CLINICAL APPROACH UNCONSCIOUS PATIENT
Dr. M. Sofi MD; FRCP (London); FRCPEdin; FRCSEdin
Lina Serhan
NEUROLOGICAL ASSESSMENT: COMA
Consciousness:
A state of awareness of self and the environment. This state is determined by two separate functions:
a) Awareness (content of consciousness).
b) Arousal (level of consciousness)
Coma: is a deep state of prolonged unconsciousness which a person cannot be awakened; fails to respond normally to painful stimuli, light, or sound; lacks a normal wake-sleep cycle; and does not initiate voluntary actions.
Coma is caused by disordered arousal rather than impairment of the content of consciousness.
Arousal depends on an intact:
a) ascending reticular activating system
b) connections with diencephalic structures
Coma is caused by:
- Diffuse bilateral hemisphere damage.
- Failure of the ascending reticular activating system, or both.
Sites and causes of coma
Diffuse hemisphere e.g. trauma ischaemia hypoglycaemia/other metabolic disorders infection drugs

Bilateral thalamic e.g. haemorrhage infarction Brain stem compression e.g. supra or infra tentorial mass lesions Brain stem e.g. ischaemia haemorrhage drugs
ASCENDING RETICULAR ACTIVATION SYSTEM
The ARAS functions:
- To arouse the cerebral cortex
- To awaken the brain to a conscious level
- Maintain the state of alertness, attention, wakefulness emotional reactions
- Prepare the cortex to receive the rostrally projecting impulses from any sensory modality.
- Decreased activity of the ARAS is associated with sleep.
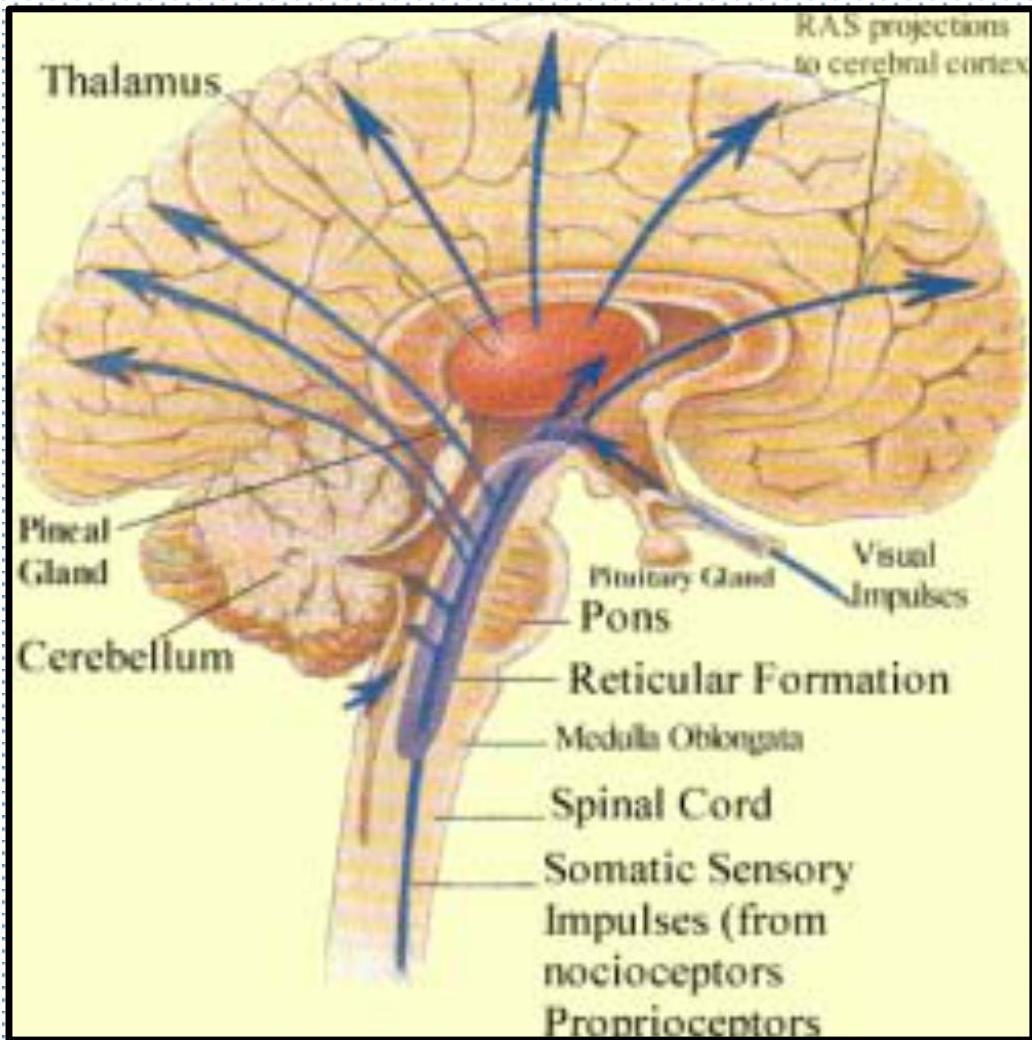
Ascending reticular activating system
Coma and related states, definitions
Consciousness: state of awareness of self and environment
Coma: the patient is unconscious, unaware, and unresponsive to external stimuli
Alertness: An alert patient is fully conscious and aware of their environment
Confusion: inability to think with customary speed, clarity, and coherence.
Lethargy: difficult to maintain the arousal state
Obtundation: A dulled or reduced level of alertness or consciousness.
Stupor: An excessively deep state of unresponsiveness. Can be aroused from it only briefly by vigorous stimulation, such as repeated shaking, loud calling, or pinching.
Delirium: It is characterized by an alteration of attention, consciousness, and cognition, with a reduced ability to focus, sustain or shift attention.
