Dyslipidemia: Pathophysiology, Diagnosis & Management
Dr. Eatimad Mahgoub Osheik
Assistant Professor, MD Internal Medicine
Learning Objectives
- Define dyslipidemia
- Understand lipid metabolism
- Interpret lipid profile
- Identify ASCVD risk
- Apply ACC/AHA guidelines
- Choose appropriate therapy
Background
- Lipids are organic water non soluble molecules
- Major types include:
- Triglycerides: serving as long term energy store
- Phospholipids: key component of cell membrane
- Cholesterol: vital for building cells, producing hormones (like estrogen, testosterone, vitamin D), and making bile for digestion and brain development
- Cholesterol and triglycerides are carried in the bloodstream by spherical particles called lipoproteins
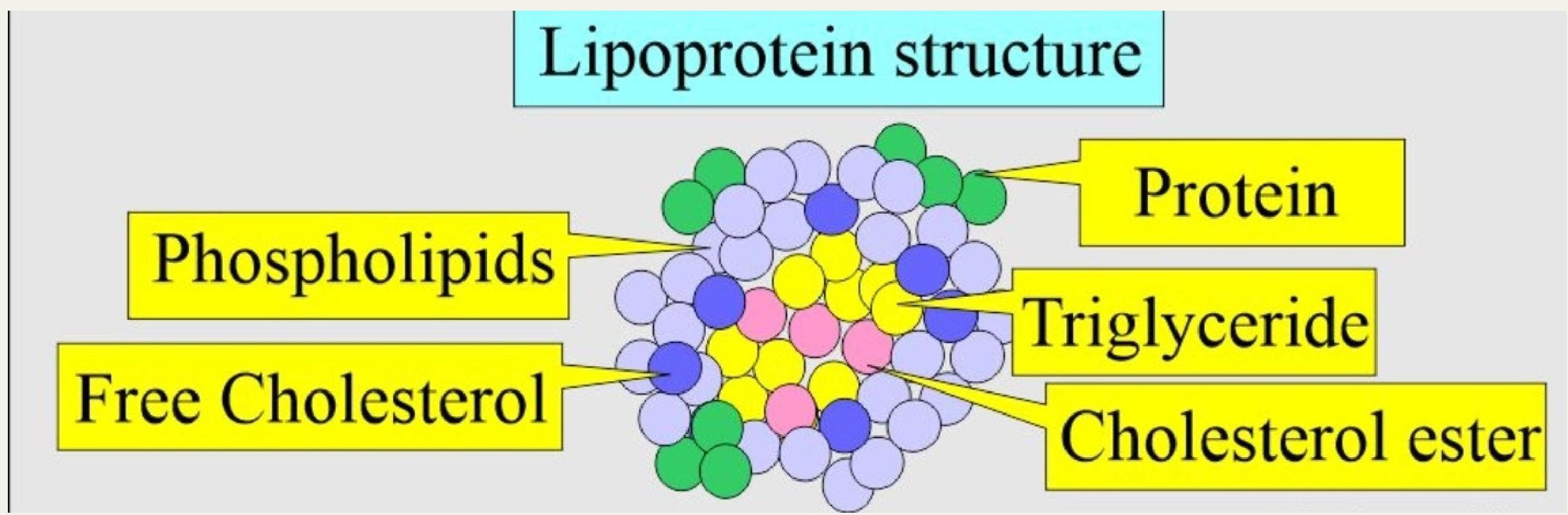
What is Lipoprotein?
A lipoprotein is a complex particle made of lipids like cholesterol, triglycerides and a protein that acts as the body’s transport system for these fats through the bloodstream to cells.
