COPD
https://next.amboss.com/us/article/3h0Sdf?q=chronic+obstructive+pulmonary+disease
Definition
COPD is a chronic disease of the lungs in which there is:
- Obstruction/narrowing of small airways, which is not fully reversible. This limits the airflow, mainly during expiration
- Inflammation in the airways
- Gas exchange problem in the alveoli
It is a preventable & treatable disease.
Etiologies
- Smoking: Most common cause worldwide
- Smoke from burning fossil fuels, e.g., coal, wood, oil, etc.
- Climate pollution
- Occupational exposure to harmful gases/particles (e.g., coal miners)
- Alpha-1 antitrypsin deficiency (COPD at a young age + cirrhosis)

Classification
Two conditions come under COPD:
- Emphysema
- Chronic bronchitis
Most COPD patients have a combination of both.
Emphysema
Emphysema is characterized by:
- Narrowing of the terminal bronchioles plus destruction of the alveolar walls
This leads to:
a) Hyperinflation: During expiration, lungs don’t collapse fully, so air gets trapped inside (so total lung capacity TLC is increased)
b) Gas exchange problems: Alveolar damage → poor gas exchange causing hypoxia and CO₂ retention
Clinical Features:
- Patients are breathless but not cyanosed
- CO₂ retention is not so bad like chronic bronchitis
- These patients are called “pink puffers” (skin is pinkish)
Normal vs. Emphysema

Alveoli Changes in Lung Diseases
NOTE THE ALVEOLAR WALL DAMAGE

alamy - CT2782
Chronic Bronchitis
Chronic bronchitis is defined as:
- Productive cough, for 3 consecutive months, for at least 2 years (in the absence of any other etiology) → 3M 2Y
Features:
a) Hypoxia & CO₂ retention (CO₂ retention is much more than emphysema)
b) Patients cyanosed & edematous (blue bloaters)
Comparison: Emphysema vs. Chronic Bronchitis
| Feature | Emphysema | Chronic Bronchitis |
|---|---|---|
| 1) Hypoxia | Yes | Yes |
| 2) CO₂ retention | Yes, but not too much | Too much |
| 3) Cyanosis | No | Yes |
| 4) Skin color | Pink puffers | Blue bloaters |
COPD Phenotypes
 Pink Puffer
Pink Puffer
 Blue Bloater
Blue Bloater
Symptoms of COPD
Primary Symptoms:
- Dyspnea
- Productive cough
- Wheezing/chest tightness
Important Notes:
- Initial stages are asymptomatic. Signs/symptoms appear when it is advanced.
- Patients frequently have acute exacerbations, mostly due to viral infections and exposure to pollutants.
Physical Findings
Physical signs of COPD are present only in advanced disease.
1) Inspection
- Cyanotic or pink color
- May look dyspneic
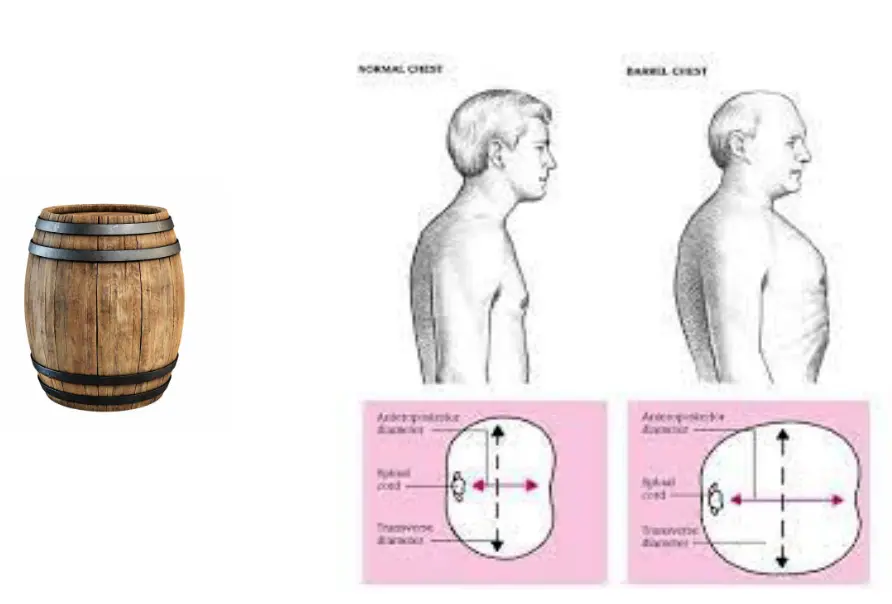
- Hyperinflated barrel chest
- Use of accessory muscles of respiration
2) Palpation
- Decreased chest expansion
3) Percussion
- Hyper resonant chest (why?)
4) Auscultation
- Decreased breath sounds
- Wheezing & crackles may be present
Barrel Chest
Important Note on Clubbing
CLUBBING IS NOT A FEATURE OF COPD
Complications
-
Type 2 respiratory failure (low O₂, high CO₂)
- (high CO₂ can cause ---?)
-
Pulmonary hypertension
-
Right heart failure (cor pulmonale) due to (2)
-
Polycythemia (in emphysema)
-
Pneumothorax (due to rupture of bullae)
- (Bullae are small air cavities in the lungs, often seen in COPD & asthma)
Bulla

