PEDIATRIC INFECTIVE ENDOCARDITIS
DR MANSOUR ALQURASHI
Infective Endocarditis (IE) Definition
- IE is an infection of the endocardium and/or heart valves that involves thrombus formation (vegetation), which may damage the endocardial tissue and/or valves.
- IE can involve native endocardium/endothelium or prosthetic material.
- Incidence: Rates of IE <5 per 100,000 individuals per year. Rates are higher among infants <1 year old compared with older children and adolescents.
Risk Factors Z
- Congenital heart disease (CHD):
- Complex cyanotic CHD, especially in those who have had surgical intervention.
- Central venous catheters (CVC):
- Critically ill and premature infants and children with cancer or connective tissue disorders.
- Artificial heart valves or prosthetic materials.
- Rheumatic heart disease:
- Severe valvular damage.
- Other risk factors:
- Injection drug use.
Microbiology
- Common pathogens:
- Fungi:
- Candida.
- Risk factors: Indwelling catheters and high glucose in parenteral nutrition (especially in preterm infants).
- Other pathogens:
- HACEK organisms: Small, fastidious gram-negative bacilli common in neonates and immunocompromised children.
- Enterococci, Brucella, Anaerobes.
- Coxiella burnetii (Q fever), Rickettsiae, typhus, Chlamydia.
Clinical Manifestations
Acute IE
- A rapidly progressive & fulminant disease, characterized by high fever and severe illness.
- Common in IE due to S. aureus or Streptococcus pneumoniae, which cause rapid destruction of heart valve, abscess formation, embolic phenomena, and shock.
- Fungal IE can present as an acute fulminant infection.
Subacute IE
- More common than acute IE.
- Characterized by a prolonged course of low-grade fever and nonspecific complaints including fatigue, arthralgias, myalgias, chills, night sweats, weight loss, and exercise intolerance.
- The presence of a cluster of these symptoms in a patient at risk for IE (i.e., CHD or indwelling CVC) should raise the possibility of IE as a potential diagnosis.
- Less virulent pathogens (e.g., viridans group streptococci, coagulase-negative staphylococci) typically have a subacute presentation.
- Risk of immunologic sequelae, such as immune-mediated glomerulonephritis.
Clinical Findings by Age Group
Neonates
- Presentation of IE may be indistinguishable from bacterial sepsis.
- Common manifestations: Feeding intolerance, tachycardia, respiratory distress, hypotension, and a new or changing murmur. Fever may be absent.
- Neonates with right-sided IE in association with CVC characteristically have little clinical evidence of disease other than persistently positive blood cultures in the setting of appropriate antibiotic treatment.
Older Infants and Children
- Septicemia signs: Fever, vasodilation, and tachycardia.
- Subacute symptoms: Malaise, headache, myalgias, and arthralgias.
- Signs of valvulitis:
- A new or changing murmur.
- Signs of acute heart failure (e.g., dyspnea, tachypnea, rales) or poor systemic perfusion due to perforation of a valve, chordal rupture, or poor ventricular function.
- Worsening cyanosis in children with underlying cyanotic CHD if IE involves either a systemic-pulmonary shunt or conduit. This is because the infection may obstruct blood flow across the shunt or conduit.
- Immune-mediated complications: Glomerulonephritis (subacute IE).
- Embolic complications:
- Septic emboli are common, resulting in extracardiac infection (e.g., osteomyelitis, pneumonia, lung abscess).
- Emboli can cause infarction to major vessels and organs:
- Brain: May result in seizures, headache, strokes.
- Other sites: Kidneys, lungs, GIT, and eyes.
- Splenomegaly: 25–60%.
