ASTHMA
DR FAROOQ SATTAR DHEDHI
https://next.amboss.com/us/article/Ph0WVf?q=asthma
https://next.amboss.com/us/article/or00Rh?q=asthma+exacerbation#Zea3b743c51e3ea853ae437ae16e84d69
DEFINITION
- characterized by inflammation of the airways, causing intermittent airflow obstruction and bronchial hyperresponsiveness
SYMPTOMS
- Coughing
- Wheezing
- Shortness of breath
Symptoms can be frequently exacerbated by triggers ranging from allergens to viral infections
ETIOLOGY
Asthma results from complex interactions between genetic and environmental factors.
Prenatal and Perinatal Factors
- Preterm birth, occurring before 36 weeks, is associated with an elevated risk of asthma
- Impaired lung development in preterm infants, even in those without early respiratory complications, increases the long-term risk of asthma
- Exposure to maternal smoking during pregnancy causes diminished pulmonary function in newborns and an increased probability of developing childhood asthma
Maternal Age and Diet
- The incidence of childhood asthma increases with a maternal age of 20 or younger and decreases with a maternal age of 30 or older
- Maternal diet during pregnancy plays a role
- Vitamin D deficiency in mother during pregnancy may cause asthma in newborn
Childhood Factors
- Wheezing caused by viral infections:
- Respiratory syncytial virus
- Rhinovirus
- Air pollution
- Gas-fired appliances and indoor fires
- Obesity
- Early puberty
Adulthood Factors
- Tobacco smoke
- Occupational exposure
- Rhinitis or atopy
- Dust mites, animal allergens (from cats and dogs), cockroach allergens
- Fungi
- Physical activity or exercise
- Gastroesophageal reflux disease
- Chronic sinusitis
- Hypersensitivity to aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs)
- Use of β-adrenergic receptor blockers, including ophthalmic preparations
- Sprays and paint fumes
- Contact with insects, plants, latex, gums, wood dust
- Emotional factors or stress
ASPIRIN-EXACERBATED RESPIRATORY DISEASE (AERD)
Aspirin-exacerbated respiratory disease (AERD) is a condition characterized by a combination of:
- Asthma
- Chronic rhinosinusitis with nasal polyposis
- NSAID intolerance
Approximately 7% of adults with asthma have AERD.
Pathophysiology of AERD
- Arachidonic acid metabolism serve as potent bronchoconstrictors
- The metabolism of arachidonic acid by the 2 cyclooxygenase (COX) isoforms—COX-1 and COX-2—generates prostaglandins and thromboxanes
- PGE2 suppresses the production of leukotrienes
- Blocking of COX will deviate to lipooxygenase pathway having pro-inflammatory effects
OCCUPATIONAL-INDUCED ASTHMA
Two types of occupational asthma:
Type 1: Sensitizer-Induced Occupational Asthma
- Triggered by workplace sensitizers
- Results from an allergic or immunological process
- Associated with a latency period
- Examples include:
- Flour - contain proteins and polysaccharides of plant or animal origin
- Formaldehyde - form a sensitizing neoantigen when combined with a human protein
Type 2: Irritant-Induced Occupational Asthma
- Caused by irritants
- Involves a nonallergic or nonimmunological process
- Induced by gases, fumes, smoke, and aerosols
Mechanisms
Patients with occupational-induced asthma can undergo:
- An immunologically mediated response
- Nonimmunological occupational asthma
The possible underlying mechanisms of the nonimmunological form are:
- Direct β-2 adrenergic receptor inhibition
- Elaboration of substance P by injured sensory nerves
EPIDEMIOLOGY
- 25 million Americans are currently affected by asthma
- Among individuals younger than 18, boys exhibit a higher prevalence compared to girls
- Among adults, women are more commonly affected than men
- Asthma prevalence is notably higher among Black individuals (prevalence of 10.1%), compared to White individuals at 8.1%
- Saudi Arabia: 14% prevalence
PATHOPHYSIOLOGY
Involves interactions among inflammatory cells and airway cells. These mechanisms lead to:
- Airway inflammation
- Intermittent airflow obstruction
- Bronchial hyperresponsiveness
Airway Inflammation
- Cytokines play a key role
- Following initial allergen inhalation, affected patients produce specific IgE antibodies
- Once produced, these specific IgE antibodies bind to receptors on mast cells and basophils
- Upon additional allergen inhalation, allergen-specific IgE antibodies on the mast cell surface undergo cross-linking, leading to rapid degranulation and the release of:
- Histamine
- Prostaglandins
- This triggers contraction of the airway smooth muscle within minutes
- An influx of inflammatory cells, including:
- Monocytes
- Dendritic cells
- Neutrophils
- T lymphocytes
- Eosinophils
- Basophils
- May lead to bronchoconstriction
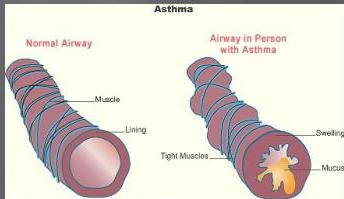
Airflow Obstruction
The narrowing of the airway lumen throughout the tracheobronchial tree is caused by:
- Contraction of airway smooth muscle
- Thickening of the airway wall due to edema
- Mucus plugging
Mediators such as histamine and leukotrienes, trigger the contraction and relaxation of airway smooth muscle.
Airway remodeling, which involves:
- Thickening of the basement membrane
- Deposition of collagen
- Shedding of epithelial cells
Can lead to irreversible changes in the airways. This process accelerates the decline in lung function.
CLINICAL EVALUATION
History
Key symptoms:
- Cough (often worse at night)
- Shortness of breath
- Wheezing
- Chest tightness
Characteristics:
- Symptoms occur intermittently, lasting for hours to days, and resolve
- Nighttime exacerbation is common
- Onset triggered by exercise, cold air, or allergen exposure
- Exercise-induced asthma symptoms typically emerge around 15 minutes into activity and dissipate within 30 to 60 minutes afterward
Associated factors:
- Atopy, such as eczema and hay fever
- Exposure to dust, animals, and infestations of rodents and cockroaches
- A strong family history of asthma and allergies
- A personal history of atopic conditions and childhood asthma symptoms
Physical Examination
Respiratory findings:
- High-pitched wheezes (note: wheezing is not specific to asthma and is typically absent between acute exacerbations)
- Tachypnea
- Tachycardia
- Prolonged expiratory phase
- Reduced air movement
- Difficulty speaking in complete sentences or phrases
- Use of accessory muscles of breathing during inspiration
- Pulsus paradoxus
Other findings:
- Pale, nasal mucous membranes
- Posterior pharyngeal cobblestoning
- Nasal polyps
- Atopic dermatitis
Important note: Nasal polyps should prompt further inquiry about:
- Anosmia
- Chronic sinusitis
- Aspirin sensitivity (to evaluate for AERD)
Asthma Without Wheezing
It is important to note that asthma can present without wheezing in some cases.
