Pediatrics-2
Epidemiology and Types
- Life-threatening emergency.
- 80% of pediatric FBA episodes occur in children < 3 years of age.
- Peak incidence: 1-2 years.
- Commonly aspirated objects: Peanuts, seeds, popcorn, food particles, hardware, pieces of toys, coins, paper clips, pins, pen caps.
Location of FBA
- Bronchial (most common)
- Laryngo-tracheal (high mortality)
- Tracheal
- Lung
Note: Most foreign bodies are located in the right main bronchus due to its wider diameter and more direct extension of the trachea.

Clinical Presentation of FBA
The presentation depends on the age of the child, type of object, degree of blockage, and location.
- History of choking: Sudden onset of cough ± dyspnea ± cyanosis. (Sensitivity 75%, specificity 90%)
- Timing: 50-75% of cases present and are diagnosed within 24 hours of aspiration.
- Symptoms: Often present with coughing, wheezing, and/or decreased lung sounds that suggest an aspiration. High index of suspicion is critical.
Location-Specific Findings:
- Laryngotracheal: Acute respiratory distress, stridor, hoarseness, or complete airway obstruction.
- Tracheal: Stridor, wheeze, and dyspnea.
- Bronchial: Coughing, wheezing, hemoptysis, dyspnea, respiratory distress, decreased breath sounds, fever, and cyanosis.
- Delayed Diagnosis (days or weeks): Symptoms due to complications like pulmonary abscesses and bronchiectasis.
Diagnosis
- Inspiratory and Lateral Chest X-ray:
- A normal chest radiograph does not rule out FBA.
- 10% of FBs are radiopaque.
- Most are radiolucent (e.g., nuts, food particles).
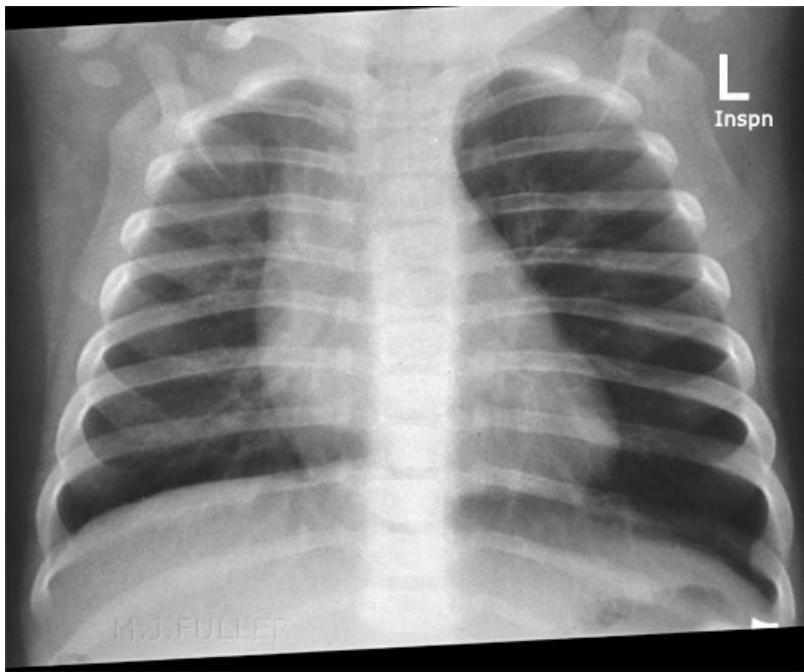
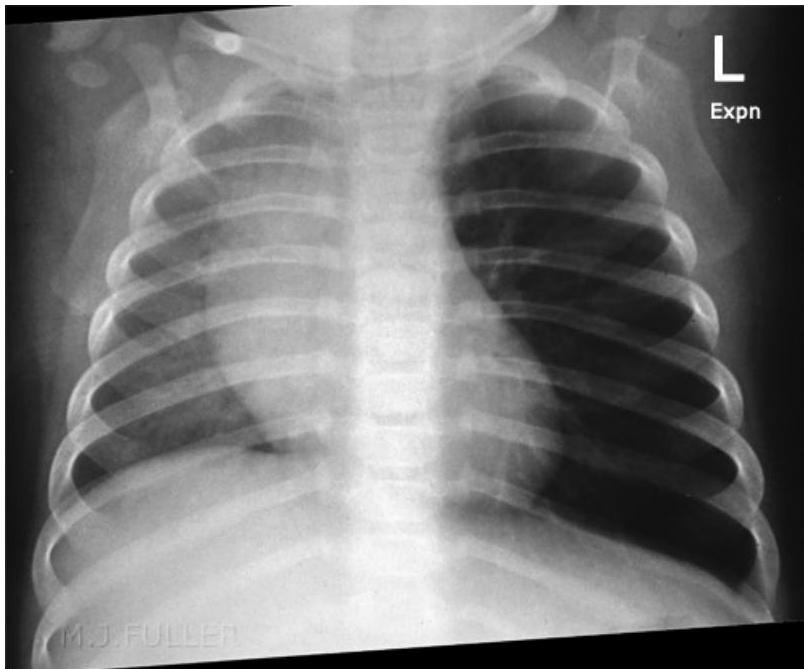
- Expiratory Chest X-ray or Fluoroscopy:
- Indicated for children with a suggestive presentation but normal inspiratory X-ray.