- Relatively uncommon manifestations (highly suggestive of IE):
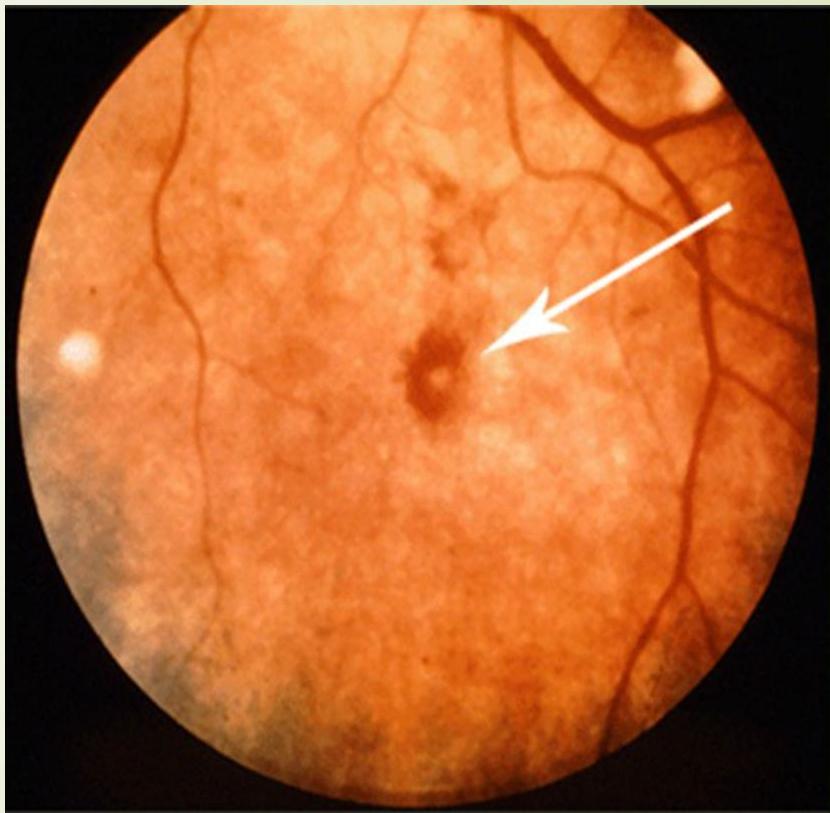
- Janeway lesions, Osler nodes, and Roth spots.
Specific Physical Signs
Janeway Lesions
Nontender hemorrhagic macules or papules located on palms, soles, and thenar and hypothenar eminences.

Osler Nodes
Tender, painful, purple-pink nodules 1 to 1.5 mm on the distal fingers and toes, hypothenar, and thenar muscle. Caused by deposition of immune complexes.

Conjunctival Petechiae


Splinter Hemorrhages
Small linear hemorrhages under the fingernails.

Roth Spots Retinal hemorrhages that have white/pale centers.
Investigations
Nonspecific Investigations
- Anemia: Hemolytic or anemia of chronic disease (common feature of IE).
- Leukocytosis.
- Thrombocytopenia: Unusual.
- Rheumatoid Factor: Positive in 50% (resolves after treatment).
- Inflammatory Markers: Elevated ESR, CRP, procalcitonin.
- Urinalysis:
- Hematuria, proteinuria, and RBC casts (suggestive of glomerulonephritis, a minor diagnostic criterion).
- Pyuria (metastatic infection).
- ECG: Prolongation of the PR interval or frank heart block can occur with periannular extension.
- Chest Radiograph:
- Nonspecific findings: Cardiomegaly, pulmonary edema, pleural effusions.
- Focal pulmonary infiltrates (in patients with pulmonary septic emboli).
- Peripheral nodular densities (metastatic lesions).
Specific Investigations
The diagnosis of IE is based upon history, physical examination, blood cultures, laboratory tests, and echocardiography.
Blood Cultures
- Cornerstone of microbiological diagnosis (95%).
- Procedure: Minimum of three blood cultures obtained over a time period of a few hours to two days, obtained from separate venipunctures.
- Critically Ill Children: Three separate venipunctures should be performed as quickly as possible (ideally within <30 minutes) and empiric antibiotic therapy started promptly.
- Considerations: Long incubation; check for HACEK organisms.
Serology/PCR
- PCR, IFA for detection of IgG and IgM antibodies.
Echocardiography
- Indication: An echocardiogram for all patients with suspected IE.
- Findings: Vegetations, myocardial abscess, valve competence.
- TTE (Transthoracic): Less sensitive for vegetations than TEE; used for adolescents or overweight children.
- TEE (Transesophageal): More sensitive.
- Other Imaging: Cardiac CT, FDG PET/CT and CMR imaging useful in select clinical situations.