INVESTIGATIONS
Spirometry
- Spirometry assesses forced expiratory volume in 1 second (FEV₁) and forced vital capacity (FVC) by measuring a maximal inhalation followed by rapid and forceful exhalation into a spirometer
- Asthma typically presents as an obstructive pattern on spirometry, indicated by a reduced FEV₁ to FVC ratio


Bronchodilator Testing
- Nebulize with salbutamol
- Improvement in FEV1 % > 12% indicates reversibility
Bronchoprovocation Testing
- During bronchoprovocation testing, clinicians induce bronchoconstriction using:
- Inhaled methacholine
- Mannitol
- Exercise
- Eucapnic hyperventilation of dry air
- This testing method can be beneficial for patients presenting with:
- Atypical symptoms
- Isolated cough
- A fall in FEV₁ of 20% or more from baseline is considered positive
- Clinicians may also conduct additional provocative testing using:
- Exercise
- Aspirin
- Exposure to environmental triggers encountered in the workplace
Peak Flow Meter
- Use peak flow measurement to monitor patients with known asthma rather than for initial diagnosis
- To measure peak flow, the patient:
- Takes a maximal breath
- Seals the peak flow meter between their lips
- Blows forcefully for 1 to 2 seconds
Pulse Oximetry
- Pulse oximetry can help assess the severity of an asthma attack or monitor for deterioration
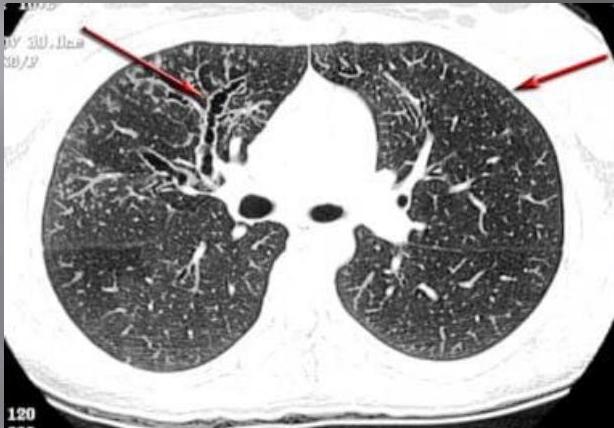
Imaging
Chest radiograph findings:
- Usually normal
- May show hyperinflation
- May reveal pneumomediastinum
When to obtain chest radiograph:
- Patients aged 40 or older with new-onset asthma
- Moderate-to-severe asthma that is difficult to control
- Presence of:
- Fever
- Chronic purulent sputum production
- Persistently localized wheezing
- Hemoptysis
- Weight loss
- Clubbing
- Inspiratory crackles
Additional imaging:
- High-resolution computed tomography (HRCT) is necessary to clarify any abnormalities noted on chest radiographs
EVALUATION DURING AN ACUTE EXACERBATION
Key assessments:
- Oxygen saturation
- Peak flow measurement
Severity classification based on peak flow:
- Below 50% predicted or the patient’s personal best → considered severe
- Between 50% and 70% → considered moderate
IDENTIFICATION OF PATIENTS AT RISK OF FATAL OR NEAR-FATAL ASTHMA
High Risk Factors
Patients at high risk for future fatal asthma exacerbations include those with:
- A recent history of poorly controlled asthma
- A prior history of near-fatal asthma
- A history of endotracheal intubation for asthma
- A history of intensive care unit admission for asthma
Minor Risk Factors
Additional risk factors include:
- Exposure to aeroallergens and tobacco smoke
- Illicit drug use
- Older patients
- Aspirin sensitivity
- Long duration of asthma
GINA GUIDELINES
GLOBAL INITIATIVE FOR ASTHMA

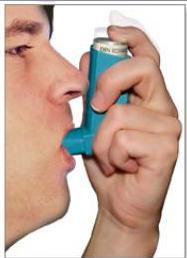
Inhaler Technique
Proper technique:
- Breathe in slowly
- Push down on the canister
- Keep breathing in deeply
Remember: ADAM

Abbreviations Used in GINA Guidelines
| Abbreviation | Full Name |
|---|---|
| SABA | Short-acting β2-agonist (short acting bronchodilator) |
| LABA | Long-acting β2-agonist (long acting bronchodilator) |
| SAMA | Short-acting muscarinic antagonist |
| LAMA | Long-acting muscarinic antagonist |
| ICS | Inhaled corticosteroid |
| OCS | Oral corticosteroid |
| LTRA | Leukotriene receptor antagonist |
Stepwise Treatment Approach
Step 1
Criteria:
- Asthma symptoms <2 times per week
- No risk factors for exacerbations
Recommendations:
- Low-dose ICS-LABA (formoterol) as needed
- Patients with exercise-induced asthma should use 1 to 2 puffs for 5 to 20 minutes before engaging in activity
Step 2
Criteria:
- Asthma symptoms or need for reliever inhaler ≥2 times per week
- No daily symptoms
Recommendations:
- Low-dose ICS-LABA (formoterol) as needed
Or:
- Low-dose ICS daily and SABA as needed
Step 3
Criteria:
- Asthma symptoms most days
- Nocturnal awakening due to asthma ≥1 time per month
- Multiple risk factors for exacerbations
Recommendations:
- Low-dose ICS-LABA (formoterol) as maintenance and reliever therapy
Other option(s):
- Low-dose ICS plus LTRA daily and SABA as needed
Step 4
Criteria:
- Severely uncontrolled asthma with ≥3 of the following:
- Daytime asthma symptoms >2 times per week
- Nocturnal awakening due to asthma
- Reliever needed for symptoms >2 times per week
- Activity limitation due to asthma
Recommendations:
- Medium-dose ICS-LABA (formoterol) as maintenance and reliever therapy
Or:
- Medium dose ICS-LABA daily and ICS-SABA as needed
Other option(s):
- Possible add-on LAMA or switch to ICS-LAMA-LABA
- Possible add-on LTRA
Step 5
Recommendations:
- A LAMA can be added
- The patient should be referred for phenotypic assessment and possible biological therapy
- High-dose ICS-LABA (formoterol) should be considered
- Possibly LTRA
- Low-dose OCS as a last resort
Acute Exacerbation Management
- LABA formoterol combined with ICS
- The SABA albuterol combined with budesonide
Home management:
- Patients whose symptoms improve after administering a bronchodilator and whose peak flow returns to 80% of their baseline or better can continue to manage their symptoms at home
Oral glucocorticoids (equivalent to 40 to 60 mg prednisone daily for 5 to 7 days) are warranted for the following patients:
- Those experiencing recurrent symptoms over the following 1 to 2 days
- Those whose peak flow remains less than 80% of their normal baseline
SEVERE ASTHMA
For patients with still uncontrolled asthma and recurrent exacerbations, consider biological therapy.
Biological therapy options:
- Anti-IgE monoclonal antibody therapy with omalizumab (subcutaneously) for patients with allergy and IgE levels ranging between 30 and 700 IU/mL
- For patients with severe eosinophilic asthma who are not adequately controlled:
- Mepolizumab
- Reslizumab
- Benralizumab
- Dupilumab
- Tezepelumab
EMERGENCY DEPARTMENT CARE
- Do ABG (Arterial Blood Gas)
- Oxygen therapy
- 3 treatments of an inhaled SABA, such as albuterol or salbutamol via a nebulizer
- Followed by repeat dosing of same every 1 to 4 hours
- Ipratropium bromide inhaler 500 µg through nebulizer then repeat every 8 hours
IV Steroids
- Start IV steroids if patient is not improving
- Methylprednisolone 60 to 80 mg
Magnesium Sulfate
- 1-time dose of 2 g given intravenously over 20 minutes
- Reduces hospitalization rates in adults with:
- An FEV₁ less than 25% to 30% predicted on presentation
- Those who fail to respond to initial treatment and continue to have hypoxemia
Intubation or Noninvasive Ventilation
Indications for intubation and mechanical ventilation or noninvasive ventilation include:
- Slowing of the respiratory rate
- Depressed mental status
- Inability to cooperate with the administration of inhaled medications
- Worsening hypercapnia and associated respiratory acidosis
- Inability to maintain oxygen saturation above 92% despite face mask supplemental oxygen
PROGNOSIS
Factors affecting prognosis:
- Genetic and environmental factors
- Social determinants of health, such as:
- Poor housing quality
- Indoor and outdoor pollution
Mortality statistics:
- The international asthma mortality rate is high
- Prognosis is predominantly linked to lung function, with mortality rates 8 times higher among individuals in the bottom 25% of lung function
Factors contributing to poorer prognosis:
- Inadequate asthma management
- Age 40 or older
- Cigarette smoking
- Blood eosinophilia
- FEV1 of 40%
WHEN YOUR PATIENT DENIES ANY MEDICAL HISTORY