Bronchiectasis
Presented by: Dr. Nada Abdelrahman

Learning Outcomes
By the end of this lecture, the student should be able:
- ☐ Define the aetiology and pathogenesis of bronchiectasis.
- ☐ Recognize the clinical features of bronchiectasis
- ☐ Diagnose and manage a case of bronchiectasis.
- ☐ Outline the complications and prognosis of bronchiectasis
Overview
Definition Prognosis Management Investigations



Aetiology Pathophysiology Clinical Features Differential diagnosis
Definition
Bronchiectasis (broncos, airways; ectasia, dilatation)
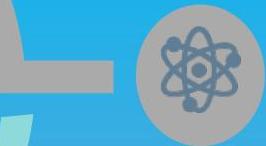
- ☐ It is a morphological term used to describe abnormal irreversibly dilated and often thick-walled bronchi.
- ☐ It result from a variety of pathologic process that cause destruction of the bronchial wall and its surrounding supporting tissues

Definition (Morphology)
Aetiology
Mechanical Bronchial Obstruction (Focal)
- Foreign body
- Tumour (e.g. Lymph node Tumour)
- Inspissated mucus
- Post-tuberculous stenosis
Intrinsic and Extrinsic Factors
- Allergic bronchopulmonary aspergillosis (Immunological over-response)
- Post-lung transplant
- Graft-versus-host disease
- RA, IBD, Sjögren’s syndrome
- Diffuse diseases of the lung parenchyma
Congenital and Primary Conditions
- Primary : congenital
- Acquired: Young’s syndrome (azoospermia, sinusitis)
- Mucociliary clearance defects (Interstitial)
- Cystic fibrosis, α1 antitrypsin
- Ciliary dysfunction syndromes:
- Immotile cilia syndrome
- Kartagener’s syndrome
- Mounier-Kuhn (tracheobronchomegaly)
Post-Infective and Bronchial Damage
- Granuloma
- Post-infective
- Bronchial damage
- Tuberculosis C sarcoidosis
- Bacterial and viral pneumonia: Including pertussis, measles and aspiration pneumonia.
Immune Deficiency
- Primary:
- Panhypogammaglobulinaemia
- Selective immunoglobulin deficiencies (IgA and IgG2)
- Secondary:
- HIV, malignancy

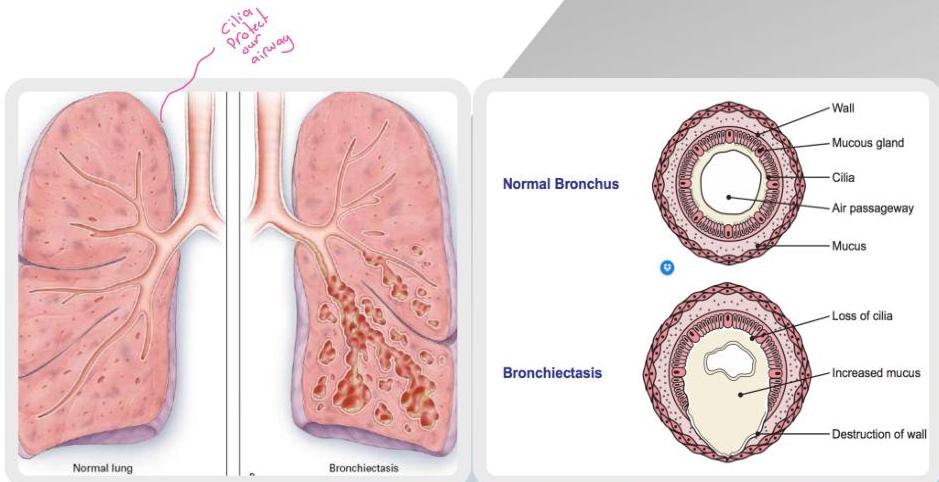
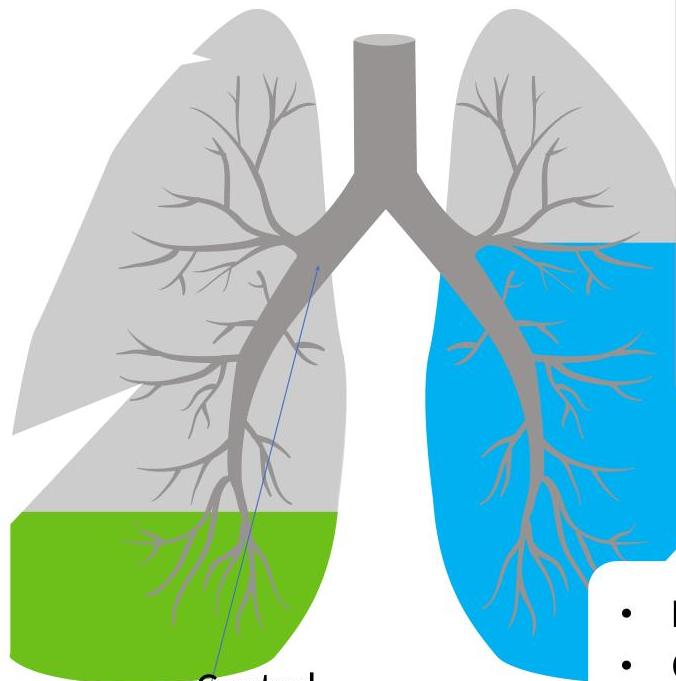
Pathophysiology
Focal bronchiectasis: bronchiectatic changes in a localized area of the lung.