Radiological Findings:
- On Inspiration: Lungs may appear similar as airways widen, allowing air past the FB.
- On Expiration: The FB can obstruct the bronchus as its diameter decreases. The greatest difference in lung aeration is seen here, as air is trapped in the affected lung while exhaled from the normal lung.
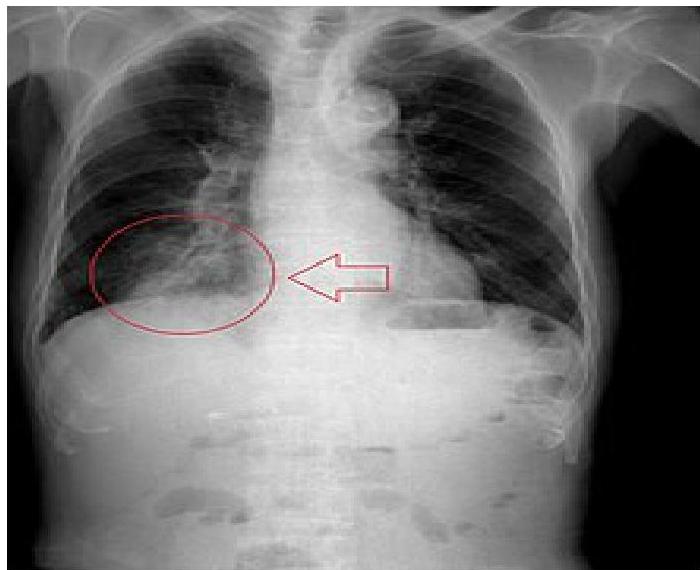