THE ABCDE APPROCH TO
| A | AIRWAYS |
|---|---|
| B | BREATHING |
| C | CIRCULATION |
| D | DRUGS/DISABILITY |
| E | EXPOSURE |
CLINICAL ASSESSMENT OF COMA
Coma is life threatening situation and evaluation must be swift, and include:
Resuscitation of CVS and respiratory system.
- ABCD
- Correction of blood glucose and thiamine
- Control of seizure
- Temperature
- Specific treatments — naloxone.
Assessment now should comprise:
- History — through friend, family or emergency medical personnel
- General physical examination
- Neurological assessment — to define the nature of coma
Coma: Initial assessment and evaluation
I. Assess level of coma: response to vocal and painful stimuli; this is known as Grady coma scale.
II. Make sure the patient is in an actual comatose state and or is not in:
- locked-in state (patient is able to move their eyes or blink)
- psychogenic unresponsiveness
III. Assess the severity of the coma with the Glasgow coma scale
IV. Take bloods:
- Drug screen
- “serum glucose, Na+, Ca+, K+, Mg+, PO₄, urea, and creatinine”
V. Perform CT or MRI scans
VI. Monitoring
- ECG – Cardiac arrhythmia
- EEG – Seizures control
Coma Differential Diagnosis
| Table 1. Mnemonic For Differential Diagnosis Of Altered Level Of Consciousness^{7} | |
|---|---|
| “MOVESTUPID” | |
| Metabolic | Metabolic: inborn errors of metabolism (eg, urea cycle defects, propionic acidemia) |
| Hypoxic | Oxygen insufficiency: hypoxemia of cardiopulmonary etiology, hypercarbia, carbon monoxide poisoning |
| Vascular | Vascular/cardiac causes: cerebrovascular accident, vasculitis (including myocardial infarction), ventriculoperitoneal shunt malfunction |
| Endocrine | Endocrine/electrolytes: diabetic ketoacidosis, hypoglycemia, electrolyte abnormalities |
| Seizure | Seizures/sepsis/shock |
| Tumor | Tumor/trauma/temperature/toxins |
| Uremia | Uremia: renal failure, liver failure |
| Psychogenic | Psychiatric/porphyria |
| Infectious | Infection/intussusception |
| Drugs | Drugs/drama |
CLINICAL ASSESSMENT OF COMA
Clinical evaluation is used to categories coma into:
A. Coma without focal signs or meningism (ATOMES P)
- This is the most common form of coma and results from Anoxic-hypoxic insult, Toxic, organ failure, metabolic, endocrine, seizures, pseudocoma.