Diffuse bronchiectasis: widespread bronchiectatic changes throughout the lung.
Medium-sized bronchi, but often extends to the more distal bronchi and bronchioles.
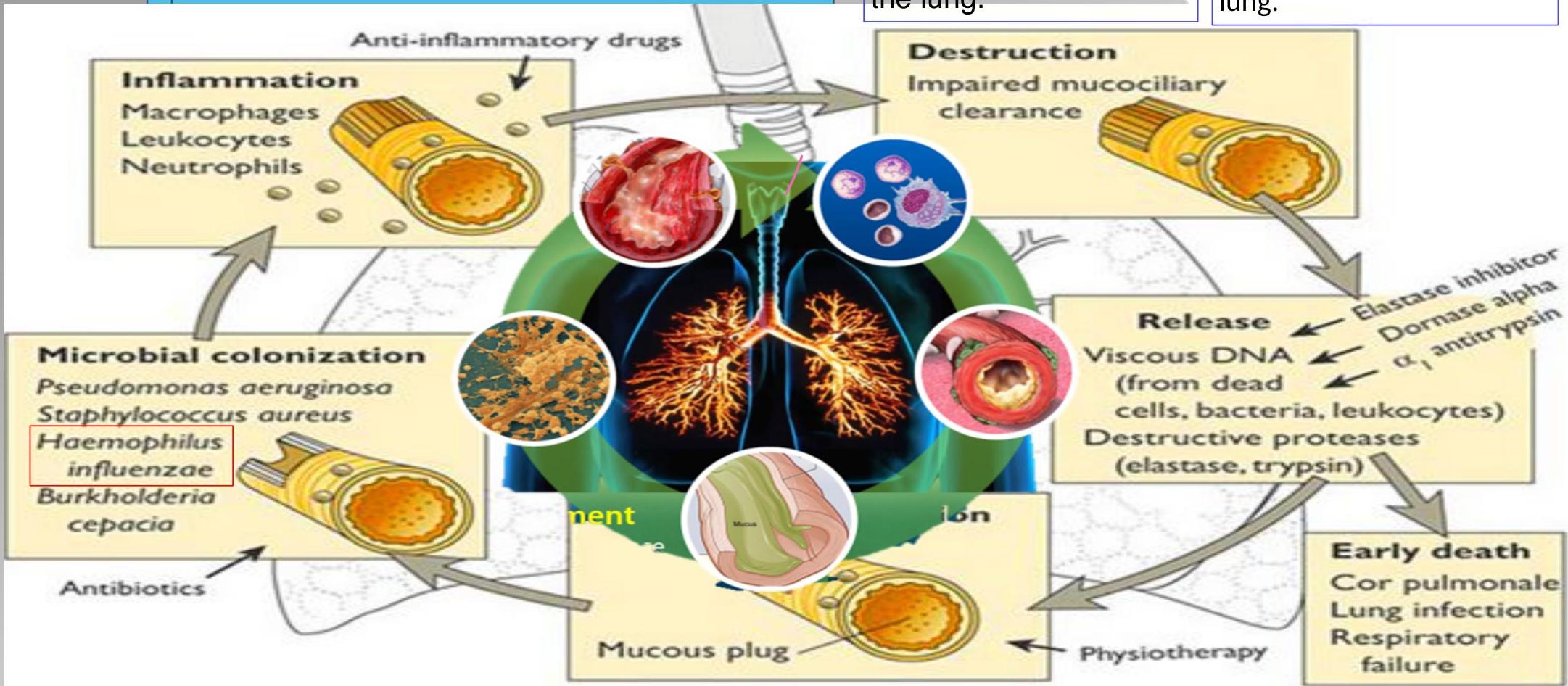
Histological Changes
 Normal
Normal
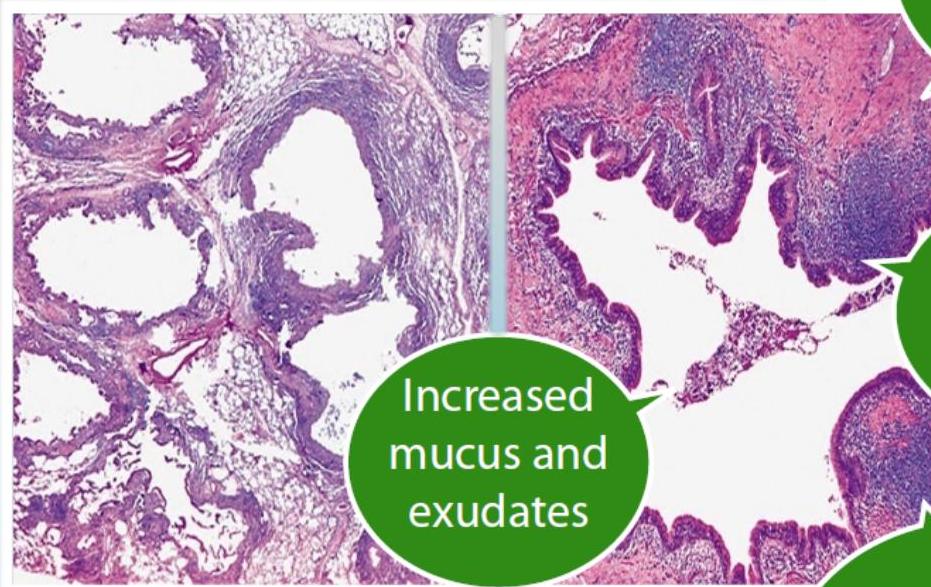 Bronchiectasis
Bronchiectasis
- Increased mucus and exudates
- Cartilage destruction and fibrosis

- Mucosal and mucous gland hyperplasia
- Inflammatory cells infiltration