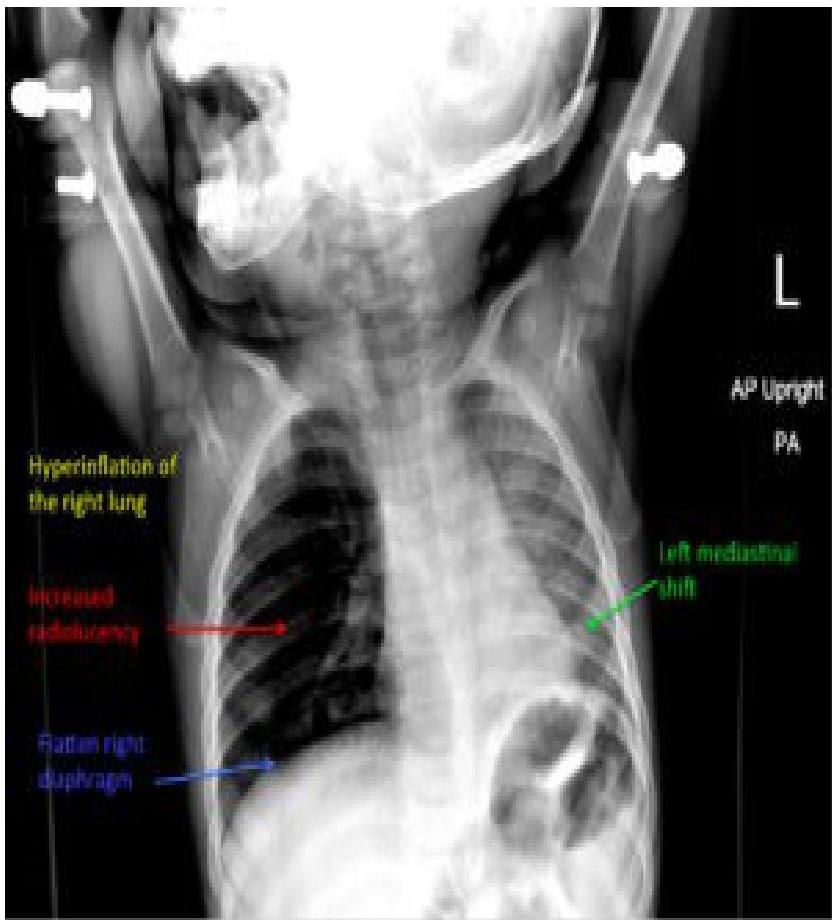
- Bronchial FBA Findings in chest x-ray:
- Hyperinflated lung
- Atelectasis
- Mediastinal shift
- Pneumonia
- Pulmonary abscesses and bronchiectasis (late signs)
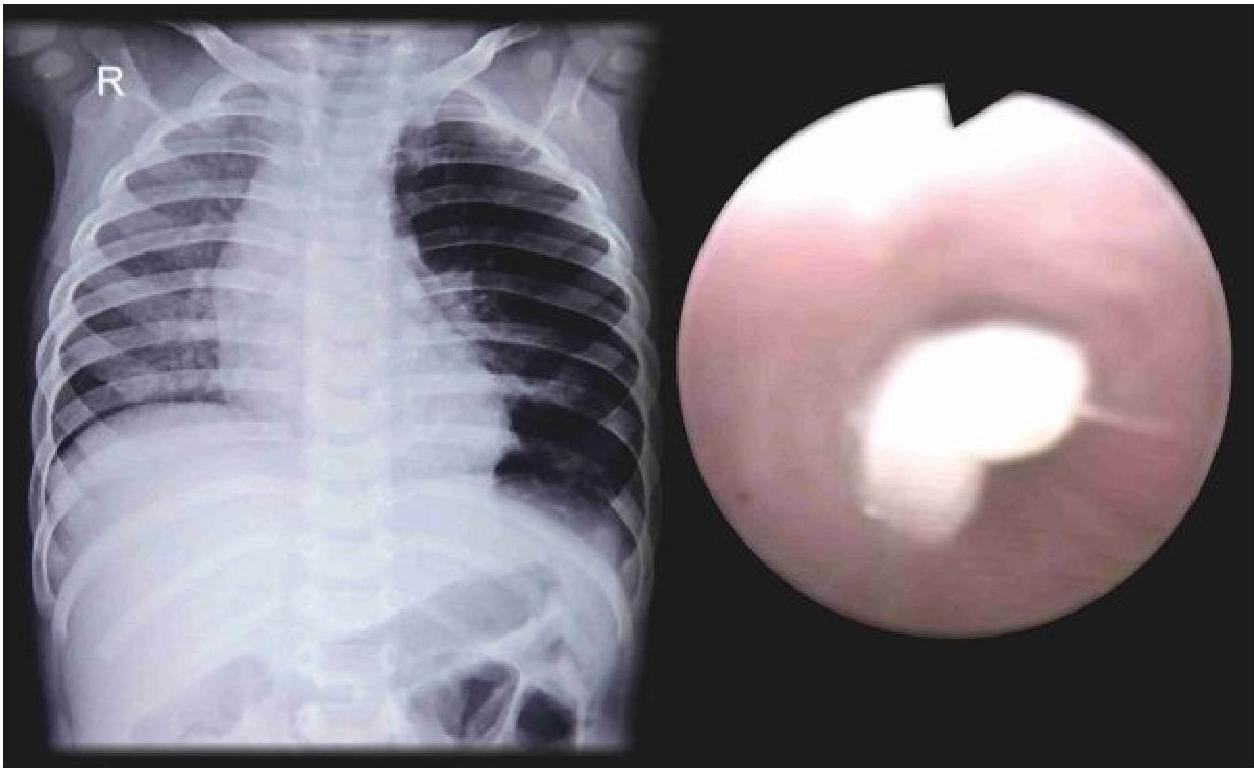
Left: Focal pneumonia in lower right lung lobe due to aspiration and airway obstruction. Right: Coin in the esophagus.