- This results from subarachnoid hemorrhage, meningitis, and meningo-encephalitis.
- C. Coma with focal signs.
- Cerebrovascular events (ischemic or hemorrhagic)
- SOL lesions (infective or non-infective, e.g. tumors)
- Trauma
Handwritten note above Coma with focal signs or meningism: “some ne it sleepless”
Handwritten note below Coma with non-ischemic or hemorrhagic: “neck Registry” and “3rd nerve palsy” with a small “3rd nerve palsy” number
| Grady Coma Scale | Respond to: | |||
|---|---|---|---|---|
| Grade | State of awareness | Calling name | Light pain | Deep pain |
| I | Confused, drowsy, lethargic, indifferent and/or uncooperative; does not lapse into sleep when left undisturbed | Yes | Yes | Yes |
| II | Stupor;may be disoriented to time, place, and person; will lapse into sleep when not disturbed; or belligerent and uncooperative | No | Yes | Yes |
| III | Deep stupor;requires strong pain to evoke movement | No | No | Yes |
| IV | Decorticate or decerbrateposturing to a deep pain stimulus | No | No | No |
| V | Does not respond to any stimuli;flaccid | No | No | No |
Assesses patient’s neurological condition
Value range 3 -15
- 3 totally comatose
- 13 Mild altered level of consciousness
- 9-12 Moderate altered conscious level
- 15 fully alert patient
Glasgow Coma Scale
| BEHAVIOR | RESPONSE | SCORE |
|---|---|---|
| Eye opening response | •Spontaneously | 4 |
| •To speech | 3 | |
| •To pain | 2 | |
| •No response | 1 | |
| Best verbal response | •Oriented to time, place, and person | 5 |
| •Confused | 4 | |
| •Inappropriate words | 3 | |
| •Incomprehensible sounds | 2 | |
| •No response | 1 | |
| Best motor response | •Obeys commands | 6 |
| •Moves to localized pain | 5 | |
| •Flexion withdrawal from pain | 4 | |
