Skin Rash Case Review
Dr. Faten Zaidan
Table of Contents
Case 1: Contact Dermatitis
Clinical Presentation
14-year-old girl develops severe itching and linear erythema and blisters of her arms and legs after hiking in the woods. She has a history of allergic rhinitis.
Questions
- What is your suspected diagnosis?
- How would you treat?
Diagnosis
Contact dermatitis (allergic dermatitis)
- May be due to contact with Ivy Plant (contains poison)
- Very painful condition
- Generally, if wheals or bullae are present, there is some sort of allergy
Treatment
- IU Steroids
- Antihistamines
- Wash off the poison

Case 2: Seborrheic Dermatitis
Clinical Presentation
15-year-old girl presents with redness and scaling of her eyebrows and alar crease. No itching is reported. She applies moisturizers without benefit.
Questions
- What is the most likely diagnosis?
- What is your first-line treatment?
Diagnosis
Seborrheic dermatitis
Treatment
- Corticosteroid combined with antifungal
- Selenium Sulfide Shampoo (to reduce scaling)

Case 3: Alopecia Areata
Clinical Presentation
15-year-old boy developed a single asymptomatic patch of alopecia. He was not concerned until multiple additional patches were noticed. His mother has not witnessed him pulling his hair.
Diagnosis
Alopecia areata
Treatment
- Mild potency steroids
Important Notes
- Alopecia universalis: All hair falls out
- Trichotillomania: Pulling of hair (behavioral cause)

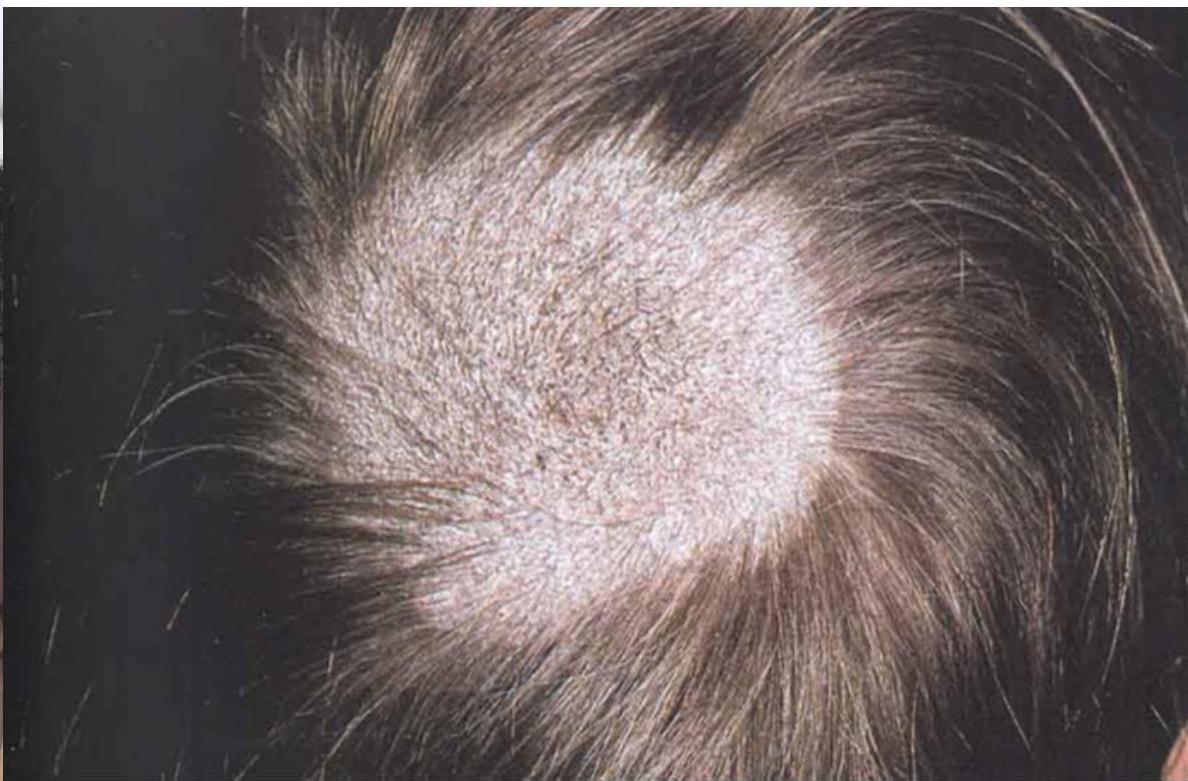
Case 4: Tinea Capitis
Clinical Presentation
Fungal infection with broken hair and presence of scales. Follicles are present.
Key Features
- Broken hair
- Presence of scales
- Follicles are present

