs is to measure cord blood or heel stick TSH values (Guthrie card).
- An immediate confirmatory serum sample should be obtained from any infant having a positive result (high TSH) on a screening test.
- A serum result of low free T4 and high TSH confirm congenital hypothyroidism and levothyroxine must be started as soon as possible.
- Congenital hypothyroidism detected by the newborn screening programme allows adequate treatment to begin within 2 weeks of life and can optimise a child’s growth and development.
- In neonates and infants, delayed treatment of thyroid dysfunction may cause permanent nervous system damage, developmental delay, and cretinism.
- Cretinism is defined as permanent severe mental retardation with coarse facial features, short stature, and seizures.
CLINICAL LAB FINDINGS
Table 175.1: Laboratory Test Results in Various Types of Thyroid Function Abnormalities in Children
| ABNORMALITY | SERUM TOTAL T4 | SERUM FREE T4 | SERUM TSH | (transporter) SERUM TBG |
|---|---|---|---|---|
| Primary hypothyroidism | ↓ | ↓ | ↑ | N |
| Hypothalamic (TRH) tertiary hypothyroidism | ↓ | ↓ | ↓ | N |
| Pituitary (TSH) secondary hypothyroidism | ↓ | ↓ | ↓ | N |
| TBG deficiency Z | ↓ | N | N | ↓ |
| TBG excess z | ↑ | N | N | ↑ |
*TSH may be slightly elevated. Key: ↓, Decreased; ↑, increased; N, Normal; T4, thyroxine; TBG, thyroxine-binding globulin; TRH, thyrotropin-releasing hormone; TSH, thyroid-stimulating hormone.
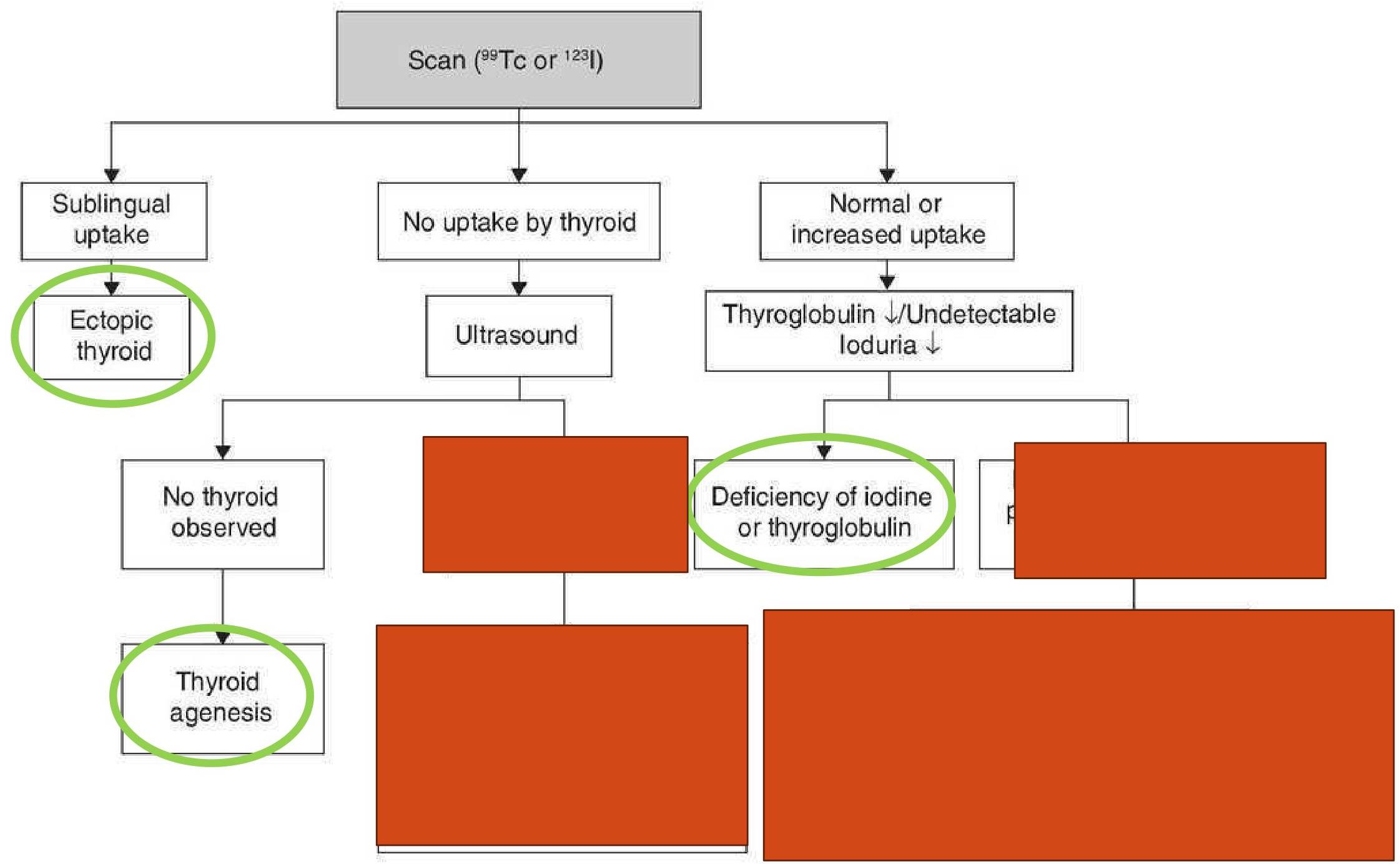
Specific Diagnostic Patterns
Thyroid Aplasia
- Low TSH
- No goiter
- No uptake of iodine
Dyshormogenesis
- High TSH (ineffective)
- Low T4
- Goiter
Poor Compliance
- Normal T4
- High TSH
Central Hypothyroidism
- Initially: Normal TSH and low T4
- Followed by: Low TSH and Low T4
HASHIMOTO THYROIDITIS
- Also known as autoimmune or lymphocytic thyroiditis.
- A family history of thyroid disease is present in 25–35% of patients.
- Caused by autoimmune inflammation of the thyroid gland attacked by the following antibodies:
- Anti-thyroid peroxidase antibodies
- Anti-thyroid antiglobulin antibodies
- First a transient hyperthyroidism is presented due to increase in TSH and TRH then hypothyroidism develop due to loss of thyroid receptors lost by autoimmune attack as well as fibrosis and atrophy of the thyroid gland.