| •Abnormal flexion (decorticate) | 3 | |
| •Abnormal extension (decerebrate) | 2 | |
| •No response | 1 | |
| Total score: | • Mild. | >13 |
| • Moderate. | 9 - 12 | |
| • Severe | < 8 |
| CLINICAL ASSESSMENT OF COMA | |
|---|---|
| General examination | Neurological (general) |
| Skin: rash, anemia, jaundice | |
| (meningitis | |
| Liver failure) | Head, neck and eardrum |
| (trauma) | |
| Temperature: (fever infection | |
| hypothermia-drugs / circulatory | |
| failure) | Meningism (SAH / meningitis) |
| Blood pressure (for example, | |
| septicemia / Addison’s disease) | Fundoscopy (Papilledema / |
| subhyaloid hemorrhage) | |
| Breath (fetor hepaticus, alcohol) | |
| (Dead fish smelt | |
| Acute | |
| Liver failure) | Motor response |
| Cardiovascular (for example, | |
| arrhythmia) | Deep tendon reflexes: Biceps, |
| Triceps, Brachioradialis, Patellar | |
| Abdomen (organomegaly) | Muscle tone/Planters |
CLINICAL ASSESSMENT OF COMA
Brainstem Reflexes
| Reflex | Technique | Reflex pathways | Localization |
|---|---|---|---|
| Direct | |||
| pupillary | |||
| light | |||
| reaction | |||
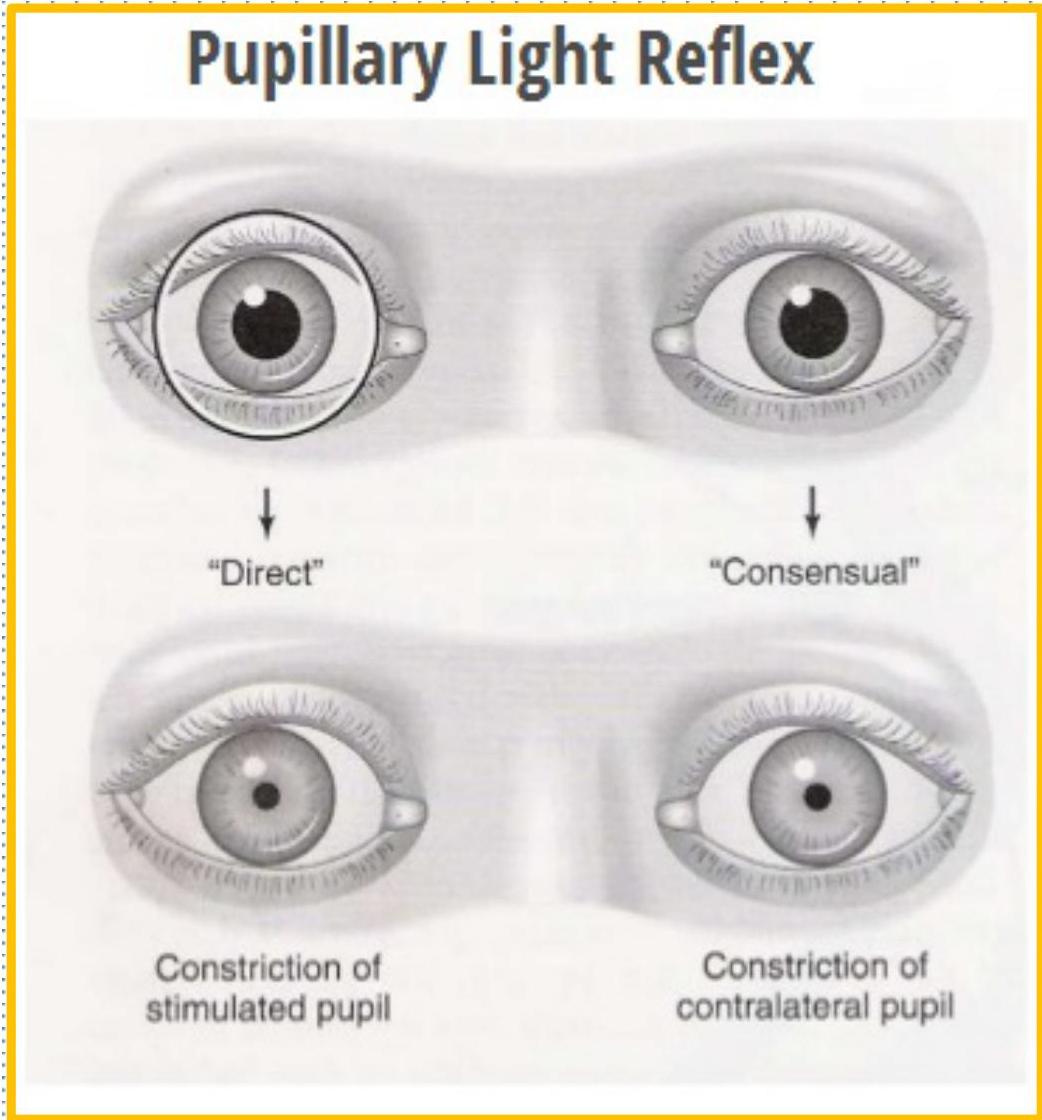
| (seen in both eyes) | The pupillary light reflex (PLR) is the constriction of the pupil that is elicited by an increase in illumination of the retina. Shine light on pupil and observe constriction. | Affluent; 2nd CN | |
| Efferent): 3rd CN | Midbrain and pontine tegmentum | ||
| Corneal response | Open lid if necessary; lightly stroke cornea with cotton wisp; observe for blink. | Affluent; 5th CN | |
| Efferent): 7th CN | Pons |
Pupillary light reflex
- Pupillary light reflex (PLR) is a reflex that controls the diameter of the pupil, in response to the intensity (luminance) of light.