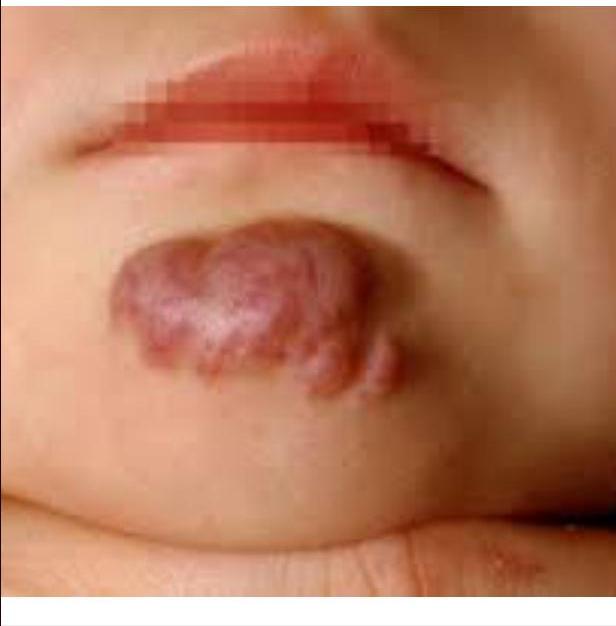
Case 5: Hemangioma
Clinical Presentation
2-month-old girl presents with vascular plaque on the chin that has been present since birth. Parents report that it has just started growing.
Diagnosis
Hemangioma
Management
- Reassurance: Expected to decrease in size or disappear within 1-2 years
When to Refer (Red Flags)
- Changes in color
- If ≥5 lesions present
- Bleeding
- Location on face or near eyes
- Location in beard area
- Concern for internal involvement
Treatment
- Propranolol (causes vasoconstriction) - important to do before surgical removal
Investigations
- If ≥5 hemangiomas: Do ultrasound of liver initially to look for hepatic hemangiomas
- If multiple hemangiomas in the body: Do MRI of the body (expect internal hemangiomas)
- Can cause obstruction or easily die (hemorrhagic shock due to internal hemangioma)
- Risk of bleeding: If it bleeds, it won’t stop
- Urgent ENT referral for ethanol injection should be done
- Requires coordination: constant monitoring, anesthesia, back-up OR, ICU - takes time

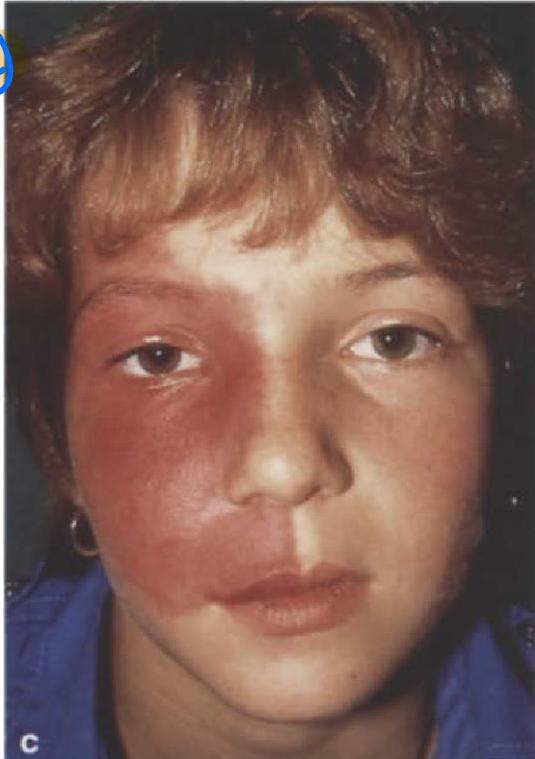
Case 6: Port Wine Stain
Clinical Presentation
5-year-old girl presents with dusky purple patch involving the right forehead, upper and lower eyelids, and cheek in trigeminal V1 distribution.
Diagnosis
Port wine stain (Sturge-Weber syndrome)
Next Steps in Evaluation
- Brain CT for intracranial calcification
- Refer to ophthalmology to check for glaucoma, brain, palsies
Case 7: Mongolian Spots
Clinical Presentation
1-month-old baby presented with gray patch on lower back extending to buttocks.
Diagnosis
Mongolian spots (Congenital dermal melanocytosis)
Differential:
- neurofibromatosis
- abuse
- itp