Structure and Function
- Core: Contains fats like triglycerides and cholesterol
- Outer Shell: Composed of phospholipids and special proteins called apolipoproteins (like ApoB for LDL, ApoA-I for HDL)
- Function: To carry fats to and from cells throughout the body
Lipid Metabolism: Lipoprotein Types
- Chylomicrons
- VLDL (Very Low-Density Lipoprotein)
- IDL (Intermediate-Density Lipoprotein)
- LDL (Low-Density Lipoprotein)
- HDL (High-Density Lipoprotein)
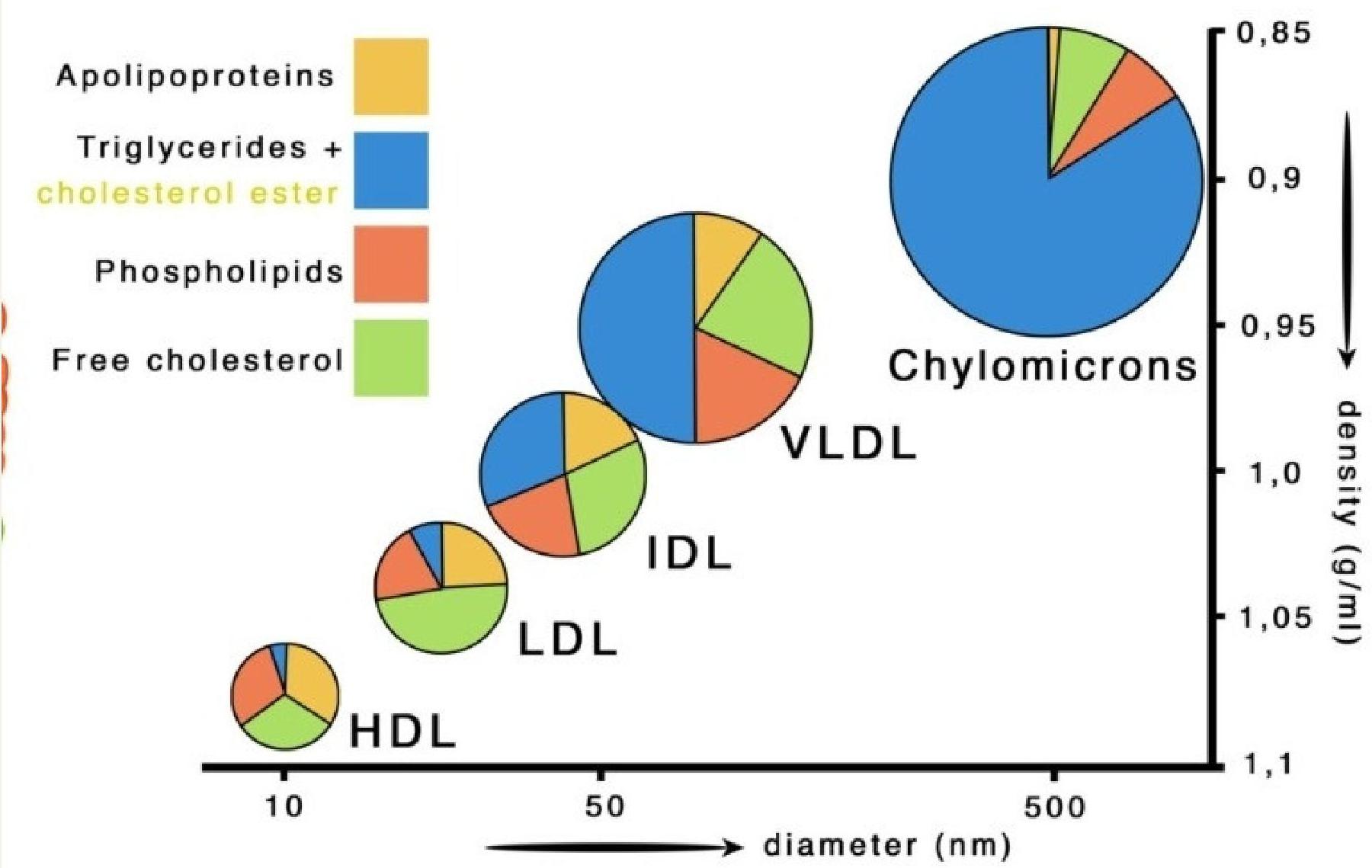
Major Types, Density, and Size
- Chylomicrons: Largest and least dense, transport dietary fats from the gut
- VLDL: Large, low density, carries triglycerides from the liver
- IDL: Medium, intermediate density, derived from VLDL
- LDL: Smaller, delivers cholesterol to tissues
- HDL: Smallest, removes cholesterol from tissues, “good” cholesterol
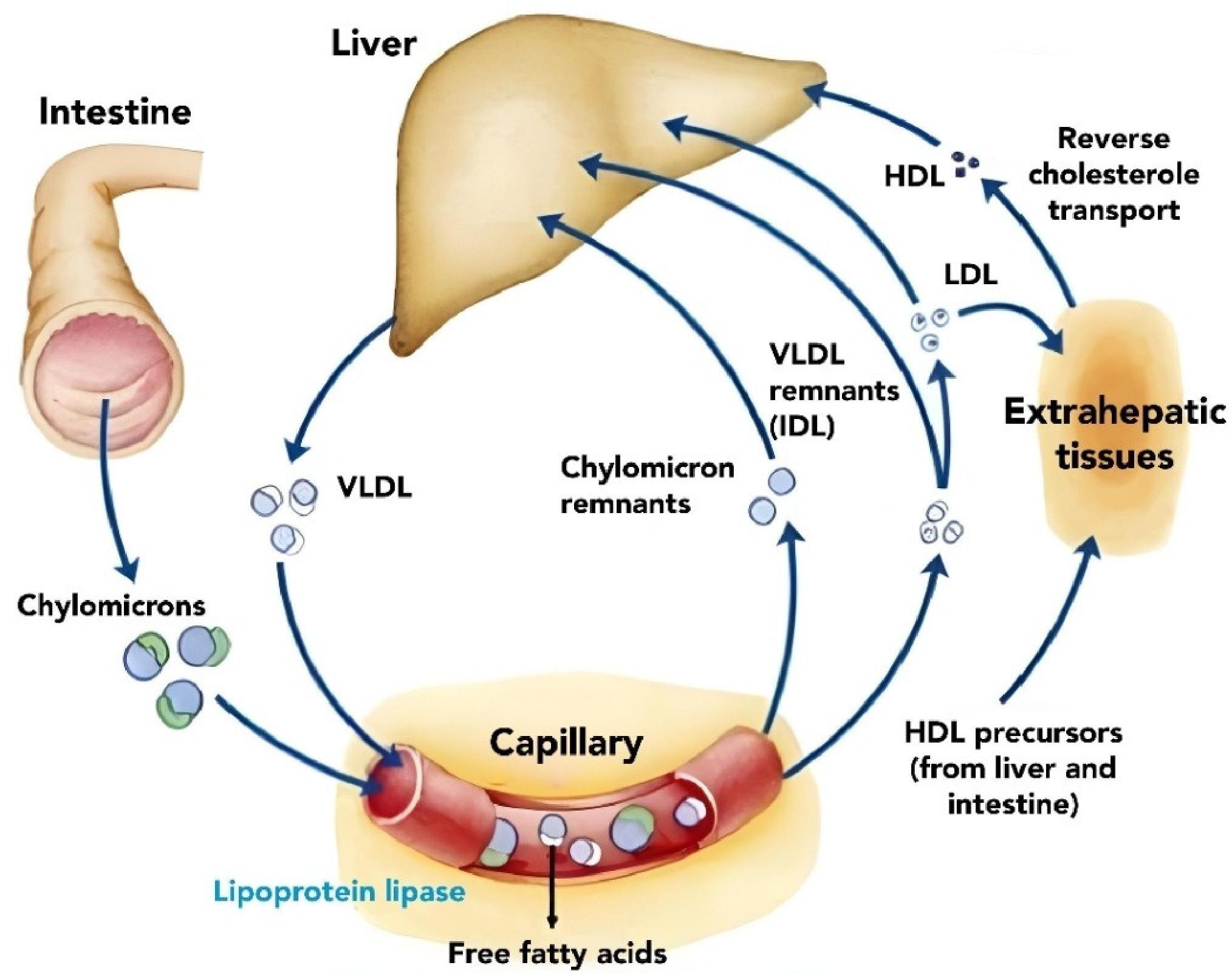
Lipid Metabolism Pathway
Introduction to Dyslipidemia
- Dyslipidemia = abnormal lipid levels in the blood
- Consequence of abnormal lipoprotein metabolism
- Major modifiable risk factor for ASCVD
- Strong association with:
- Coronary artery disease
- Stroke
- Peripheral arterial disease
Dyslipidemia Types
Includes:
- ↑ Low Density Lipoprotein (LDL)
- ↓ High Density Lipoprotein (HDL)
- ↑ Triglycerides (TG)
- Mixed dyslipidemia
Classification of Hyperlipidemia
Primary Hyperlipidemia
Single or multiple gene defect results in disturbance of LDL, HDL or/and TG production or clearance
Fredrickson Classification:
- Type I: Familial Chylomicronemia
- Type IIa: Familial Hypercholesterolemia
- Type IIb: Familial Combined Hyperlipidemia
- Type III: Dysbetalipoproteinemia
- Type IV: Hypertriglyceridemia
- Type V: Mixed Chylomicronemia-VLDL Elevation