- A greater intensity of light causes the pupil to constrict (miosis).
- lower intensity of light causes the pupil to dilate (mydriasis) (allowing more light in).
- The afferent limb of PLR is optic 2nd CN and efferent limb is oculomotor 3rd CN.
CORNEAL REFLEX
The corneal reflex, also known as the blink reflex or eyelid reflex, is an involuntary blinking of the eyelids elicited by stimulation of the cornea (such as by touching)

Afferent limb of the reflex being the ophthalmic division of the 5th CN, the efferent limb running in the 7th CN
OCULOCHOCKLEAR AND OCULOVESTIBULAR REFLEX
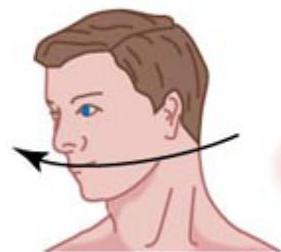
Oculocephalic response (doll’s eyes)
Reflex arc: (CN 3,6,8)
The patient’s eyes are held open. the head is briskly turned from side to side. A positive response occurs when the eyes rotate to the opposite side to the direction of head rotation. thus indicating that the brainstem (CN3,6,8) is intact.
Oculovestibular:
Reflex arc: (CN 3,6,8)
-
Hot and cold water produce currents in opposite directions and therefore a horizontal nystagmus in opposite directions in patients with an intact brainstem.
-
If the water is warm (44 °C or above) both eyes will turn toward the contralateral ear, with horizontal nystagmus (quick horizontal eye movements) to the ipsilateral ear.
-
If the water is cold, (30 °C or below). The eyes then turn toward the ipsilateral ear, with horizontal nystagmus to the contralateral ear.
In comatose patients the fast phase of nystagmus will be absent. As a result, cold water irrigation will result in deviation of the eyes toward the ear being irrigated. If both phases are absent, this suggests the patient’s brainstem reflexes are also damaged and carries a very poor prognosis.
Doll’s Eye reflex movement
“The OCR/DOLL’S EYE REFLEX” is movement of the eyes in the direction opposite that in which the head is moved. For example, the reflex is present if the eyes move to the right when the head is rotated to the left, and vice versa.
Normal (reflex present)
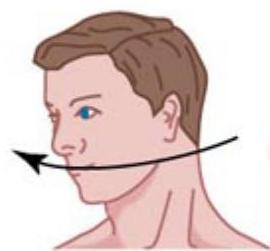 Head rotated to the right
Head rotated to the right
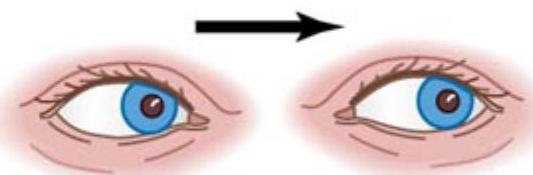 Eyes move to the left
Eyes move to the left
Abnormal (reflex absent)
 Head rotated to the right
Head rotated to the right
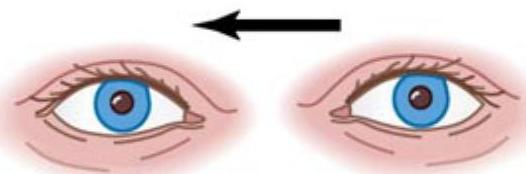 Eyes follow
Eyes follow
Abnormalities are caused by lesions of the inner ear or brainstem, especially the Pons and midbrain.
Caloric reflex test
maement of the eye and nystagmus
OCULOCULOVESTIBULA TR REFLEX:
This is a test that involves irrigating cold or warm water or air into the external auditory canal. With warm water both eyes will turn toward the contralateral ear, with quick horizontal nystagmus to the ipsilateral ear.