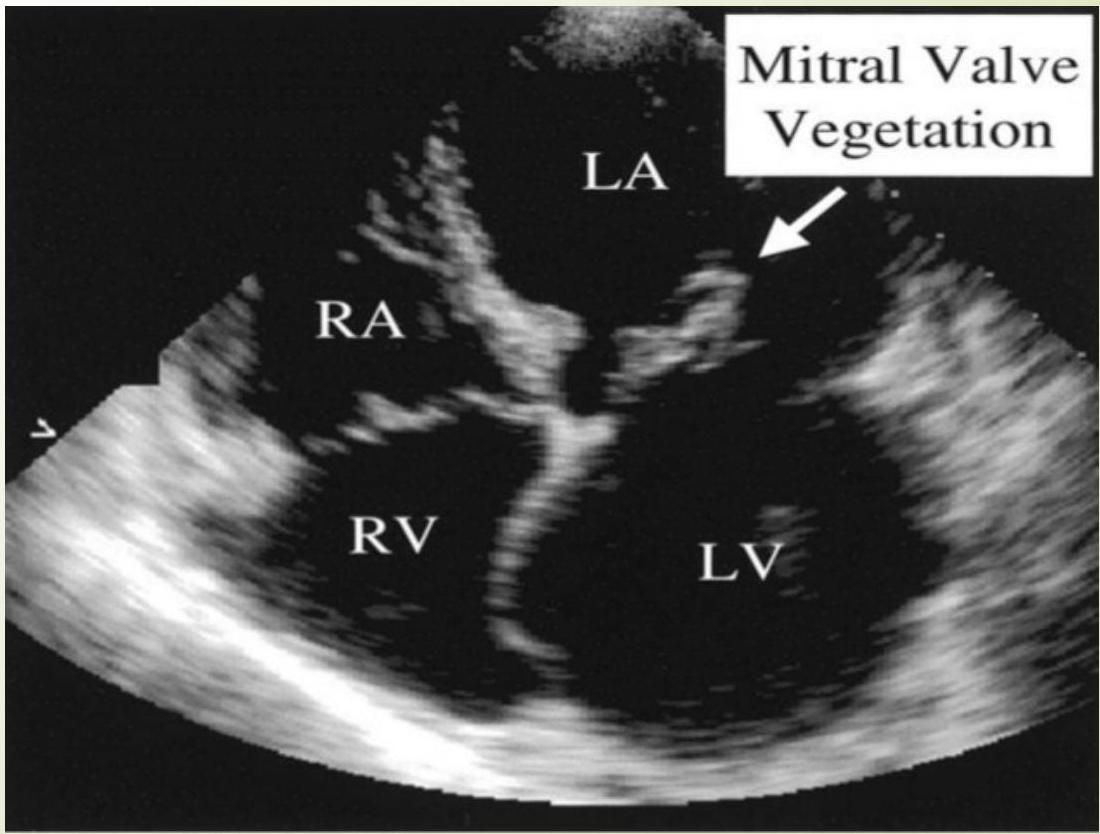
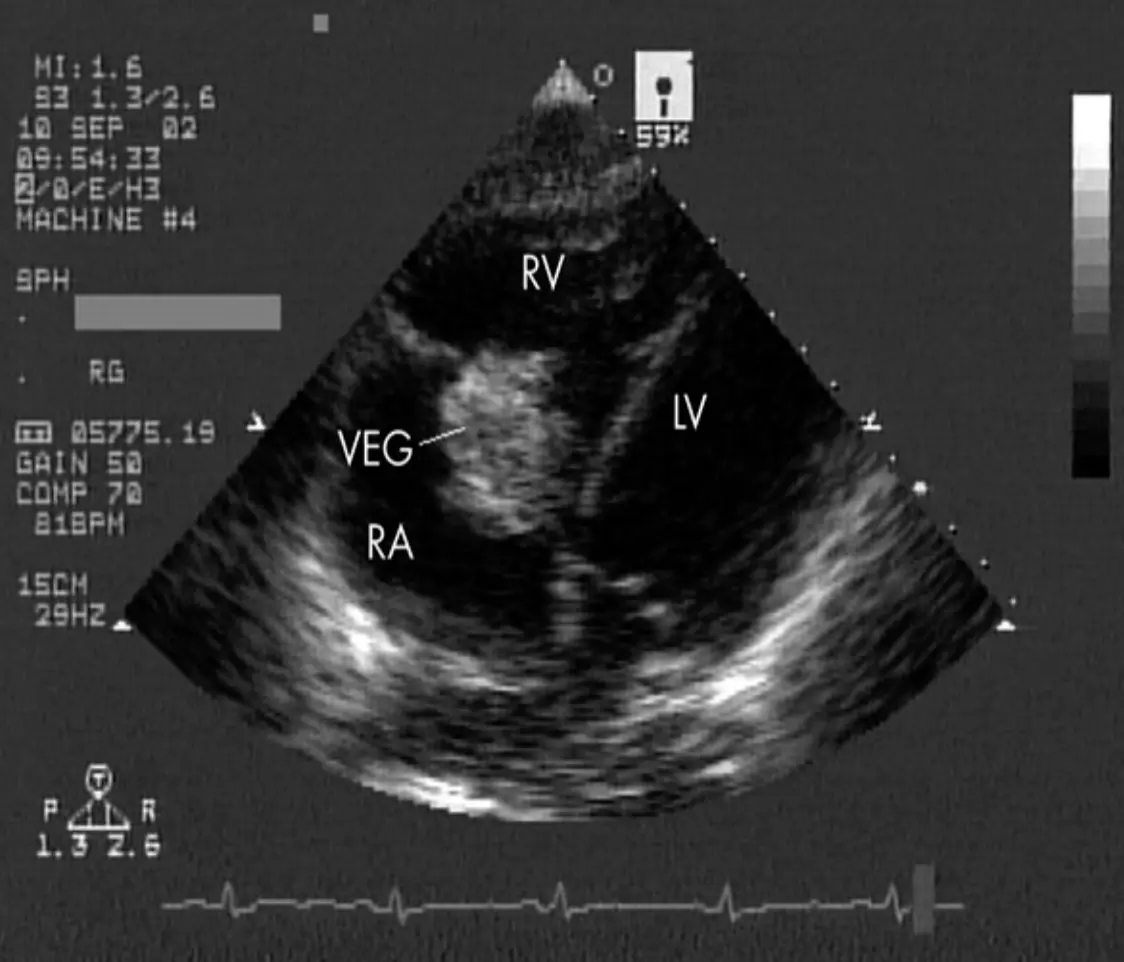
Echocardiography Images
Mitral Valve Vegetation
Diagnosis: Duke Criteria Z - SMLE
Major Criteria
- Positive blood culture: Z
- 2 positive cultures for a typical pathogen.
- OR 3 positive cultures for a non-typical pathogen.
- Evidence of endocardial involvement:
- Positive echocardiogram (vegetation or intra-cardiac abscess).
- Evidence of endocardial involvement during surgery.
Minor Criteria
- Fever.
- Presence of predisposing heart disease.
- Positive blood culture (but not for a typical pathogen and less than 3).
- Echo finding (but not meeting major criterion).
- New evidence of valve regurgitation (i.e., new coming murmur).
- Immune phenomena: Osler node, Roth spot, or glomerulonephritis.
- Vascular phenomena: Janeway lesion, arterial emboli, or intracranial hemorrhage.
Diagnostic Requirements
- 2 Major criteria.
- OR 1 Major criteria & 3 Minor criteria.
- OR 5 Minor criteria.
Treatment
- Goal: Complete eradication of the causing organism.
- Regimen: Prolonged, Parenteral, and Bactericidal antibiotic regimen guided by antibiotic sensitivity studies.
Empiric Therapy
- Indications: For patients with severe manifestations of acute IE, empiric treatment should be started as soon as diagnosis is suspected.
- Stable Patients: In children who are clinically stable, antibiotic therapy can be withheld for at least 48 hours until the results of blood cultures are available.
- Protocol: Empiric therapy should be administered after at least two (preferably three) sets of blood cultures have been obtained from separate venipunctures, ideally spaced over 30 to 60 minutes.
- Coverage: Staphylococci (methicillin-susceptible and methicillin-resistant), streptococci, enterococci, and gram-negative bacilli.
Regimens:
- Suspected Native Valve Endocarditis:
- Vancomycin and Ceftriaxone.
- Suspected Prosthetic Valve Endocarditis:
- Vancomycin (activity against enterococci and methicillin-resistant staphylococci).
- PLUS either Cefepime or Piperacillin-tazobactam (activity against aerobic gram-negative organisms including Pseudomonas).
Surgical Indications in Endocarditis
- Hemodynamically unstable: a. New or worsening heart failure. b. Valvular dysfunction.
- Uncontrolled infection: a. Remaining positive blood cultures. b. Fungal endocarditis. c. Perivalvular or myocardial abscess.
- Embolic manifestations.
Prognosis and Complications
Risk Factors for Complications:
- Prosthetic cardiac valves.
- Left-sided involvement.
- S. aureus or fungal IE.