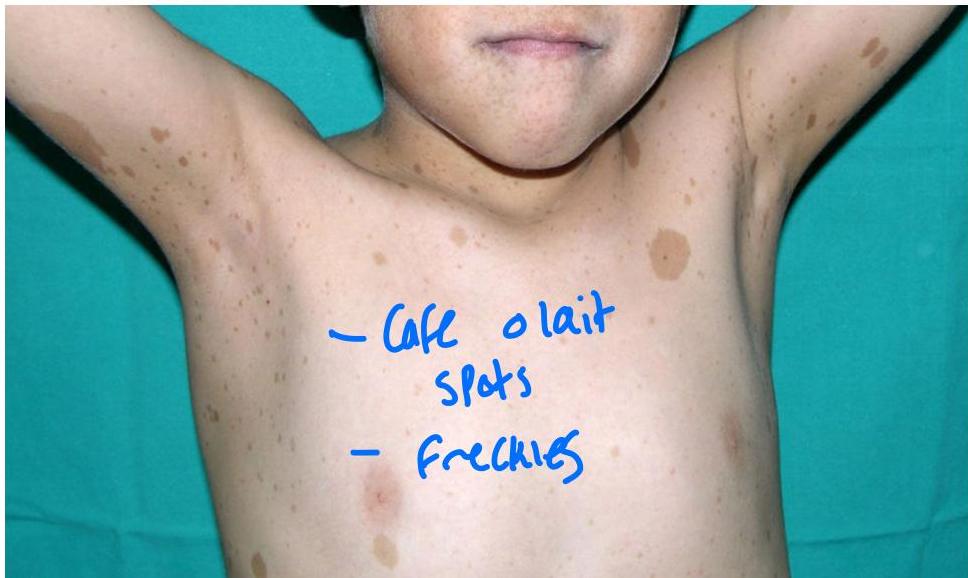
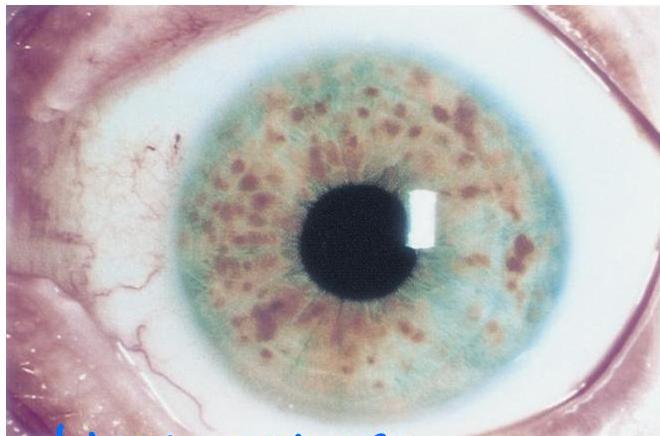
Case 8: Neurofibromatosis Type 1
Clinical Presentation
5-year-old girl presented with five café au lait macules on the trunk, ranging from 5 to 9 mm in diameter. Axillary freckling also noted.
Diagnosis
Neurofibromatosis Type 1
Associated Findings
- Lisch nodules (iris hamartomas)