When to Suspect Primary Hyperlipidemia
- Early onset hyperlipidemia (childhood or young adulthood)
- Strong family history of premature cardiovascular disease
- Very high lipid levels:
- LDL-C ≥190 mg/dL
- Triglycerides ≥500 mg/dL
- Poor response to diet and lifestyle changes
- No secondary cause
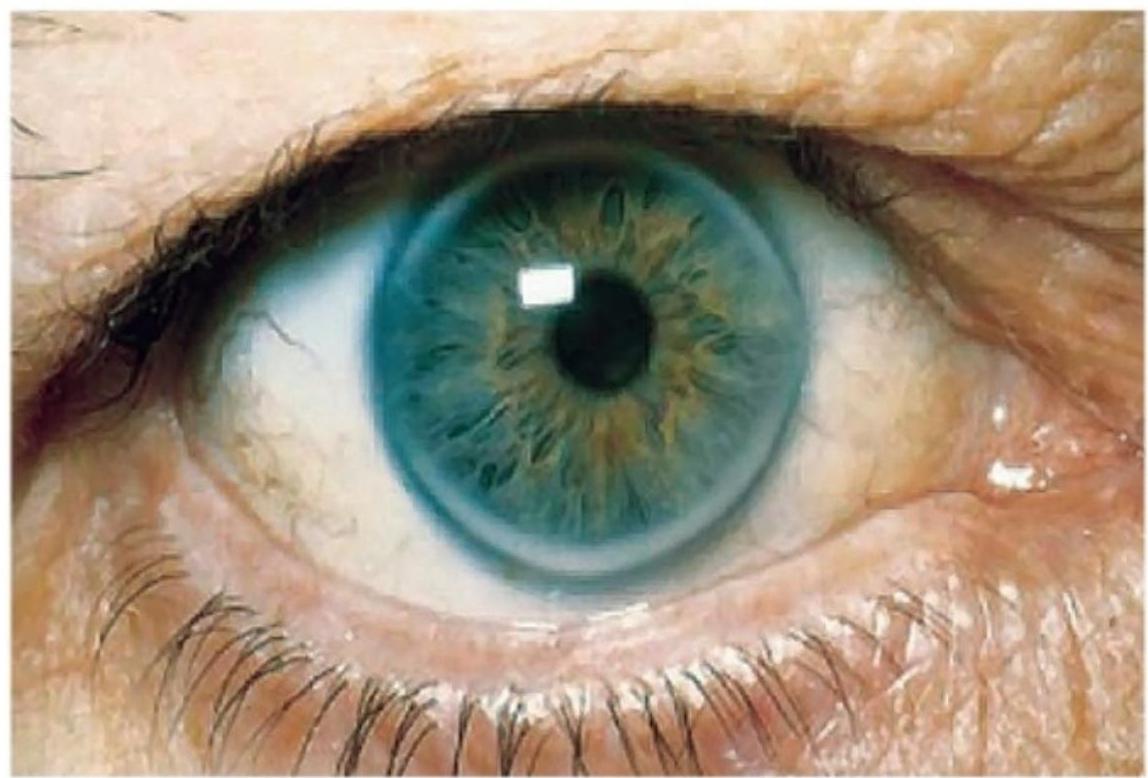
- Characteristic signs: tendon xanthomas, xanthelasma, corneal arcus at young age
Clinical Signs of Primary Hyperlipidemia



Secondary (Acquired) Hyperlipidemia
Causes:
- Endocrine causes: diabetes mellitus, hypothyroidism, obesity
- Renal disease: nephrotic syndrome, chronic renal failure
- Hepatic dysfunction: cholestasis
- Medications: thiazide diuretics, β-blockers, oral estrogens, steroids
- Lifestyle factors: excessive alcohol intake, high fat and carbohydrate diets, smoking
Lipid Profile Interpretation
Normal Values
| Parameter | Normal Value |
|---|---|
| Total Cholesterol | < 200 mg/dL |
| LDL | < 100 mg/dL |
| HDL | > 40 mg/dL (men), > 50 mg/dL (women) |
| Triglycerides | < 150 mg/dL |
ASCVD Risk Factors
Nonmodifiable
- Age (men ≥45 y; women ≥55 y)
- Male sex
- Family history of premature ASCVD
- Race/ethnicity
Modifiable
- Dyslipidemia
- Hypertension
- Diabetes mellitus
- Smoking
- Obesity/metabolic syndrome
ASCVD: Key Concept
ASCVD includes:
- Coronary artery disease
- Cerebrovascular disease; Stroke / TIA
- Peripheral arterial disease
ACC/AHA focuses on ASCVD risk, not LDL alone
Lipid-Lowering Therapies Summary
| Class | Examples | Primary Effect | Use Case | Common Side Effects |
|---|---|---|---|---|
| Statins | Atorvastatin, Rosuvastatin | ↓ LDL, ↓ TG, ↑ HDL | First-line for high CV risk | Muscle pain, liver enzyme elevation |