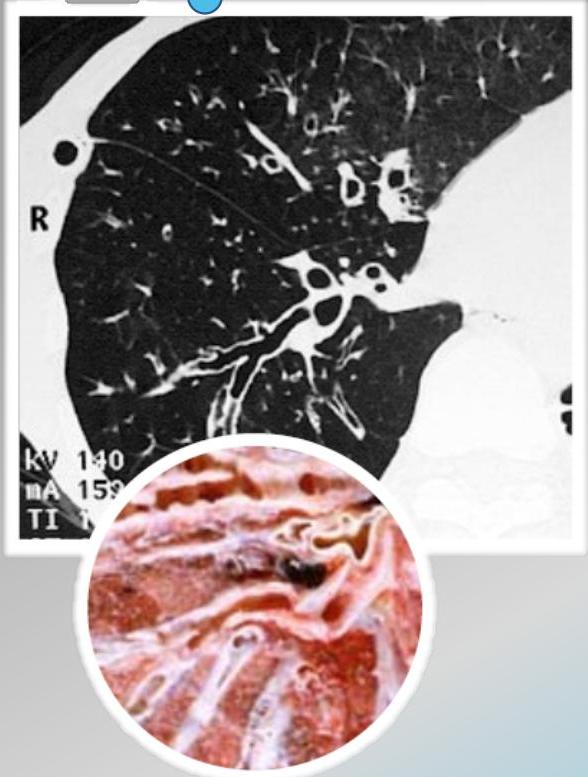
Morphological Forms
 Cylindrical
Cylindrical
Diffuse Bronchiectasis Predominance
- cystic fibrosis (CF)
- postradiation fibrosis
- Sarcoidosis
- Mycobacterium avium-intracellulare complex (MAC)
- Congenital causes: Immotile cilia syndrome
- Allergic bronchopulmonary aspergillosis
Forms of Bronchial Dilatation
Dilatations of the air sacs occur due to bronchiectasis, as depicted below.