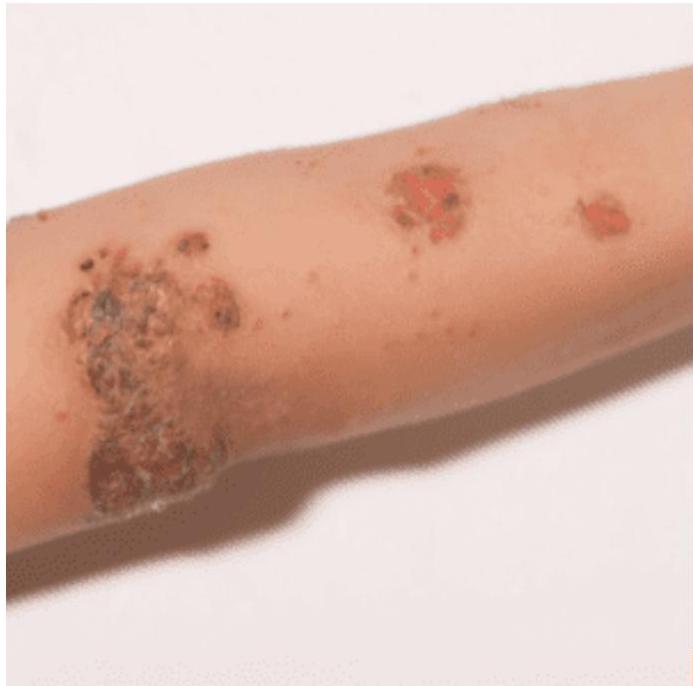
Case 9: Impetigo
Clinical Presentation
15-year-old boy presents with crusting on the arm after falling off his skateboard 2 weeks earlier. The erosion has not yet healed.
Diagnosis
Impetigo
Management
- Mupirocin + fucidic acid
Case 10: Erythema Multiforme
Background: Hypersensitivity Reactions
Three hypersensitivity reactions that occur after medication, viral, or bacterial infection (e.g., Mycoplasma infection):
- SJS (Stevens-Johnson syndrome)
- TEN (Toxic Epidermal Necrolysis)
- EM (Erythema Multiforme) - not fatal, targetoid lesions
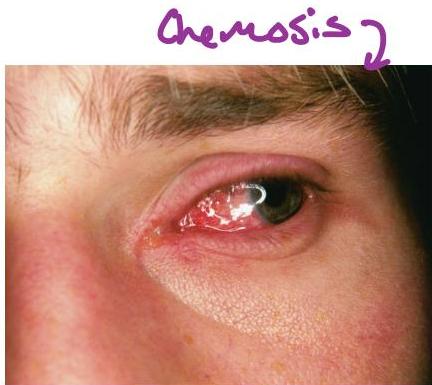
Features:
- Mucosal lesions
- Chemosis
- Positive Nikolsky sign
- Involves ≥2 regions in the body
Clinical Presentation
15-year-old boy presented with erythematous targetoid lesions of the arms. No active mucosal lesions. History of herpes labialis 10 days prior to onset.
Diagnosis
Erythema multiforme
- Benign condition
Treatment
- Supportive treatment
- Steroids
- Antihistamines
- Saline infusion

Case 11: SJS/TEN
Clinical Presentation
12-year-old boy with epilepsy develops acute onset malaise, fever, and painful skin 2 weeks after starting an anticonvulsant. The eruption starts on his trunk and then spreads to the entire body, resulting in widespread skin sloughing. Patient requires hospital admission.
Diagnosis
SJS (Stevens-Johnson syndrome) or TEN (Toxic Epidermal Necrolysis)
- Fatal condition
- Requires immediate admission
Treatment
- IVIg
- Steroids
- Antihistamines

Case 12: Scabies
Clinical Presentation
12-year-old girl returns home from summer camp noting severe itching, which is most pronounced at night. Papules and linear tracks are concentrated on her wrists and the web spaces of her hand.
Diagnosis
Scabies
Confirmation
- History and physical exam
- Direct microscopy
Presentation
- Itchy, especially at night
- Tunnels/burrows
Characteristic Locations
- In between fingers
- Axillae
- Genital area
Treatment
- Permethrin
- Given to all household members


Case 13: Measles
Clinical Presentation
3-year-old boy presented to ER with fever of 38°C for two days. Associated with maculopapular rash, cough, and sore throat. Rash started from head to toe. Usually starts behind the ears. He had contact with his cousin who had similar presentation two weeks ago.
Upon examination: erythematous throat, bilateral conjunctivitis, maculopapular rash all over trunk and extremities.
Diagnosis
Measles
Key Points
- Vitamin A decreases severity of clinical presentation
- Should isolate the patient
- First sign: Koplik spots (white spots in oral mucosa)

