Viral Haemorrhagic Fever
Dr Nada Abdelrahman Associated

Lina Serhan
Learning outcomes
- By the end of this lecture, the students should be able
- Identify the aetiology of viral hemorrhagic fevers.
- Review the appropriate evaluation of patients with viral hemorrhagic fevers.
- Describe the management of viral hemorrhagic fevers.
Definition
Viral haemorrhagic fevers (VHFs) represent a group of severe systemic febrile illnesses caused by four families of viruses
- Arenaviridae
- Bunyaviridae
- Filoviridae
- Flaviviridae
 Ebola virus
Ebola virus

- Zoonotic diseases require a vector for their transmission
Aetiology
Arenaviridae family
- Lassa virus (LASV) - Lassa fever
- Chapare virus (CHPV) - Chapare HF
- Guanarito virus (GTOV) - Venezuelan HF
- Junin virus (JUNV) - Argentine HF
- Lujo virus (LUJV) - Lujo HF
- Lymphocytic choriomeningitis virus (LCMV)
- Machupo virus (MACV) - Bolivian HF
- Sabia virus (SABV) - Brazilian HF

Bunyaviridae family
- Rift Valley fever virus (RVFV) - Rift Valley fever
- Crimean-Congo hemorrhagic virus (CCHFV)
- Dobrava-Belgrade virus (DOBV) – HF with renal syndrome
- Hantaan virus (HTNV) – HF with renal syndrome
- Puumalavirus (PUUV) – HF with renal syndrome.
- Saaremaa virus (SAAV) – HF with renal syndrome.
- Seoul virus (SEOV) – HF with renal syndrome.
- Sin Nombre virus (SNV) – Hantavirus PS
- Severe fever and thrombocytopenia syndrome virus (SFTSV)
- Tula virus (TULV) – HF with renal syndrome
Filoviridae family:
- Bundibugyo ebolavirus (BDBV) - Ebola virus disease
- Marburg marburgvirus (MARV) - Marburg HF
- Sudan ebolavirus (SUDV) - Ebola virus disease
- Taï Forest ebolavirus (TAFV) - Ebola virus disease
- Zaire ebolavirus (EBOV) - Ebola virus disease
Flaviviridae family:
- Dengue virus (DENV-1-4) - Dengue fever
- Kyasanur forest disease virus (KFDV) - Kyasanur forest disease
- Omsk hemorrhagic fever virus (OHFV) - Omsk HF
- Yellow fever virus (YFV) - Yellow fever
Epidemiology
-
Arenaviridae: rodent-borne diseases, via contact with rodent urine or droppings or aerosol transmission. Human-to-human and nosocomial infections e.g. Lassa virus, outbreaks in West Africa with case fatality rates as high as 50%
-
Bunyaviruses e.g. Rift Valley fever: transmitted via arthropods and rodents. Crimean-Congo hemorrhagic fever endemic in Africa and Asia is the most widespread tick-borne illness in humans.
-
Filoviruses e.g. Ebola virus disease detected in bats in Africa. Risk of person-to-person spread, especially in those caring for infected patients. Ebola outbreaks in the Congo, with case fatality rates as high as 80% to 90%
-
Flaviviruses e.g. Dengue transmitted via arthropods (Aedes aegypti). Endemic in over 100 countries (Africa, Americas, Asia, Australia, Europe, and the Pacific Islands with a mortality rate of 0.8% to 2.5%.
 This Photo by Unknown Author is
This Photo by Unknown Author is
 Pathophysiology
Pathophysiology
ايما الصغار
Dengue
- In the last 50 years, the incidence of dengue has increased 30-fold worldwide, including Southwestern KSA.
- Mode of transmission: bite of infective Aedes aegypti mosquito.
- Is spherical single-stranded enveloped RNA virus related to flavivirus group in the family flaviridae.
- 4 serotypes; DEN 1, DEN 2, DEN 3, DEN 4

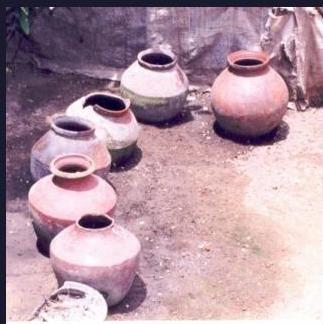


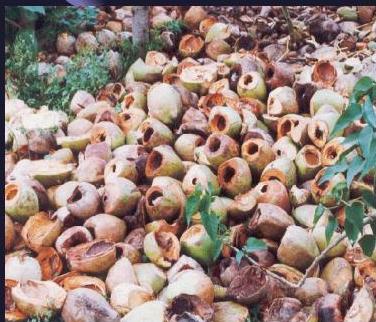


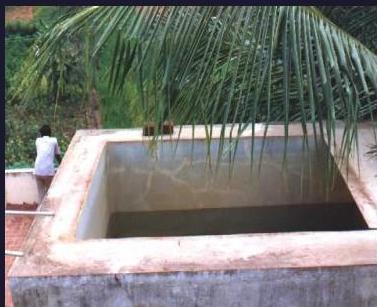
Few common and favoured breeding places/sites of
Aed aegypti