- Idiopathic
- Chronic recurrent aspiration (e.g scleroderma)
- Traction bronchiectasis from idiopathic pulmonary fibrosis
- Recurrent immunodeficiency-associated infections
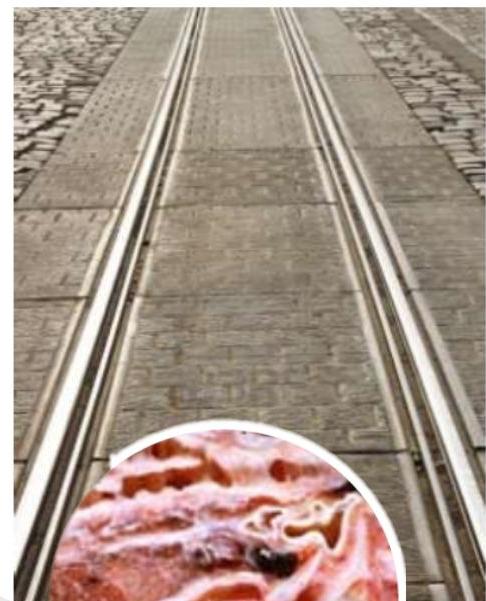
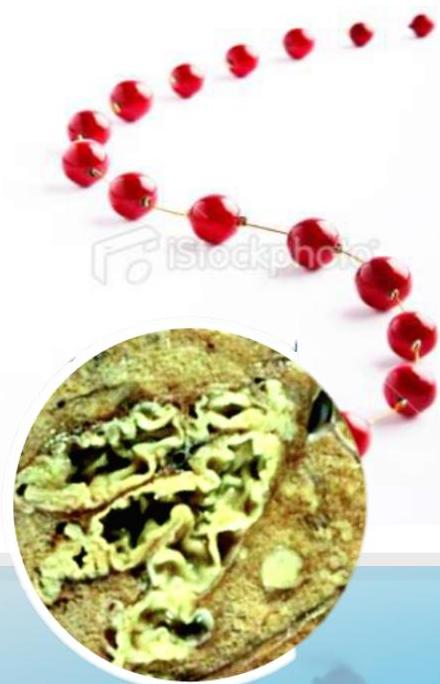
Morphological Classification
| Cylindrical bronchiectasis | Varicose bronchiectasis | Cystic bronchiectasis |
|---|---|---|
| Mild | Moderate | Sever |
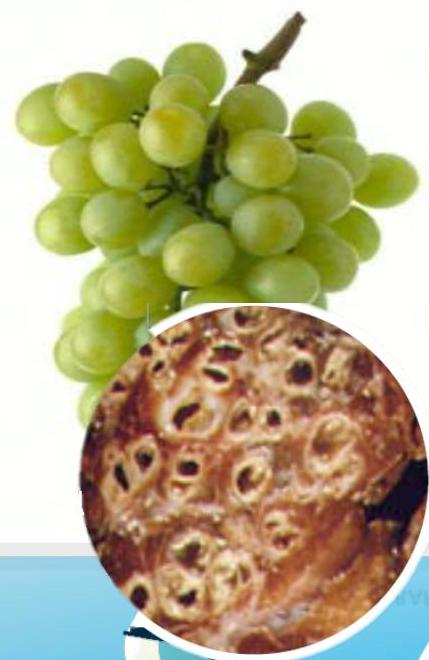
| Tram track appearance | String of beads | Cluster of grapes |

Clinical Features
Respiratory Symptoms
- Cough: Persistent, Productive of large amounts and Purulent. (thick, tenacious). Often worse in the early morning.
- Breathlessness: exertional dyspnoea.
- Haemoptysis: Common, sign of infection. Streaks of blood C. Massive amounts can occur.
- Halitosis: Bias smell.
Physical Signs
- Clubbing: Other background: Lung, Mouth.
- Chest examination:
- Bilateral / unilateral
- Coarse crackles
- Wheezing
- Normal (in some cases)
Acute Exacerbations (Infection)
- Increased volume and purulence of sputum.