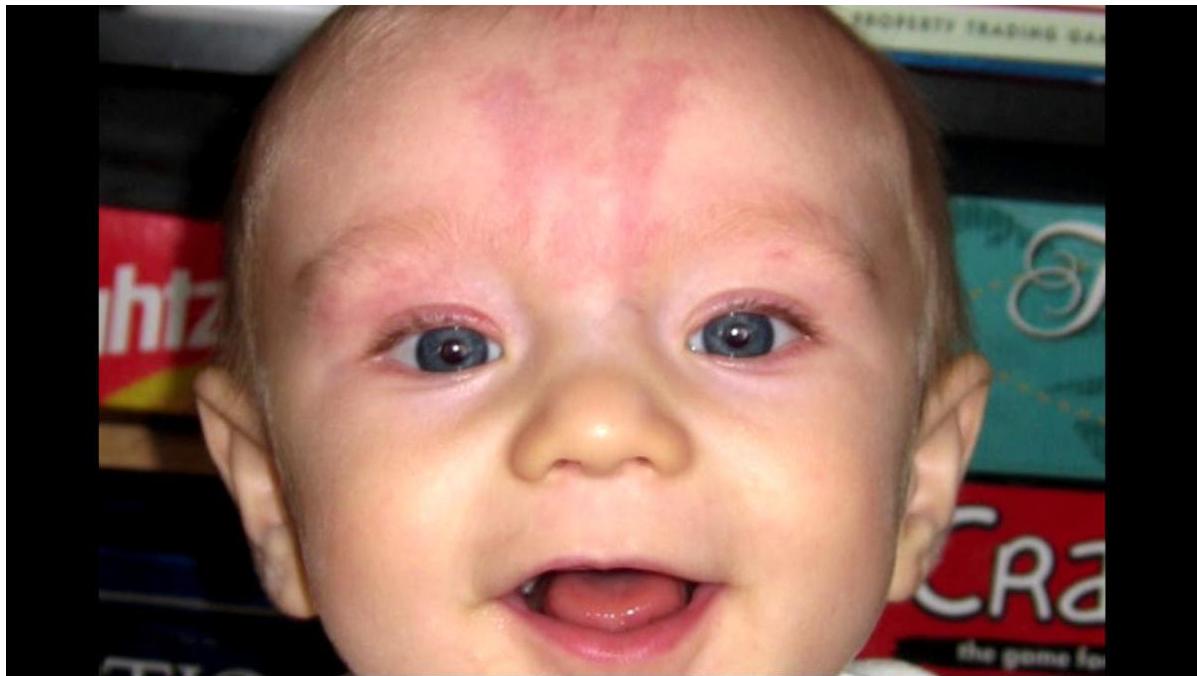
Case 14: Nevus Simplex
Clinical Presentation
Two-month-old girl presented with pinkish macule on the forehead located between eyes. Appeared since birth, darkens with intense crying.
Diagnosis
Nevus simplex
Management
- Reassure mother (benign, usually fades with time)
Case 15: Impetigo
Clinical Presentation
Punched out pustules with high-grade fever. Quickly spreading among school children.
Characteristics
- Common in children
- Highly contagious
- Punched out lesions (raised, reddish, depressed center)
Diagnosis
Impetigo (or possibly Molluscum contagiosum)
Treatment
ablation - usually self resolving
- Neosporin
Case 16: HSP
Clinical Presentation


Diagnosis
HSP (Henoch-Schönlein Purpura)
Features Patient May Present With
- Abdominal pain → Suspect intussusception
- Joint pain
- Microscopic hematuria
Differential Diagnosis
- Meningococcemia
Case 17: Fifth Disease
Clinical Presentation
4-year-old boy presented with papular erythematous rash on trunk. Four days before, same rash appeared on the cheeks. Associated with high-grade fever, sore throat, and runny nose.
Diagnosis
Fifth disease (Parvovirus B-19)
- Also causes bone marrow depression → aplastic anemia
Management
- Supportive


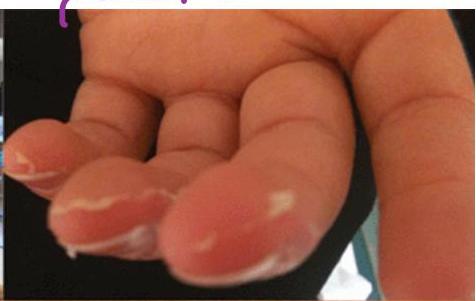
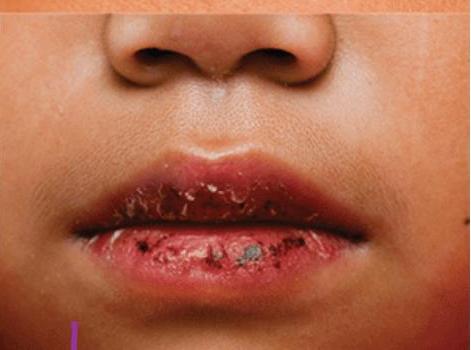
Case 18: Kawasaki Disease
Spot Diagnosis
Differential Diagnosis: Scarlet Fever
Diagnosis
Kawasaki Disease
Diagnostic Criteria
- Fever of ≥5 days
- Non-purulent conjunctivitis
- Cracked lips (mucous membrane involvement)
- Lymphadenopathy
- Rash
- Desquamation of fingers → occurs in last days of fever
Treatment
- IVIg and aspirin
- Regular follow-up by echo
- To decrease risk of aneurysm