| Ezetimibe | Ezetimibe | ↓ LDL | Add-on to statins or statin-intolerant | GI upset, rare liver effects |
| PCSK9 Inhibitors | Evolocumab, Alirocumab | ↓↓↓ LDL | High-risk, familial hypercholesterolemia | Injection site reactions |
| Bempedoic Acid | Bempedoic acid | ↓ LDL | Statin-intolerant patients | Hyperuricemia, tendon rupture |
| Fibrates | Fenofibrate, Gemfibrozil | ↓ TG, ↑ HDL | Severe hypertriglyceridemia | Myopathy (esp. with statins), GI upset |
| Omega-3 Fatty Acids | Icosapent ethyl (Rx fish oil) | ↓ TG | High triglycerides, CV risk reduction | GI upset, bleeding risk |
| Niacin | Niacin | ↓ LDL, ↓ TG, ↑ HDL | Rarely used now due to side effects | Flushing, liver toxicity |
Statins: Mechanism of Action
- Inhibit HMG-CoA reductase (Hydroxy Methyl Glutaryl-CoA reductase) → ↓ cholesterol synthesis in liver
- Liver compensates by ↑ LDL receptor expression → ↑ LDL clearance from blood
- Result: ↓ LDL (primary), modest ↓ TG, slight ↑ HDL
Side Effects & Management
- Muscle pain/myopathy → check CK, reduce dose, switch statin, or try alternate-day dosing
- Rhabdomyolysis (rare) → stop statin, hospitalize, hydrate
- Elevated liver enzymes → monitor AST/ALT, stop or reduce dose if >3× ULN
- GI upset → take with food, at night
- Drug interactions
Statin Intensity Categories
High-Intensity (↓ LDL ≥50%)
- Atorvastatin 40–80 mg
- Rosuvastatin 20–40 mg
Moderate-Intensity (↓ LDL 30–49%)
- Atorvastatin 10–20 mg
- Rosuvastatin 5–10 mg
- Simvastatin 20–40 mg
Management According to ACC/AHA Guidelines
Initial Evaluation (All Patients)
A. Fasting or Non-fasting Lipid Panel
- Total cholesterol
- LDL-C
- HDL-C
- Triglycerides
B. Identify Secondary Causes, Review Medications
C. Assess ASCVD Risk