Investigations
1) Chest X-Ray (CXR)
- Hyperinflated dark lung fields
- Poor vascular markings
- Flattened diaphragm
- Wide intercostal spaces
- Bullae may be seen
COPD on X-Ray


Normal X-Ray

2) Spirometry

Key Spirometry Measurements
FEV₁ (Forced Expiratory Volume in 1 second) → air coming out in the 1st sec. of expiration
FVC (Forced Vital Capacity) → total air coming out forcefully (after a deep inspiration)
Spirometry Findings in COPD
- Spirometry is definitive for diagnosis (in the context of history & examination)
- Shows an obstructive pattern
- FEV₁ is reduced, FVC is reduced & FEV₁/FVC ratio is also reduced (obstructive pattern)
- FEV₁/FVC ratio is always less than 0.7 (<70%)
- Residual volume (RV) high due to air trapping
- Total lung capacity (TLC) increased due to air trapping
3) CT Chest
- Shows more detailed pathology but not done routinely
4) CBC
- May show polycythemia
5) Arterial Blood Gas (ABG)
- Shows Type 2 respiratory failure in late COPD (low O₂, high pCO₂)
Most COPD patients have high PCO₂ in ABG, even at baseline. They are stable with this PCO₂.
6) ECG
May show features of cor pulmonale:
- Right axis deviation

