Internal Medicine
TREATMENT
Aim of BP : < 120/80
- First, a trial of diet & exercise for about 2 months ( depending on the BP)
- low salt diet * wt. reduction * exercise
- eat more fruits & vegetables * stop smoking
- Add medicine if the above fails.
- Start with 1 medicine and gradually go to the max dose
- Give at least 2-3 wks for a medicine to work fully. Then add another medicine if needed.
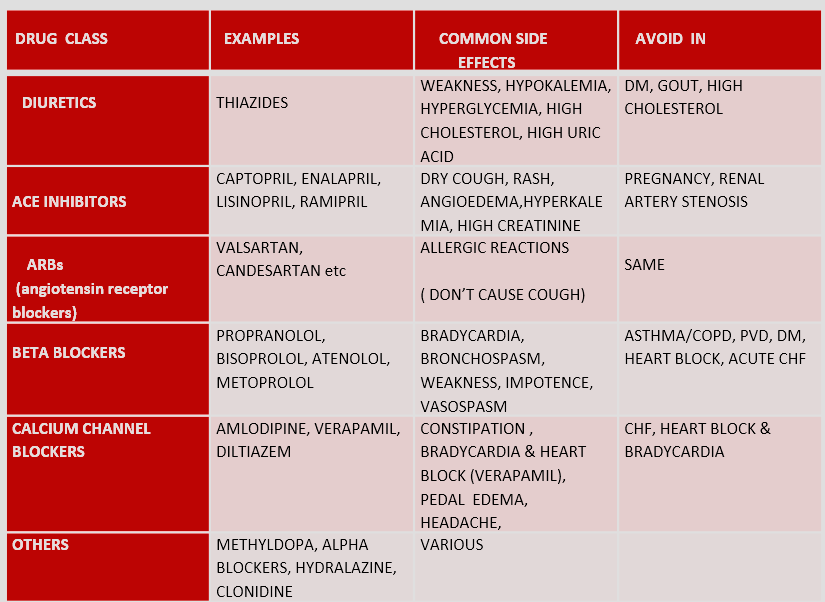
DRUG CLASS FOR HTN & COMMON SIDE EFFECTS/AVOID IN
EXAMPLES COMMON SIDE EFFECTS AVOID IN **** DIURETICS - THIAZIDES
- WEAKNESS, HYPOKALEMIA, HYPERGLYCEMIA, HIGH CHOLESTEROL, HIGH URIC ACID
- DM, GOUT, HIGH CHOLESTEROL ACE INHIBITORS CAPTOPRIL, ENALAPRIL, LISINOPRIL, RAMIPRIL
- DRY COUGH, RASH, ANGIOEDEMA,HYPERKALEMIA, HIGH CREATININE
- PREGNANCY, RENAL ARTERY STENOSIS ARBs (angiotensin receptor blockers) VALSARTAN, CANDESARTAN etc
- ALLERGIC REACTIONS (DON’T CAUSE COUGH) BETA BLOCKERS Z PROPRANOLOL, BISOPROLOL, ATENOLOL, METOPROLOL
- BRADYCARDIA, BRONCHOSPASM, WEAKNESS, IMPOTENCE, VASOSPASM
- ASTHMA/COPD, PVD, DM, HEART BLOCK, ACUTE CHF
- Avoid beta blockers in asthma/COPD, heart severe bradycardia/heart blocks
- Avoid beta blockers in DM ( they mask the S/S of hypoglycemia). Not an absolute contraindication.
- Never stop beta blockers suddenly. Always taper.
CALCIUM CHANNEL BLOCKERS AMLODIPINE, VERAPAMIL, DILTIAZEM
- CONSTIPATION , BRADYCARDIA & HEART BLOCK (VERAPAMIL), PEDAL EDEMA, HEADACHE,
- CHF, HEART BLOCK & BRADYCARDIA
OTHERS METHYLDOPA, ALPHA BLOCKERS, HYDRALAZINE, CLONIDINE
- VARIOUS
GUIDELINES TO START Rx.
Suggested by National Institute of Clinical Excellence , U.K. ( NICE guidelines)
- Age < 55 or white race : ACE or ARB
- Age > 55, black race : Calcium channel blocker or diuretic
These are just “guidelines”, & they are different in different countries
SPECIAL SITUATIONS
- HTN w/ DM: First choice ACE or ARB
- HTN w/ IHD: First choice is beta blocker , ACEI
- HTN w/ pregnancy: Methyldopa(aldomet), hydralazine, labetolol ( all safe) ACEI AND ARBs ABSOLUTELY “NO ” IN PREG.& Bilateral renal artery stenosis
- Patient w/ high sympathetic activity (tachycardia, anxious looking, hyperthyroid ⇒ beta blocker is better
Therapeutic
TREATMENT - Aim of BP: < 120/80
Rx contd.
- First, a trial of diet & exercise for about 2 months ( depending on the BP)
- low salt diet * wt. reduction * exercise
- eat more fruits & vegetables * stop smoking
- Add medicine if the above fails.
- Start with 1 medicine and gradually go to the max dose
- Give at least 2-3 wks for a medicine to work fully. Then add another medicine if needed.
DRUGS FOR HTN
- Diuretics
- ACE inhibitors
- ARBs (angiotensin receptor blockers)
- Beta blockers
- Ca. channel blockers
- Others
GUIDELINES TO START Rx.
Suggested by National Institute of Clinical Excellence , U.K. ( NICE guidelines)
- Age < 55 or white race : ACE or ARB
- Age > 55, black race : Calcium channel blocker or diuretic
These are just “guidelines”, & they are different in different countries
SPECIAL SITUATIONS
- HTN w/ DM: First choice ACE or ARB
- HTN w/ IHD: First choice is beta blocker , ACEI
- HTN w/ pregnancy: Methyldopa(aldomet), hydralazine, labetolol ( all safe) ACEI AND ARBs ABSOLUTELY “NO ” IN PREG.& Bilateral renal artery stenosis
- Patient w/ high sympathetic activity (tachycardia, anxious looking, hyperthyroid ⇒ beta blocker is better
SOME IMPORTANT POINTS
-
Avoid beta blockers in asthma/COPD, heart severe bradycardia/heart blocks
-
Avoid beta blockers in DM ( they mask the S/S of hypoglycemia). Not an absolute contraindication.
-
Never stop beta blockers suddenly. Always taper.