Absent or asymmetric implies brain stem disease.
Vestibulo-ocular Reflex
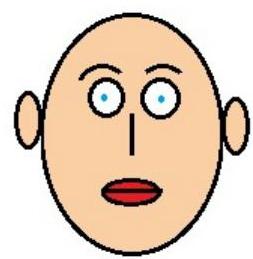
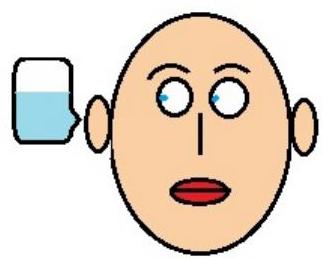
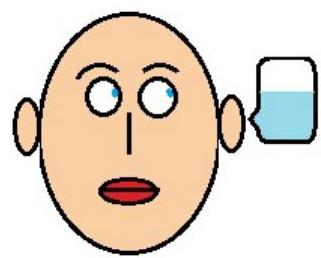
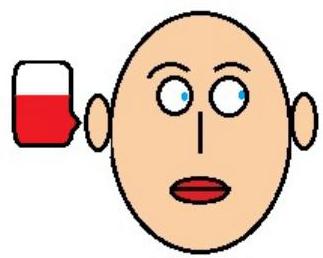
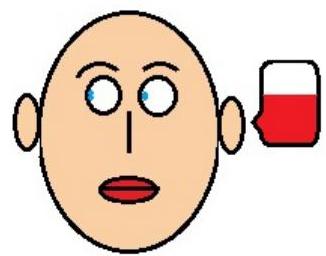
One mnemonic used to remember the FAST direction of nystagmus is COWS. COWS: Cold Opposite, Warm Same.
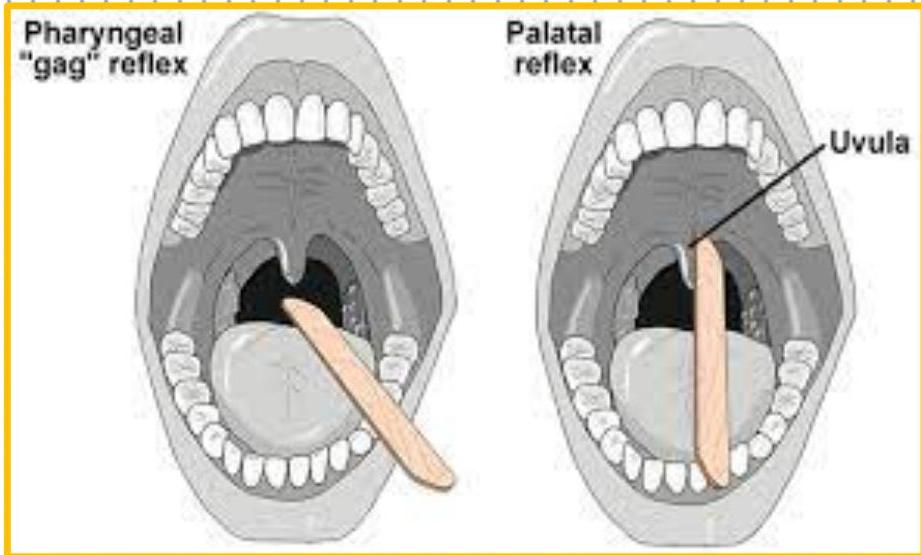
Gag reflex
Gag reflex is an integrity of IX and X nerves
Test procedure: Using a long handle swab stick gently and briskly touch the pharyngeal wall
Test findings:
- Normal gag reflex there is symmetrical elevation of the uvula or the fauces.
- A positive gag reflex will produce a non-symmetrical elevation of the uvula or the fauces.
- If on saying â¢ahhâ there is elevation of the uvula but not with the gag reflex this indicates lesion with the IX nerve.