- Pleuritic chest pain
- Fever, malaise, anorexia, weight loss






Diagnosis

Clinical History
- Chronic productive cough*
- Sputum production*
- Reported bouts of respiratory tract infection
Physical Examination
- Wheezing, rhonchi, crackles
- Clubbing
- Cyanosis
Associated/Causative Conditions
- Bronchial obstruction: localized wheezing
- ABPA: Prominent wheezing
- CTDs: Arthritis, Sicca syndrome
- PCD, CF, Young Syndrome: Recurrent sinus disease, Infertility
Diagnostic Investigations
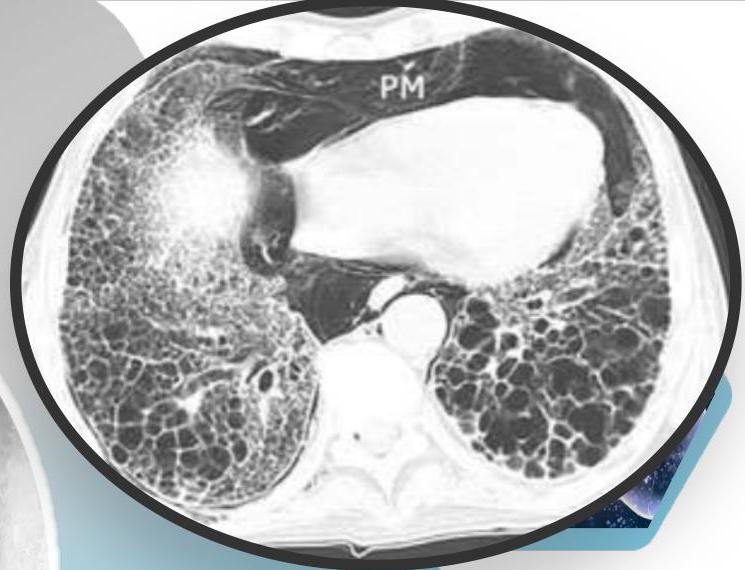
- ☐ Thin-section HRCT scanning: is the gold standard, with excellent sensitivity and specificity.
- ☐ Chest X-ray: increase in size and loss of bronchovascular markings, crowding of bronchi, and loss of lung volume. Severe case: Honeycombing.
- ☐ Sputum examination and culture: choice of antibiotic/ exclud.



- ☐ Immune assessment: immunoglobulins and responses to Hib, tetanus and pneumococcal vaccines.
- ☐ Sweat test and cystic fibrosis genetic assessment.
- ☐ Nasal nitric oxide test for screening for primary ciliary dyskinesia (PCD).
- ☐ Total IgE and Aspergillus-specific IgE or Aspergillus skin-prick testing : to exclude allergic bronchopulmonary aspergillosis.
- ☐ Spirometry: obstructive pattern.
Radiographic Findings (Chest X-ray)
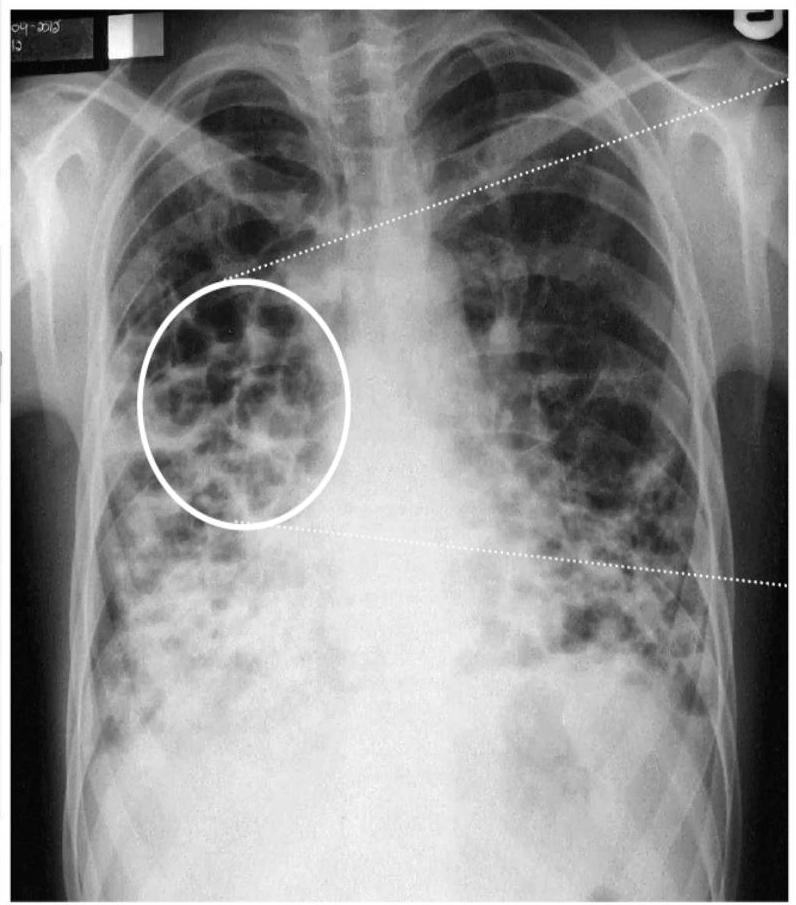
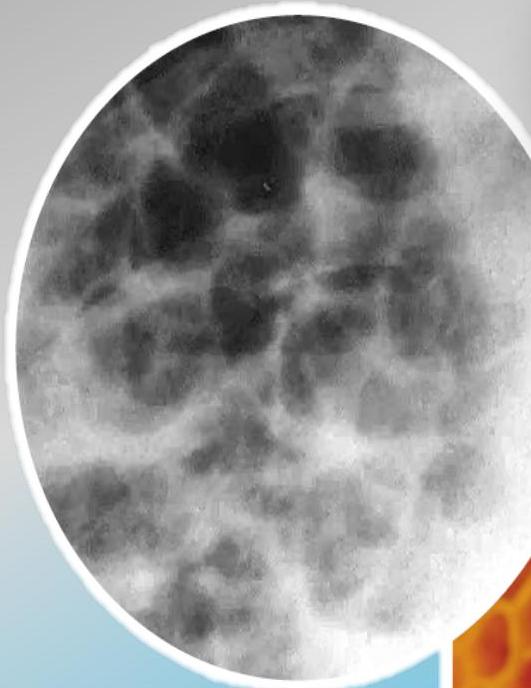
Conglomerating cysts of varying size and wall thickness. “Honeycomb” sign.