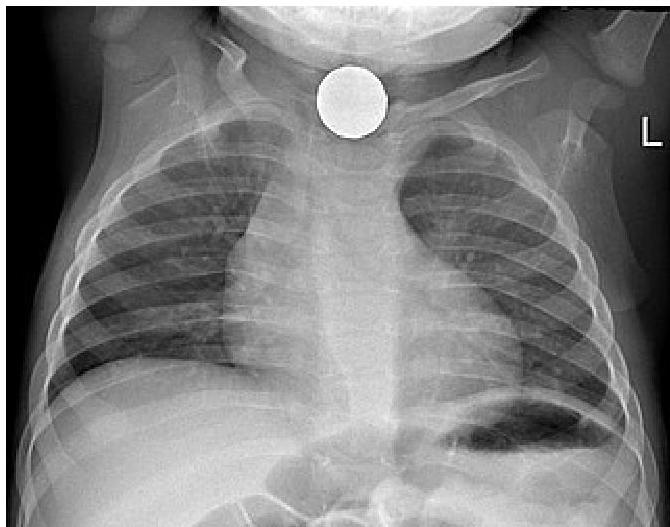
Foreign body aspiration of a coin in the esophagus
Management of FBA
Basic Management (Initial Steps)
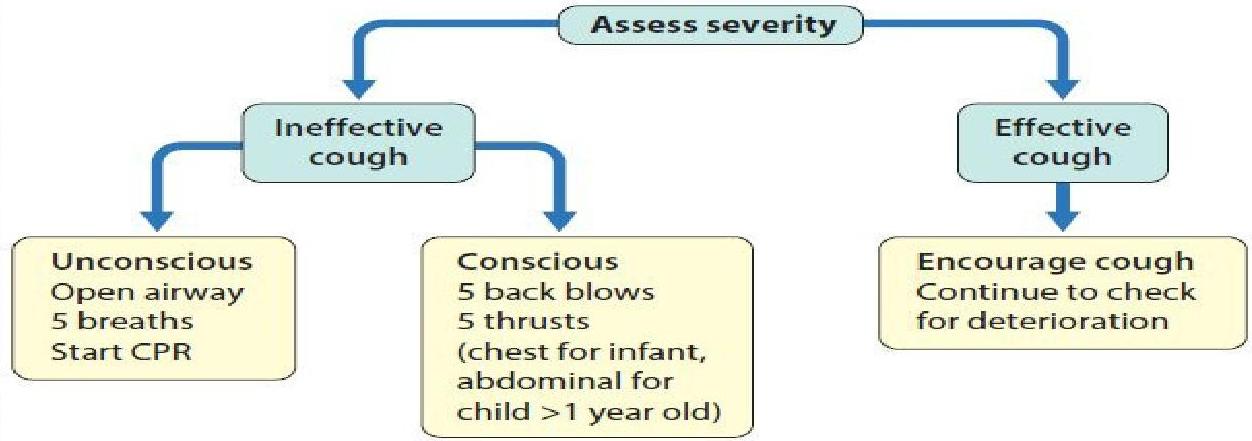
- Partial vs. Complete Obstruction:
- An airway obstruction can be partial or complete.
- In partial obstruction, the patient can usually clear the foreign body with coughing.
- In complete obstruction, acute intervention is required to remove the foreign body.
- Caution: Finger sweeping in the mouth is NOT recommended due to the increased risk of displacing the foreign object further into the airway.