- Previous IE.
- Prolonged symptoms (≥3 months).
- Cyanotic congenital heart disease.
- Systemic-to-pulmonary shunts.
- Poor clinical response to antimicrobial therapy.
Statistics:
- Complications occur in 50-60% of cases.
- Mortality at 8%.
Complications of IE
Cardiac Complications:
- Heart failure: Caused by perforation of the valve, rupture of an infected chordae, or perivalvar leaks or dehiscence in patients with prosthetic valve.
- Extension of infection beyond the endothelium:
- May cause perivalvular abscess (leading to an arrhythmia or atrioventricular heart block), myocardial abscesses, toxic myocarditis, acquired VSD.
- Obstruction: Extension of infection into a prosthetic shunt or conduits may occlude the graft. These infections require surgical intervention because they rarely respond to medical management.
- Acute myocardial infarction.
Metastatic Infection:
- Infection at other sites can occur from septic emboli resulting in osteomyelitis, pneumonia, or distal abscesses in the kidneys, spleen, brain, or soft tissues.
Neurological & Vascular Complications:
- Mycotic aneurysms: Can occur in any systemic artery and result from septic embolization or, occasionally, from contiguous spread of infection. This complication is an indication for surgery.
- Stroke: Occurs in 5 to 15 percent of pediatric IE cases, chiefly in the setting of left-sided IE.
- Other embolic events:
- Pulmonary embolism (typically occurs in the setting of right-sided IE).
- Ischemia of the extremities.
- Splenic infarction.
- Visual impairment (due to embolism or due to endophthalmitis as a result of bacteremic seeding).
Renal Complications:
- Acute kidney injury (AKI): Occurs in approximately 10 percent of pediatric patients with IE.
- Causes: Renal infarction, glomerulonephritis (immune-mediated secondary process), and drug-induced acute interstitial nephritis.
Prevention & Prophylaxis Z
High-Risk Cardiac Conditions Requiring Prophylaxis
(Conditions with the Highest Risk of Adverse Outcome From Endocarditis or Which Prophylaxis With Dental Procedures Is Reasonable)
- Prosthetic cardiac valve or prosthetic material used for cardiac valve repair.
- Previous infective endocarditis.
- Congenital heart disease (CHD):
- Unrepaired cyanotic CHD, including palliative shunts and conduits.
- Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 mo after the procedure (endothelialization).
- Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization).
- Cardiac transplantation recipients who develop cardiac valvulopathy.
Procedures Requiring Antimicrobial Endocarditis Prophylaxis
(In High-Risk Patients)
| Category | Procedures |
|---|---|
| Oral-dental* | • Dental extraction • Dental implant placement or reimplantation of avulsed teeth • Periodontal procedures, including surgery, scaling, root planing, and probing • Prophylactic cleaning of teeth or implants when bleeding is anticipated • Root canal instrumentation or surgery beyond the apex |
| Respiratory tract | • Bronchoscopy if mucosa is to be incised • Procedures done during an established infection • Tonsillectomy, adenoidectomy, or both |
| *For patients without active infection. |
Procedures NOT Requiring Prophylaxis
- TEE, esophagogastroduodenoscopy, colonoscopy, or cystoscopy, in the absence of active infection.
- GU or GI tract procedures do not require preprocedure antibiotics.
- Tattooing and body piercing.
- Implantable cardiovascular devices.
Recommended Prophylaxis Regimens
(During Oral-Dental or Respiratory Tract Procedures for patients without active infection)
| Route | Drug | Adult Dosage | Children Dosage |
|---|---|---|---|
| Oral (Given 1 h before procedure) | Amoxicillin | 2 g | 50 mg/kg |
| Allergic to Penicillin: | |||
| Clindamycin | 600 mg | 20 mg/kg | |
| OR Cephalexin / Cefadroxil | 2 g | 50 mg/kg | |
| OR Azithromycin / Clarithromycin | 500 mg | 15 mg/kg | |
| Parenteral (Given 30 min before procedure) | Ampicillin (IM or IV) | 2 g | 50 mg/kg |
| OR Cefazolin (IM or IV) | 1 g | 25 mg/kg | |
| Allergic to Penicillin: | |||
| Clindamycin (IV) | 600 mg | 20 mg/kg |
Adapted from Wilson W, Taubert KS, Gewitz M, et al: Prevention of infective endocarditis. Circulation 116(15):1736–1754, 2007.