Radiographic Findings (Signs)
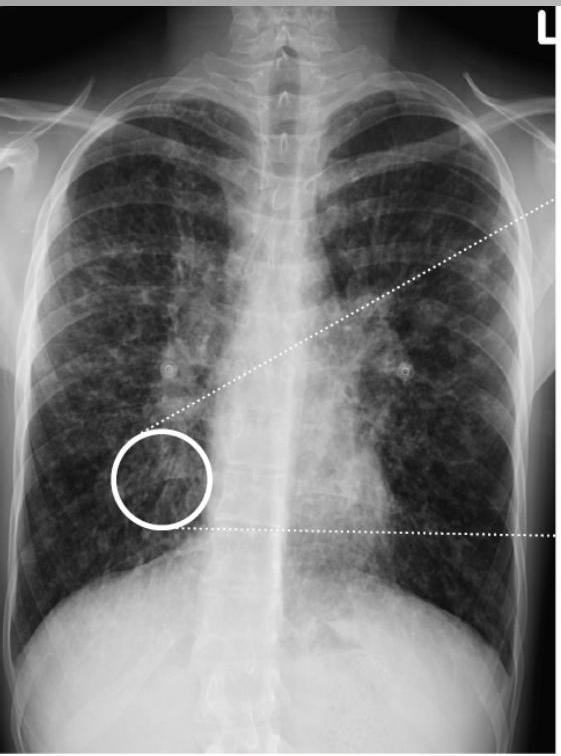


Bronchial wall thickening and widening with parallel configuration. Tram track sign.
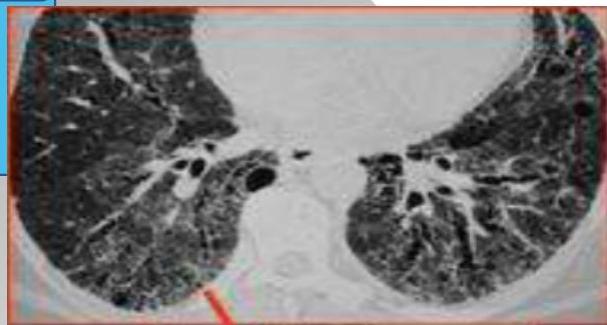
CT Scan Findings
 Cylindrical
Cylindrical
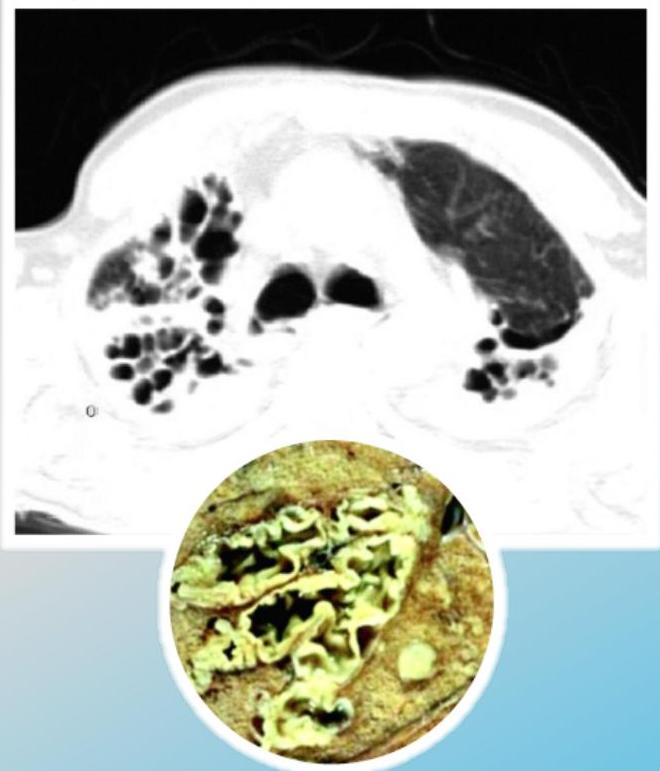 Saccular/Varicoid
Saccular/Varicoid
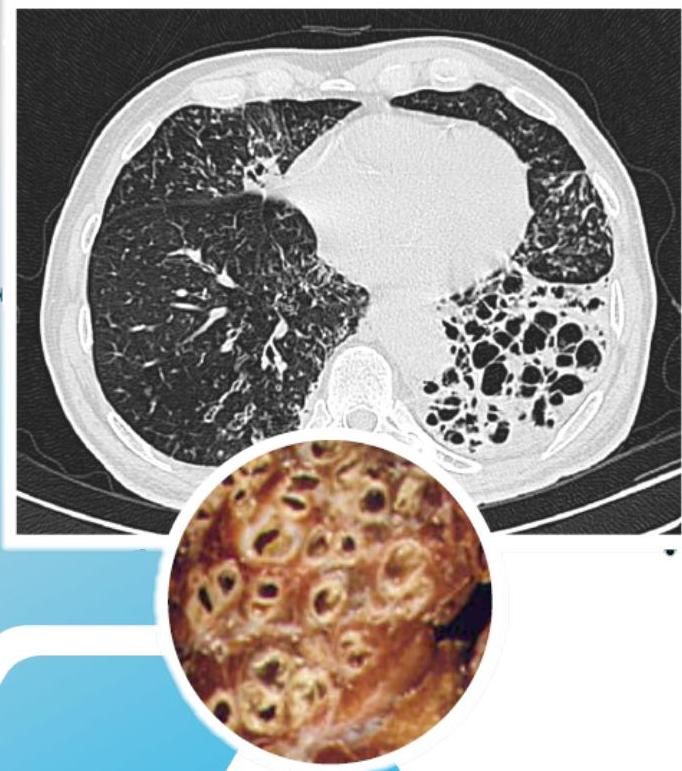 Cystic
Cystic
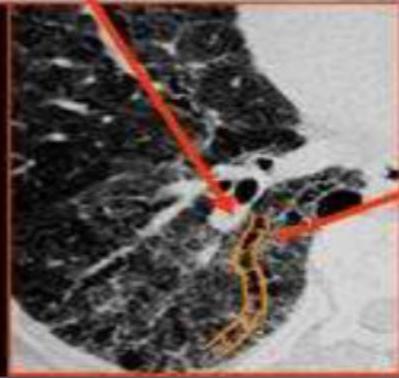
Signet Ring Appearance
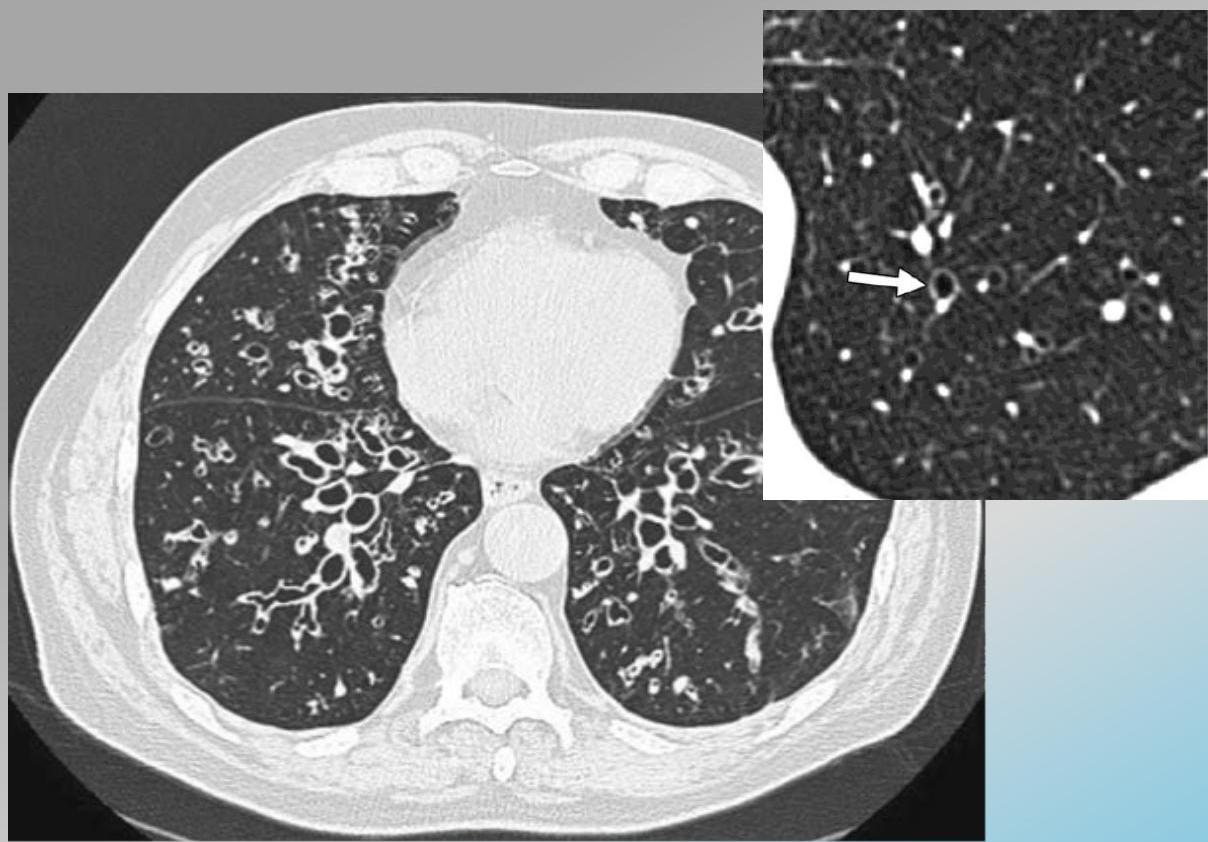
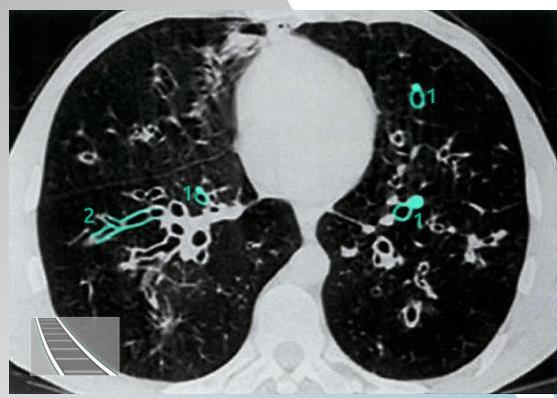

CT scan showing bronchiectasis. Note the dilated bronchi with thickened wall, which are larger than adjacent arteries, giving a signet ring appearance.