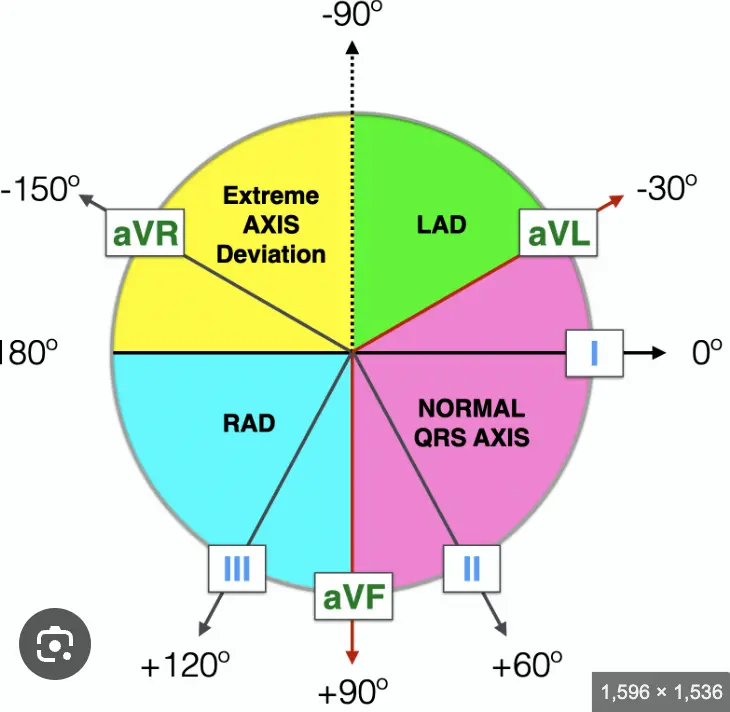
- Right ventricle hypertrophy
When to Suspect COPD
Consider COPD in anyone who has:
- Chronic cough, dyspnea and sputum, PLUS
- History of exposure to risk factors like smoking or environmental pollution, PLUS
- FEV₁/FVC ratio less than 0.7, even after bronchodilation
Severity of COPD (GOLD Criteria)
Based on FEV₁, COPD has 4 severity stages:
| GOLD Stage | Severity | FEV₁/FVC | FEV₁ % of Predicted |
|---|---|---|---|
| GOLD I | Mild COPD | <0.7 | >80% |
| GOLD II | Moderate COPD | <0.7 | 50-80% |
| GOLD III | Severe COPD | <0.7 | 30-50% |
| GOLD IV | Very Severe COPD | <0.7 | <30% |
GOLD: Global Initiative for Chronic Obstructive Lung Disease
FEV₁: Forced Expiratory Volume in 1 second
FVC: Forced Vital Capacity
Management
COPD is a chronic disease but it is characterized by acute exacerbations, due to various factors. So, there is:
- Treatment of the chronic stable patient
- Treatment for acute exacerbations
Aims of Chronic Treatment
- To improve signs/symptoms
- To reduce exacerbations
- To improve survival
- To slow the disease progression
Treatment of Chronic Stable Patient
- Stop smoking & avoid exposure to pollutants
- Inhaled bronchodilators
- Inhaled corticosteroids (ICS)
- Theophylline (not routinely)
- Oxygen therapy
Only smoking cessation & O₂ therapy have shown to improve survival.
1) Smoking Cessation
- Most important step
- Survival is improved & lung function also improves
- Formal smoking cessation programs are very helpful
- Can also use anti-smoking meds (Nicotine patches, varenicline)
- Avoid exposure to pollutants e.g., wood fire
2) Inhaled Bronchodilators
Foundation of COPD treatment. Produce bronchodilation.
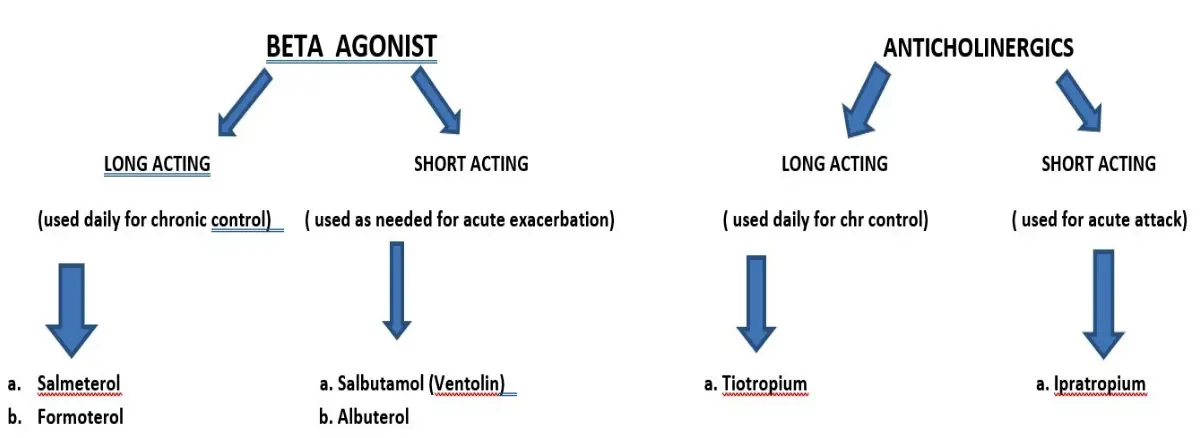
a) Beta-Agonists:
- Short-acting (e.g., salbutamol, Ventolin)
- Long-acting (LABA) (e.g., salmeterol, formoterol)
b) Anticholinergics:
- Short-acting (ipratropium)
- Long-acting (tiotropium)
(Short-acting meds are used “AS NEEDED” for acute attack while long-acting are used daily as a baseline therapy)
Bronchodilators
BETA AGONIST
LONG ACTING
(used daily for chronic control)
- a. Salmeterol
- b. Formoterol
SHORT ACTING
(used as needed for acute exacerbation)
- a. Salbutamol (Ventolin)
- b. Albuterol
ANTICHOLINERGICS
LONG ACTING
(used daily for chr control)
- a. Tiotropium
SHORT ACTING
(used for acute attack)
- a. Ipratropium
3) Inhaled Corticosteroids (ICS)
- They reduce inflammation in the airways
- Examples: Fluticasone, Budesonide
“Inhaled” steroids are used long-term while I.V. steroids are used for acute attack.
Combinations of a LABA & ICS are available & widely used as chronic baseline therapy.
Important Notes on Bronchodilator Use
- Short-acting bronchodilators are used for acute exacerbations (they have a quick onset of action), while long-acting agents are used daily for chronic treatment.
- Short-acting agents can be used as “inhalers” or nebulizer solutions
- Short-acting agents are not available in combination with steroids
LABA & ICS Combination
ICS + Beta Agonist
DEVICE USED TO INHALE:


ANOTHER LABA + ICS: ICS + Salmeterol



Very Important
Poor inhaler technique is a very common cause of not responding to medicines.
4) Theophylline (Aminophylline)
- Not used too much now, due to toxicities
- Sometimes added if inhaled bronchodilator therapy is not helping
- If patient already taking it, don’t stop (COPD will worsen)
5) Oxygen (Long-Term Oxygen Therapy - LTOT) Z
- Do ABG → start O₂ if pO₂ is low
- Some patients need it 24 hrs, while others need it for few hours daily
- Best is at least 15 hrs/day
Indications of LTOT Z
- pO₂ of less than 55 mmHg on ABG (even after maximum therapy). Should be done twice, & not during acute exacerbation
- pO₂ between 55 to 60, if complications are present (pulmonary HTN, cor pulmonale)
(Normal pO₂ is 60 and above)
Portable Oxygen


Benefits of LTOT
- Improves survival (what else improves survival?)
- Improves pulmonary HTN & cor pulmonale
- Symptomatic improvement & sense of well-being
Important Warning
Be careful when giving O₂ to COPD patients. It can worsen the CO₂ (why?)
Other Modalities in Management
-
Pulmonary Rehabilitation: Includes exercise training, nutritional counselling, social support. Should be done for all patients with moderate to severe COPD.
-
Vaccinations:
- Yearly flu vaccine
- Pneumovac every 5 years
Monitoring the Patient’s Progress
How to monitor:
- By spirometry
- By history
Acute COPD Exacerbation
Characteristics:
- Caused by viral/bacterial chest infection or exposure to pollutants (commonest is viral)
- Worsening of signs/symptoms acutely
- ABG shows severe hypoxia & worsening CO₂
Treatment of Acute Exacerbation
- Nebulization with high doses of short-acting bronchodilators (Ventolin +/- ipratropium)
- Oral, I.V. or inhaled steroids
- “Controlled” oxygen (if needed)
- If still no improvement → ventilation
Indications for Ventilation During Acute Attack
- CO₂ very high
- Mental status changes (due to high CO₂)
- No improvement with maximum therapy (oxygen in blood still very low even after giving O₂)
2 ways of ventilation:
a) Intubation and ventilation (if patient drowsy)
b) Non-invasive ventilation (BiPAP) - If patient is awake
Example of Non-Invasive Ventilation: BiPAP
BiPAP = Bilevel Positive Airway Pressure Ventilation
BiPAP is never used in a drowsy patient.

Clinical Case
Patient Presentation:
- Chronic smoker
- Looks bluish & bloated
- Complains of moderate dyspnea since few months & also productive cough for 2 years
- AP diameter of the chest is high
- FEV₁: FVC ratio is less than 0.7, gets only slight improvement after Ventolin
What’s the Diagnosis?
- Asthma
- Chronic bronchitis ✓
- Emphysema
Summary: Very Important Points
LAST SLIDE IS VERY IMPORTANT