- If there is no movement of the uvula with the gag reflex and with saying ‘ahh’ this may signify bilateral palatal muscle paralysis.
| Cheyne-Stokes respiration: diffuse forebrain damage, upper brainstem damage, metabolic encephalopathy, impending transtentorial herniation | |
|---|---|
| Biot’s Respiration: Groups of quick, shallow inspirations followed by regular or irregular periods of apnea:: CVA or trauma of medulla or lower pons, or uncal tentorial herniation | Biot respiration |
| Kussmaul Respiration: Is a deep and labored breathing pattern associated with severe metabolic acidosis, in DKA and renal failure. It is a form of hyperventilation that reduces CO2 | |
| Apneustic Respiration: Deep, gasping inspiration with a pause at full inspiration. Pontine lesions specially infarct, rarely with metabolic coma or transtentorial herniation | |
| Ataxic Respiration: Irregular breathing, with irregular pauses and increasing periods of apnea. lesion of the reticular formation of the dorsomedial part of the medulla. Poor prognosis |
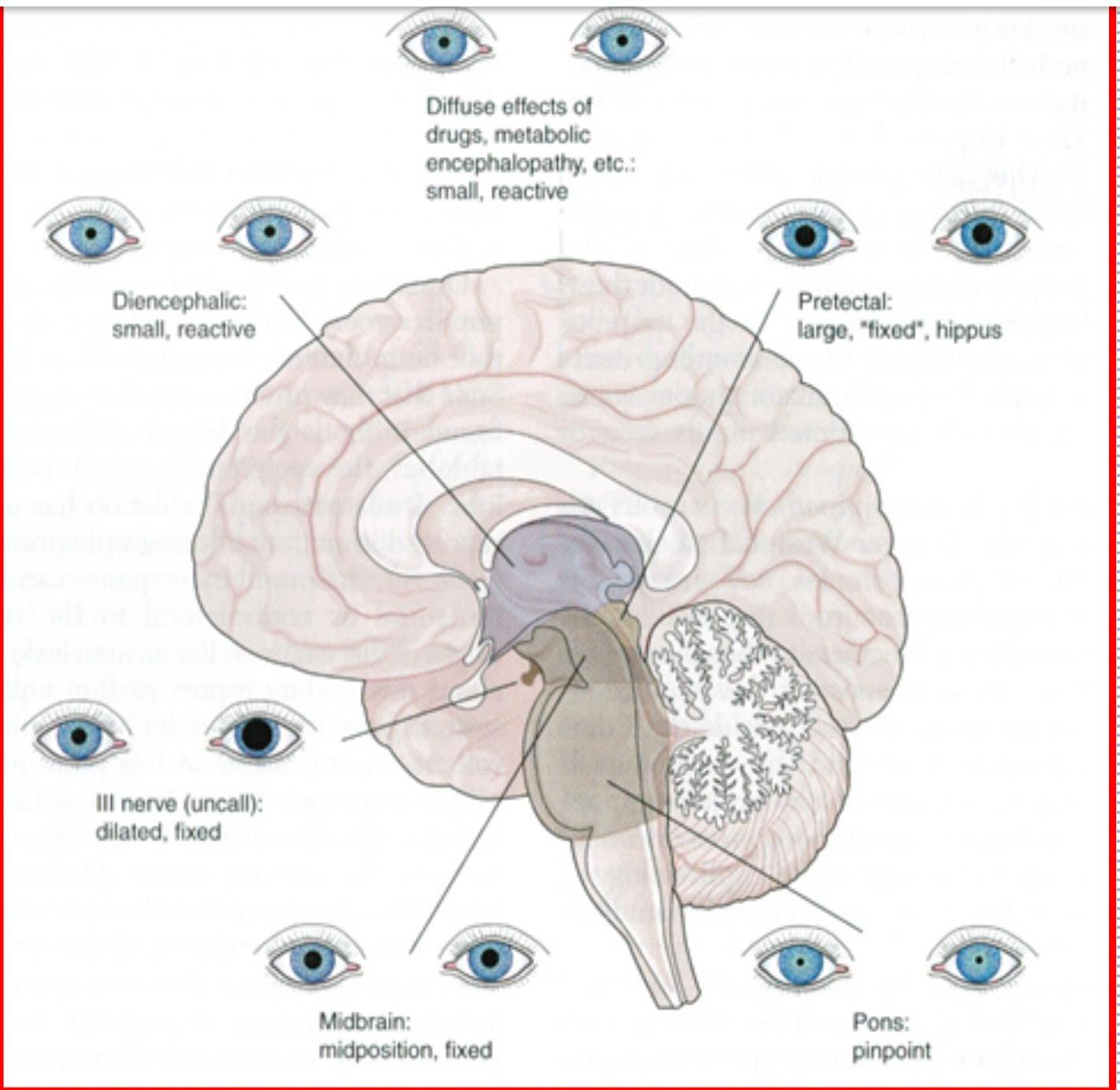
Diagnostic value of pupillary changes in coma
| Diencephalon |
|---|
| Benzodiazepine |
| Anoxic/Hypoxic |
| Atropine |
| Pontine hemorrhage |
| Morphine |
| Midbrain lesion |
| Transtentorial herniation |
| Dilated fixed pupil 3rd N palsy |
| PCOM Aeurysm |
Small reactive drugs, metabolic encephalopathies diencephalic dysfunction

Large fixed pupils- pretectal lesions

Pinpoint pupils- pontine lesions

Midposition, fixed pupils- midbrain lesions

Dilated fixed pupils- 3rd nerve lesions
Pupils: Localizing Value
Small reactive:
- Drugs
- Metabolic
- Diencephalic
Fixed dilated:
- Hypoxic ischemic encephalopathy
- Opiate withdrawal
- Barbiturate intoxication
- Atropine
- Scopolamine
- Glutethimide
Pinpoint reactive:
- Pontine hemorrhage
- Opiate overdose
- Cholinergic toxicity
Coma Mimics
- ☑ Akinetic mutism not moving but alert
- ☑ Locked-in syndrome hemorrhage in dorsal part of Pons
- Catatonia
- Conversion reaction