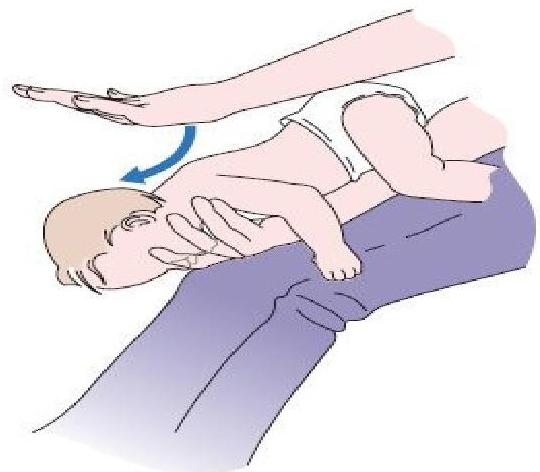
- Choking Infants (< 1 year):
- The child should be placed face down over the rescuer’s arm.
- Deliver 5 back blows with the heel of the hand.
- Turn the patient face-up and deliver 5 chest thrusts.
- The rescuer should alternate five back blows followed by five chest thrusts until the object is cleared.
- Choking Children (> 1 year):
- Use the Heimlich maneuver (abdominal thrusts) to dislodge a foreign body.
- If the patient becomes unresponsive during physical intervention, CPR should be started.

Note: Abdominal thrusts are repeated several times. The child can be standing, kneeling, sitting, or supine. Abdominal thrusts are best avoided in infants as they may cause intra-abdominal injury.
Advanced Management
- Persistence of Obstruction: In the event that basic measures do not remove the foreign body and adequate ventilation cannot be restored, treatment by trained personnel becomes necessary.
- Laryngoscopy: Should be performed in unresponsive patients if non-invasive airway clearance techniques are unsuccessful. If the foreign body can be seen, it can be removed with forceps.
- Endotracheal Intubation: An endotracheal tube should be placed to prevent airway compromise from resulting inflammation after the procedure.
- Emergency Airway: If the foreign body cannot be visualized, intubation, needle cricothyrotomy, or tracheostomy can be done to restore an airway for patients who have become unresponsive.
- Rigid Bronchoscopy: If non-invasive measures do not dislodge the object and the patient can maintain adequate ventilation, rigid bronchoscopy under General Anesthesia (GA) should be performed. Apply oxygen, cardiac monitoring, and pulse oximetry. Efforts should be made to keep the patient calm and avoid agitation.
- Flexible Bronchoscopy: Might be used when the diagnosis or object location are unclear.
- Post-Removal Care:
- Nebulized beta-adrenergic medication.
- Chest physiotherapy.
- Steroids and Antibiotics: Indicated when the FB is difficult to extract, when there is a documented respiratory tract infection, or when swelling within the airway occurs after removal of the object.
Case Study: FBA
Presentation: A 10-month-old male presented after choking on a carrot. Mom reported coughing with perioral cyanosis. Exam: No retractions, but wheezing heard in the right lung fields, particularly when coughing.
ENT
- Prevalence: Common accident in children, significant cause of morbidity and mortality. (infants and preschool)
- Statistics: 500 children die of FBA each year in the USA; 40% of lethal accidents among children under 1 year of age are caused by FBA.
Clinical Presentations
Acute Episode
- Period of choking, gagging, wheezing, hoarseness
Asymptomatic (Missed Diagnosis?)
- Cough, wheezing
Complications
- Pneumonia, obstructive emphysema, bronchiectasis
Diagnosis
- Medical history is key.
- Physical examination findings are abnormal in 80% of children with FBA and in 40% of children without FBs.
- Sensitivity and specificity of physical examination: 80.4% and 59%, respectively.
Radiological Examination
- Many FBs are not radiopaque, and small FBs may cause symptoms but not radiographic changes.
- Plain Film: Air trapping, obstructive emphysema, mediastinal shift
- Rt and Lt Lateral Decubitus Film

Common Aspirated Objects
- Food products (peanuts, seeds)
- Beans and seeds absorb water over time
- Inert FB (pieces of toys) cause less reaction

Negative Imaging Studies
- Do not exclude the presence of an FB.
- A high degree of clinical suspicion is crucial.
Removal
- Airway foreign bodies are removed most safely under general anesthesia using the ventilating rigid bronchoscope.