Management
Airway Clearance
- Chest physiotherapy: Postural drainage
- Mucolytics: Nebulized hypertonic saline
Anti-inflammatories
- ☐ Long-term azithromycin → macrolides
- ☐ Inhaled corticosteroid & bronchodilators
Treatment of Infection
- ☐ Pseudomonas aeruginosa: dual therapy. Ciprofloxacin or IV anti-pseudomonal β-lactam (e.g. piperacillin)
- ☐ H. influenzae infection: oral antibiotics such as amoxicillin, co-amoxiclav, doxycycline. Or IV cephalosporin
- ☐ Cystic fibrosis: colistimethate or an aminoglycoside for P. aeruginosa. Need 2 weeks of IV for exacerbation
Practices to Avoid
- Rotating oral antibiotic regimes
- Long-term quinolones

Surgical Treatment
- ☑ Localized: Lobectomy
- ☑ Artery embolization: For massive haemoptysis. For massive haemophysis.
Prognosis and Complications
Complications
- ☐ Secondary bacterial infections
- ☐ Aspergillus lung disease and non-tuberculous mycobacteria
- ☐ Massive Life-threatening haemoptysis
- ☑ Respiratory failure
- ☐ Pulmonary artery hypertension(PAH) & Cor pulmonale
-
- Aspergilloma
-
- Brain abscess
-
- Secondary amyloidosis

Prognosis
- Variable
- Worse outcome with: A low FEV1 and infection with P. aeruginosa
- *Low graded fever means bad prognosis*
Prevention
- Vaccination
- Treatment of bronchial obstruction
References
Clark & Kumar: 982-985