diff
- scarlet disease
Case 19: Shingles
Clinical Presentation
Five-month-old term male infant came with vesicular rash. Mother first noticed several clusters of vesicles on the baby’s chest five days before presentation. In the subsequent four days, new adjacent vesicles erupted on the chest with clear discharge. Physical examination revealed a thriving, afebrile and well-appearing infant. Multiple crops of vesicles on an erythematous base were present on both the anterior and posterior right hemithorax.
Diagnosis
Shingles (Herpes Zoster)
Treatment
- Acyclovir


Case 20: Candidiasis
Clinical Presentation
Candidiasis (diaper dermatitis)
Key Features
- Satellite lesions
- In skin folds
Treatment
- Antifungal (e.g., Elica M - not given for more than 3-4 days)
- Combines antifungal + steroid
- Parent counseling

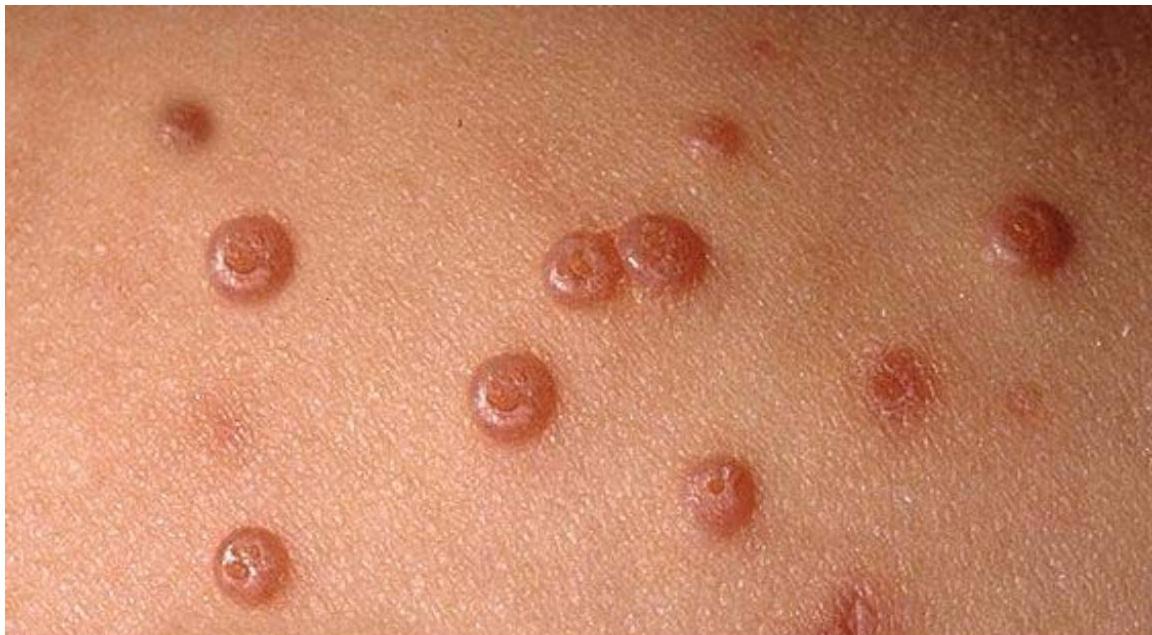
Case 21: Hand-Foot-Mouth Disease
Clinical Presentation
3-year-old boy presented to ER with 40°C body temperature not responding to paracetamol. On examination: maculopapular and vesicular rash on the medial side of the palms and soles. Similar lesions on the lips.
Diagnosis
Hand-foot-mouth disease
Features
- High-grade fever
- Irritable, sick-looking
- May have lesions around mouth
Management
- Supportive management




mouth pain - lead decreased water food intake ± dehydration.