- Use Pooled Cohort Equations (age 40-75)
- 10-year ASCVD risk categories:
- Low: <5%
- Borderline: 5-7.4%
- Intermediate: 7.5-19.9%
- High: ≥20%
Lifestyle Measures (All Patients)
- Heart-healthy diet (Mediterranean/DASH; Dietary Approaches to Stop Hypertension)
- Weight reduction
- Physical activity (≥150 min/week)
- Smoking cessation
- Limit alcohol
Statin Benefit Groups (ACC/AHA)
Statins recommended for 4 major groups:
- Clinical ASCVD
- LDL ≥ 190 mg/dL
- Diabetes (age 40–75)
- High ASCVD risk (≥7.5%)
Clinical ASCVD Management
Includes:
- Prior MI, stroke/TIA
- PAD
- Coronary or arterial revascularization
Management:
- High-intensity statin:
- Atorvastatin 40–80 mg
- Rosuvastatin 20–40 mg
Goals:
- ≥50% LDL-C reduction
- LDL-C <70 mg/dL (practical target)
If LDL ≥70 despite max statin:
- Add ezetimibe
- If still ≥70 → PCSK9 inhibitor
Severe Hypercholesterolemia Management
LDL-C ≥190 mg/dL (age 20–75)
Initial Management:
- High-intensity statin (no risk calculation needed)
If LDL ≥100:
- Add ezetimibe
- Consider PCSK9 inhibitor (esp. familial hypercholesterolemia)
Diabetes Mellitus Management (Age 40–75, LDL ≥70)
Management:
- Moderate-intensity statin (minimum)
- High-intensity statin if:
- Age 50–75
- Multiple ASCVD risk factors
Primary Prevention (No ASCVD, No DM, LDL 70-189)
Based on 10-year ASCVD Risk:
- Borderline (5-7.4%): Consider statin if risk enhancers present
- Intermediate (7.5-19.9%): Moderate-intensity statin
- High (≥20%): High-intensity statin
Risk-Enhancing Factors (Help Decide Statin Use)
- Family history of premature ASCVD
- LDL ≥ 160 mg/dL
- Metabolic syndrome
- CKD
- Chronic inflammatory diseases
- South Asian ethnicity
- Elevated TG ≥ 175 mg/dL
- hs-CRP ≥ 2 mg/L
- Lp(a), ApoB elevation