Clinical features
- thrombocytopenia + high hematocrit (always exclude dengue fever)
Abrupt onset of high fever
- Ass with myalgia, arthralgia
- “Break-bone fever”
- Severe frontal headache and retro-orbital
- Retro-orbital pain worsens with eye movement
Loss of appetite & sense of taste (metallic taste)
- Macular or maculopapular rash
- Nausea and vomiting + diarrhoea
- Respiratory symptoms: cough, sore throat
Cardiac manifestations
Neurological Manifestations
3 phases
| Course of dengue illness | FEBRILE | CRITICAL | RECOVERY |
|---|---|---|---|
| Days of illness | 1 2 3 | 4 5 | 6 7 8 9 10 |
| Temperature | 40 | start & stop | |
| Potential clinical issues | Dehydration | Shock / Bleeding | Reabsorption / Fluid overload |
| Laboratory changes | Hematocrit | Organ Impairment | Platelet ↑ |
| Serology and virology | Viraemia | IgM/IgG |
Note: Onset of defervescence usually occurs between day 3 to day 5 of illness.
Note: Quasi or quite because of death occurs between day 3 to day 5 of illness.
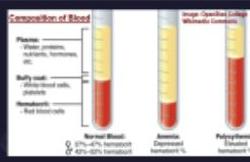
Composition of Blood
Plasma:
- Water, proteins, nutrients, hormones, etc.
Buffy coat:
- White blood cells, platelets
Hematocrit:
- Red blood cells
Inorganic Normal Blood:
- 37%–47% hematocrit
- 42%–52% hematocrit
Inorganic Anemia:
- Depressed hematocrit %
Inorganic Polycythemia:
- Elevated hematocrit %
Image: OpenStax College Wikimedia Commons
HealthyAndNaturalWorld.com
Clinical signs
hemorrhagic manifestation everywhere





Clinical spectrum of Dengue
Dengue case classification and levels of severity (WHO 2009 [2])
| Dengue ± warning signs | Warning signs | Severe dengue: One or more of the following |
|---|---|---|
| Probable dengue | ||
| ✓ Live in/travel to dengue-endemic area | Abdominal pain or tenderness | |
| ✓ Persistent vomiting | ||
| ✓ Clinical fluid accumulation | ||
| ✓ Mucosal bleed | ||
| ✓ Lethargy, restlessness | ||
| ✓ Liver enlargement > 2 cm | Severe plasma leakage | |
| leading to: | ||
| • Shock (DSS) | ||
| • Fluid accumulation with respiratory distress | ||
| Severe bleeding | ||
| Severe organ involvement | ||
| • Liver: AST or ALT ≥ 1000 | ||
| • CNS: Impaired consciousness | ||
| • Heart and other organs | ||
| Fever and 2 of the following criteria: | ||
| • Nausea, vomiting | ||
| • Rash | ||
| • Aches and pains | ||
| • Tourniquet test positive | ||
| • Leukopenia | Laboratory: Increase in hematocrit (HCT) concurrent with rapid decrease in platelet count |
DSS Dengue shock syndrome
Expanded Dengue Syndrome (EDS)
World Health Organization classification of cases:

Grade 1: Fever and nonspecific constitutional symptoms. Positive tourniquet test is only hemorrhagic manifestation
Grade 2: Grade 1 manifestations + spontaneous bleeding
Grade 3: Signs of circulatory failure (rapid/weak pulse, narrow pulse pressure, hypotension, cold/clammy skin)
Grade 4: Profound shock (undetectable pulse and BP)
Differential Diagnosis
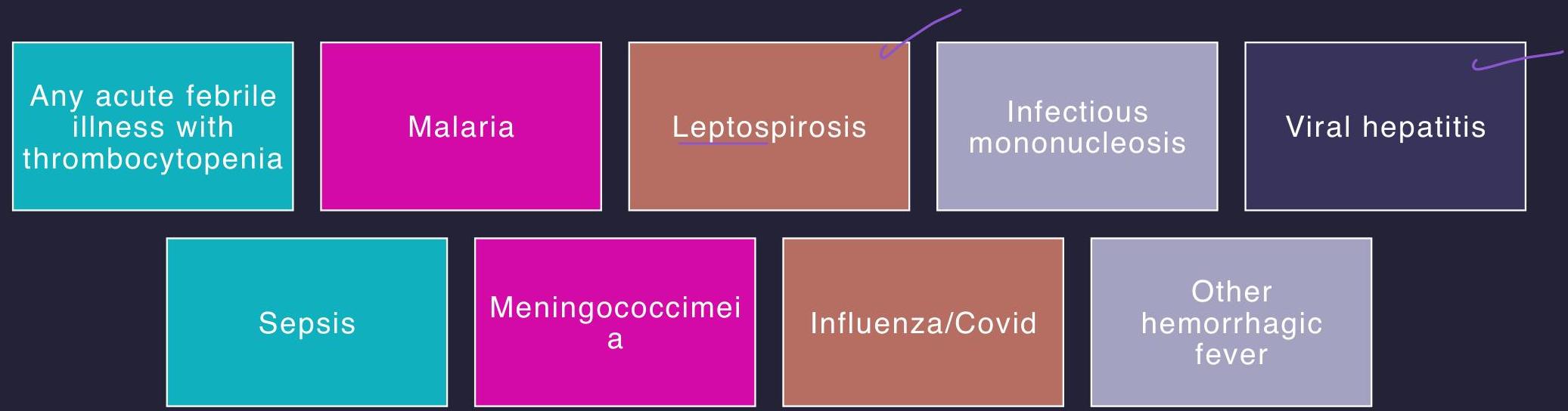
Laboratory evaluation
- Complete blood count with differential
- Coagulation studies
- Liver function tests & Renal function test
- Urinalysis, urine culture
- Chest x-ray
- should be natural
- Blood cultures
- Dengue-specific tests: NS1Ag
- Serology: IgM capture ELISA, RT-PCR
Remember
Four Criteria for DHF:
- Fever
- Hemorrhagic manifestations
- Excessive capillary permeability
- ≤ 100,000/mm³ platelets
Initial Warning Signals:
- Disappearance of fever
- Drop in platelets
- Increase in hematocrit
Alarm Signals:
- Severe abdominal pain
- Prolonged vomiting
- Abrupt change from fever to hypothermia
- Change in level of consciousness (irritability or somnolence)
When Patients Develop DSS:
- 3 to 6 days after onset of symptoms
Treatment of Dengue Fever
There is no specific antiviral treatment
Management is essentially supportive and symptomatic
Rest, Fluids and Antipyretics
Outline of current management protocol
☐ Group A: Home danger signs Oral fluids, paracetamol (avoid NSAIDs), explain Gastric ulceration bleeding
Clinical and laboratory parameter monitoring
☐ Group B without warning signs: Oral fluids; if not tolerated, IV fluids for 24–48 h (0.9% saline or Ringer lactate).
☐ Group B with warning signs: Baseline HCT, isotonic fluids till able to take orally adequately. Increase or decrease fluid rate based on serial HCT. profond shouck
☐ Group C: Judicious fluid resuscitation, treatment of bleeding manifestations, glycemic control and discontinue intravenous fluids once hemodynamics stabilize. sometimes need ionotrapes
Prevention
- The best preventive measure is vector control
- Personal protection against mosquito biting
- Screening doors and windows
- Protective clothing
- Application of mosquito repellents on exposed skin
- A vaccine for Dengue (Dengvaxia) (CYD-TDV) live, recombinant vaccine uses the yellow fever virus genome as a backbone for the dengue virus’s envelope and pre-membrane gene sequence.


Isolation precautions should be instituted immediately if this entity is suspected category A bioweapons agents as they are stable when aerosolized and are associated with severe morbidity and mortality in infected individuals..
Prognosis
- Dramatic clinical response to aggressive fluids and electrolytes.
- Convalescence may be prolonged, with weakness and mental depression
- Survival is related directly to early hospitalization and aggressive supportive care
- Treated DHF is associated with a 3% mortality rate
- Un-treated DHF is associated with a 50% mortality rate. Causes of death include EDS multi-organ failure, hemorrhagic complications, and circulatory collapse.
- A 51-year-old woman presented with myalgias, fever, and a petechial rash for the past two days. She recently returned from a ten-day trip to West Africa. She states she had similar symptoms three years ago, resolved with supportive care at home. The patient’s temperature is 39.4 °C, Pulse is 100/min, RR17/min, and BP 90/50 mmHg. She has petechial lesions over the distal right arm after a BP measurement is obtained using a sphygmomanometer. Initial laboratory workup is shown below. Which of the following is the most likely diagnosis? Positive for frequent test
A. Dengue hemorrhagic fever B. Ebola C. Parvovirus B19 D. COVID-19 E. Typhoid fever
| Laboratory value | |
|---|---|
| Serum chemistries | Result |
| Hemoglobin | 9.8 g/dL |
| Hematocrit | 30 % |
| Leukocyte count | 2000 /mm3 |
| Platelet count | 50,000 /mm3 |
| AST | 170 U/L (5 to 40) |
| ALT | 200 U/L (7 to 56) |
| Serum creatinine | 1.4 mg/dL |
ДЕМЕНТАЛЬНА БАЛКЛОЯ