Akinetic Mutism
- Silent, immobile but alert appearing.
- Patients are in a wakeful state of profound apathy
- Seemingly indifferent to pain, thirst, or hunger.
- Usually due to lesion in:
- bilateral mesial frontal lobes
- bilateral thalamic lesions
- lesions in periaqueductal grey (brainstem)
Many cases of akinetic mutism have occurred after a thalamic stroke
”Locked-In’ Syndrome”
Locked-in syndrome (LIS) is a complex medical condition presenting with quadriplegia, bulbar palsy, and whole-body sensory loss due to damage in the brain stem, commonly the anterior pons.
Cognition, vertical eye movement, blinking, and hearing are classically preserved in patients suffering from the condition.
 A large pontine hematoma
A large pontine hematoma
Catatonia
Catatonia, a neuropsychiatric syndrome characterized by stupor, excitement, mutism, posturing, abnormal movements and behaviors, that is most often seen in:
- Mood disorders but can also be seen in can also be seen in
- Organic brain disease: encephalitis, toxic and drug-induced psychosis
Conversion reactions
- Fairly rare
- Oculocephalic may or may not be present
- The presence of nystagmus with cold water caloric indicates the patient is physiologically awake
- ☐ EEG used to confirm normal activity
Coma: Practice questions
-
Direct pupillary light reflex in an unconscious patient reveals? A. Small pinpoint reactive pupil in hemispheric infarction B. Nonreactive dilated pupils in pontine hemorrhage C. Large dilated pupils in morphine overdose D. Bilateral dilated nonreactive pupil in hypoxic brain insult
-
Coma is a recognized clinical manifestation in which of the following? A. Simple partial seizure B. Transient ischemic attack C. Locked in syndrome D. Non-convulsive status epilepticus
-
The features of metabolic coma include? A. Presence of focal neurological deficit B. Positive neck rigidity and Kerning’s sign C. Fixed dilated pupils to direct light reflex D. Small reactive pupils to direct light reflex
THANK YOU