Hypertriglyceridemia Management
TG <5.6 mmol/L (150-499 mg/dL)
- Statins first-line for ASCVD risk reduction
- Consider icosapent ethyl (EPA) in high-risk patients on statins
- Fibrates not routine
TG ≥5.6 mmol/L (≥500 mg/dL)
- Goal: prevent pancreatitis
- Fibrate first-line
- Add omega-3 fatty acids
- Statin if ASCVD risk present
TG ≥11.3 mmol/L (≥1000 mg/dL)
- Very high pancreatitis risk
- Very low-fat diet, strict glucose control
- Hospitalize if symptomatic
General Management Flowchart
Patient with Dyslipidemia
↓
Fasting Lipid Profile
↓
Rule out Secondary Causes (DM, Hypothyroidism, CKD, Drugs)
↓
Lifestyle Modification (ALL PATIENTS)
↓
Assess ASCVD Risk / Statin Benefit Group
↓
Start Statin Therapy (if indicated)
↓
Reassess Lipids after 4-12 weeks
↓
Target Achieved?
↙ ↘
YES NO
↓ ↓
Continue ↑ Statin Intensity or Add Ezetimibe
Statin ↓
Consider PCSK9 inhibitor (very high risk)
ACC/AHA-Based Statin Decision Algorithm
Does patient have Clinical ASCVD?
↓
YES → High-intensity statin
↓
NO
↓
Is LDL ≥190 mg/dL?
↓
YES → High-intensity statin
↓
NO
↓
Is patient diabetic (Age 40–75)?
↓
YES → Moderate / High-intensity statin
↓
NO
↓
Calculate 10-year ASCVD risk
↓
Risk ≥7.5% → Moderate / High-intensity statin
Risk <7.5% → Lifestyle modification
Hypertriglyceridemia Management Summary
Triglycerides Level
↓
<150 mg/dL → Normal
150–499 mg/dL → Lifestyle + Statin (if ASCVD risk)
≥500 mg/dL → Fibrate ± Omega-3
↓
Prevent Acute Pancreatitis
Clinical Scenarios
Scenario 1
Patient: 62-year-old male, history of MI 2 years ago
Lipid profile:
- Total cholesterol: 220 mg/dL
- LDL-C: 150 mg/dL
- HDL-C: 35 mg/dL
- TG: 150 mg/dL
Diagnosis: Dyslipidemia (elevated LDL-C, low HDL-C) with established Clinical ASCVD (prior MI).