- On examination you may notice: diffuse goiter with a pebble-like surface.
- Onset typically occurs after 6 years of age with a peak incidence in adolescence with a female predominance.
Diagnosis and Approach
- The diagnosis may be confirmed by serum antithyroid peroxidase and antithyroglobulin antibodies.
- Neither biopsy nor thyroid scan is indicated in Hashimoto thyroiditis Z.
- Goal of treatment with thyroid hormone sufficient to normalize TSH and free T4 is indicated for hypothyroidism in Hashimoto thyroiditis.
- Patients without manifestation of hypothyroidism require thyroid function testing (serum TSH and free T4) every 6–12 months to detect the later development of hypothyroidism. Z
- Goiter with a normal TSH usually is not an indication for treatment.
TREATMENT OF HYPOTHYROIDISM
- The aim of therapy for congenital hypothyroidism is to normalise free T4 within 2 weeks and TSH within the first month of life.
- An optimal cognitive outcome depends on both the adequacy and timing of postnatal therapy.
- Medication: Levothyroxine.
- If therapy is instituted after 6 months, when the signs of severe hypothyroidism are present, the likelihood of normal intellectual function is markedly decreased.
- Growth improves after thyroid replacement even in late diagnosed cases.
- In neonatal hypothyroidism, the goal is to bring the serum free T4 rapidly into the upper half of the range of normal.
- Suppression of TSH is not seen and not necessary in all cases because such suppression may lead to excessive doses of levothyroxine.
- However, the presence of normal serum thyroxine with inappropriately elevated TSH levels during treatment may suggest an inadequate thyroxine dose or nonadherence to treatment.
Associated Diseases
- Autoimmune polyglandular syndrome type I: consists of hypoparathyroidism, Addison disease, mucocutaneous candidiasis, and hypothyroidism.
- Autoimmune polyglandular syndrome type II: consists of Addison disease, type 1 diabetes mellitus, and, frequently, hypothyroidism.
- Trisomy 21 and Turner syndrome are predisposed to the development of autoimmune thyroiditis.
- Associated autoimmune diseases include celiac disease, type 1 diabetes mellitus, adrenal insufficiency, and hypoparathyroidism.
