Treat as early as possible – why we should operate earliest, to avoid amblyopia
Eye lid
Case Presentation
A 7 month-old male patient was referred to pediatric ophthalmologist for evaluation of left upper eyelid. The mother stated that the eyelid had been “droopy” since birth and that it appeared to be getting progressively worse. She denied any alteration of eyelid position with feeding. He had been followed closely by his pediatric ophthalmologist and had previously shown no signs of amblyopia of the left eye.
The patient was born full term after an uncomplicated pregnancy and delivery. There was no history of birth trauma. Visual Acuity (without correction): Fixes and follows OD, Fixes and follows OS. He had demonstrated a fixation preference for the right eye. Pupils: No anisocoria and no relative afferent papillary defect.


1- What is diagnosis?
Left simple congenital ptosis
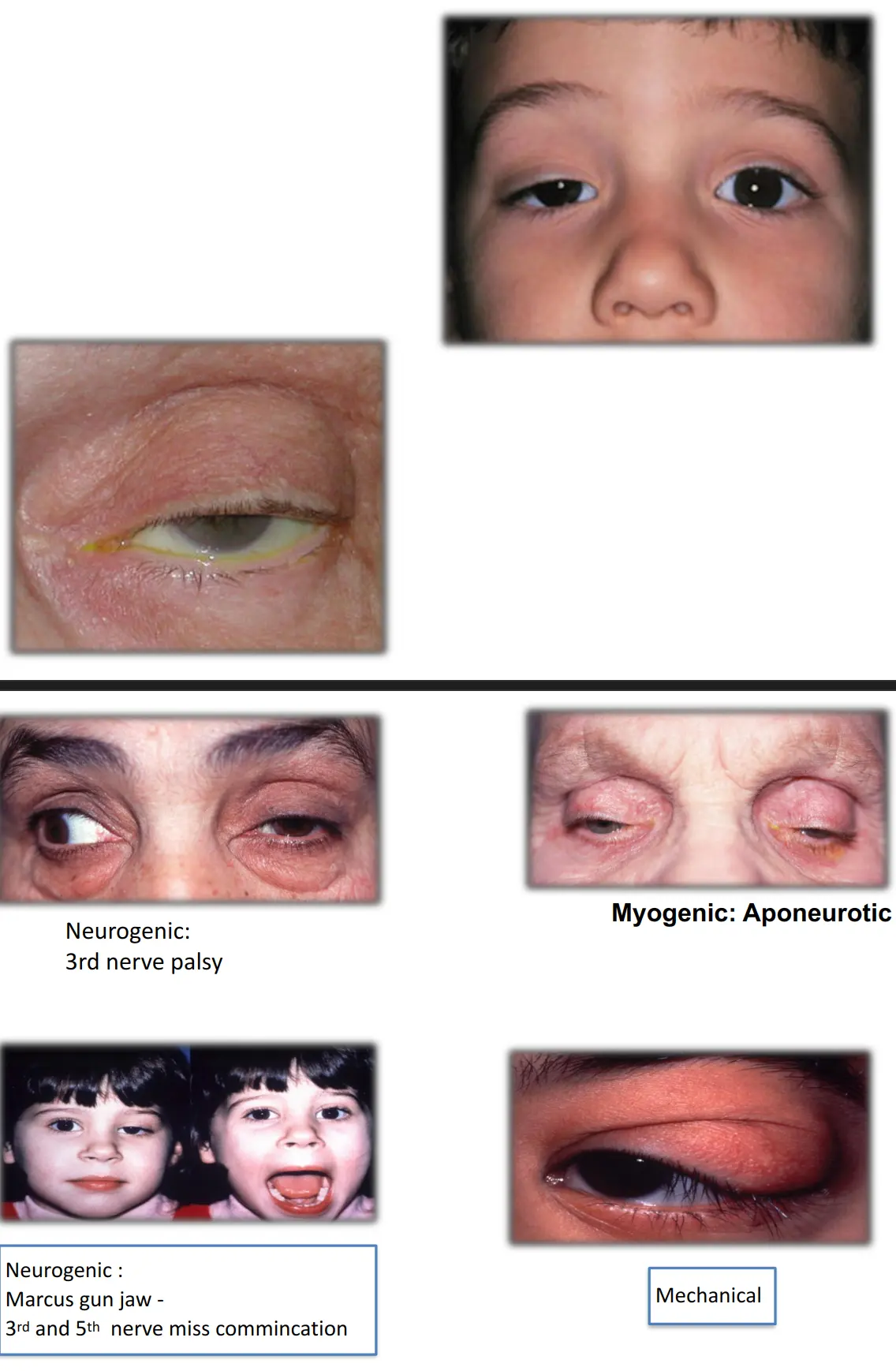
2- Differential diagnosis
In Pediatrics:
- Traumatic ptosis
- Neurogenic ptosis: Horner syndrome and 3rd n palsy.
- Myogenic ptosis: Ocular myopathy and Myasthenia gravis
- Mechanical ptosis
- Pseudoptosis.
In adult:
- Multiple sclerosis
- Blepharochalasis
- Involutional (snile) changes
- Prolapsed orbital fat
- Dermatochalasis
3- Clinical Examination & Investigations
Clinical Exam
- VA
- Ocular motility –
- pupil reflex –
- degree of ptosis – eg marginal reflex distance, which is the distance between the center of the pupil and the edge of the upper lid
- function of levator muscle -
- Measure the vision for amblyopia -
- Bells phenomena -
- Marcus gunn phenomena -
- Corneal sensitivity (by touch)
Investigations none
4- Treatments
- Observation in mild ptosis: in mild cases
- if severe Surgical correction as early as possible in severe cases
- Sling operation
If the case was: child with sever ptosis (cover pupil) OR (chin eleva(on: “Bilateral ptosis”) >>>> surgery!