Treatment:
- High-intensity statin: Atorvastatin 40–80 mg or Rosuvastatin 20–40 mg
- Target: LDL-C <70 mg/dL and ≥50% reduction from baseline
- If LDL-C ≥70 on maximally tolerated statin: Add ezetimibe
- If still ≥70: Consider PCSK9 inhibitor (evolocumab/alirocumab)
Scenario 2
Patient: 35-year-old female, no ASCVD, family history of premature CAD
Lipid profile:
- Total cholesterol: 330 mg/dL
- LDL-C: 250 mg/dL
- HDL-C: 40 mg/dL
- TG: 150 mg/dL
Diagnosis: Severe Hypercholesterolemia (LDL-C ≥190 mg/dL), consistent with Familial Hypercholesterolemia (Fredrickson Type IIa) given age and family history.
Treatment:
- High-intensity statin immediately (no risk calculation required)
- If LDL-C remains ≥100 mg/dL: Add ezetimibe
- Consider PCSK9 inhibitor if targets not achieved or confirmed FH
- Cascade screening of first-degree relatives
Scenario 3
Patient: 50-year-old male, type 2 diabetes, no ASCVD
Lipid profile:
- Total cholesterol: 210 mg/dL
- LDL-C: 130 mg/dL
- HDL-C: 38 mg/dL
- TG: 180 mg/dL
Diagnosis: Diabetic Dyslipidemia (elevated LDL-C, low HDL-C, borderline high TG) in Type 2 Diabetes.
Treatment:
- High-intensity statin (indicated for age 50–75 with diabetes plus additional risk factors: HDL 38 mg/dL, TG 180 mg/dL suggest metabolic syndrome components)
- Alternative: Moderate-intensity statin if no multiple risk factors
- Optimize glycemic control; reassess lipids in 4–12 weeks
Scenario 4
Patient: 45-year-old female, no ASCVD, non-diabetic, borderline 10-year ASCVD risk 7%
Lipid profile:
- Total cholesterol: 210 mg/dL
- LDL-C: 140 mg/dL
- HDL-C: 50 mg/dL
- TG: 150 mg/dL
Diagnosis: Borderline ASCVD Risk (7%) Dyslipidemia.
Treatment:
- Decision based on risk-enhancing factors:
- If present (e.g., family history of premature ASCVD, metabolic syndrome, LDL ≥160, CKD, high Lp[a]): Moderate-intensity statin
- If absent: Intensive lifestyle modification for 3–6 months (Mediterranean/DASH diet, exercise, weight management); reassess risk and consider coronary artery calcium (CAC) scoring if decision remains uncertain
Scenario 5
Patient: 40-year-old male, presents for routine check-up, BMI 32
Lipid profile:
- Total cholesterol: 250 mg/dL
- LDL-C: 120 mg/dL
- HDL-C: 35 mg/dL
- TG: 800 mg/dL
Diagnosis: Severe Hypertriglyceridemia (TG 800 mg/dL [≥500 mg/dL threshold]), likely secondary to obesity/metabolic syndrome (BMI 32).
Treatment:
- Priority: Prevent acute pancreatitis
- Fibrate (fenofibrate) first-line
- Add prescription omega-3 fatty acids (icosapent ethyl)
- Very low-fat diet (<15% of calories from fat), strict weight reduction, alcohol abstinence
- Evaluate for secondary causes (diabetes, hypothyroidism, renal disease, medications)
- Once TG <500 mg/dL, add statin for ASCVD risk reduction if indicated
Summary
- Dyslipidemia is a major, modifiable cause of ASCVD
- LDL-C is the primary treatment target
- Statins are first-line therapy
- Lifestyle modification is essential for everyone
- Risk stratification guides therapy
- Add non-statins when needed
- Triglycerides matter → pancreatitis risk
- Treat secondary causes first