Key Points to Remember
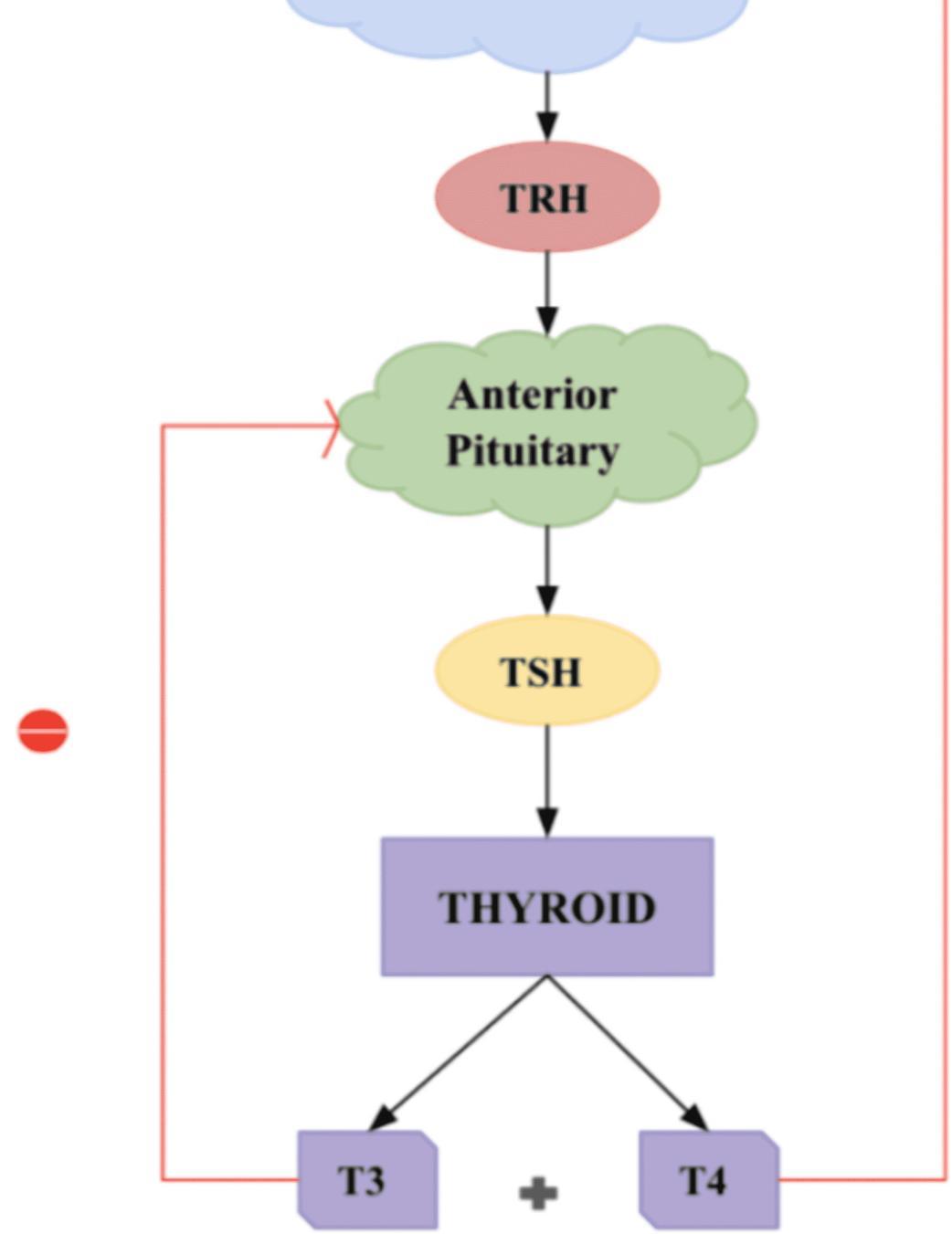
- The amount of TSH that the pituitary sends into the bloodstream depends on the amount of T4 that the pituitary sees. If the pituitary sees very little T4, then it produces more TSH to tell the thyroid gland to produce more T4. Once the T4 in the bloodstream goes above a certain level, the pituitary’s production of TSH is shut off.
- The “free” T4 or T3 is the hormone that is unbound and able to enter and affect the body tissues.