PEDIATRIC NEUROLOGICAL EXAM
Dr Faten Zaidan
Kindly review neurological chapter of Dr Mansour AlHowasi
COMPONENTS OF PEDIATRIC NEUROLOGICAL EXAMINATION
- Cognitive/mental status through GCS
- Motor and sensory: power tone and reflexes
- Cranial nerve examination
- Cerebellar exam
In the exam, you will be asked to either examine the cranial nerves specifically or general neurological examination including power, tone, reflexes and gait.
Steps:
- GCS or AVPU
- Motor function
- Sensory function
- Cerebellum
- Cranial Nerve
INSPECTION AND MENTAL STATUS
- Take 1 minute to inspect your patient while playing, talking, and interacting with the parents.
- Take notes on any abnormal behavior, eye contact or abnormal posture of the body. See how patient is playing and interpreting the surroundings.
- In children who are less than 7 years old, you will assess the developmental milestones.
- In neonates, you will assess the primitive reflexes.
- In children above 7 years old, you will do mini-mental status exam.
Mini-Mental State Examination (MMSE)
Patient’s Name: _____________________________
Date: _____________________________
Instructions: Ask the questions in the order listed. Score one point for each correct response within each question or activity.
| Maximum Score | Patient’s Score | Questions |
|---|---|---|
| 5 | ”What is the year? Season? Date? Day of the week? Month?“ | |
| 5 | ”Where are we now: State? County? Town/city? Hospital? Floor?“ | |
| 3 | The examiner names three unrelated objects clearly and slowly, then asks the patient to name all three of them. The patient’s response is used for scoring. The examiner repeats them until patient learns all of them, if possible. Number of trials: __________ | |
| 5 | ”I would like you to count backward from 100 by sevens.” (93, 86, 79, 72, 65, …) Stop after five answers. Alternative: “Spell WORLD backwards.” (D-L-R-O-W) | |
| 3 | ”Earlier I told you the names of three things. Can you tell me what those were?“ | |
| 2 | Show the patient two simple objects, such as a wristwatch and a pencil, and ask the patient to name them. | |
| 1 | ”Repeat the phrase: ‘No ifs, ands, or buts.‘“ | |
| 3 | ”Take the paper in your right hand, fold it in half, and put it on the floor.” (The examiner gives the patient a piece of blank paper.) | |
| 1 | ”Please read this and do what it says.” (Written instruction is “Close your eyes.”) | |
| 1 | ”Make up and write a sentence about anything.” (This sentence must contain a noun and a verb.) | |
| 1 | ”Please copy this picture.” (The examiner gives the patient a blank piece of paper and asks him/her to draw the symbol below. All 10 angles must be present and two must intersect.) | |
| 30 | TOTAL |
CONSCIOUS LEVEL (GCS & AVPU)
Pediatric Glasgow Coma Scale (PGCS)
| >1 Year | < 1 Year | Score | ||
|---|---|---|---|---|
| EYE OPENING | Spontaneously | Spontaneously | 4 | |
| To verbal command | To shout | 3 | ||
| To pain | To pain | 2 | ||
| No response | No response | 1 | ||
| MOTOR RESPONSE | Obeys | Spontaneous | 6 | |
| Localizes pain | Localizes pain | 5 | ||
| Flexion-withdrawal | Flexion-withdrawal | 4 | ||
| Flexion-abnormal (decorticate rigidity) | Flexion-abnormal (decorticate rigidity) | 3 | ||
| Extension (decerebrate rigidity) | Extension (decerebrate rigidity) | 2 | ||
| No response | No response | 1 | ||
| >5 Years | 2-5 Years | 0-23 months | ||
| VERBAL RESPONSE | Oriented | Appropriate words/phrases | Smiles/coos appropriately | 5 |
| Disoriented/confused | Inappropriate words | Cries and is consolable | 4 | |
| Inappropriate words | Persistent cries and screams | Persistent inappropriate crying and/or screaming | 3 | |
| Incomprehensible sounds | Grunts | Grunts, agitated, and restless | 2 | |
| No response | No response | No response | 1 | |
| TOTAL PEDIATRIC GLASGOW COMA SCORE (3-15): |
Glasgow Coma Scale Breakdown
△ Eye opening
- Spontaneous - 4
- To speech - 3
- To pain - 2
- None - 1

△ Verbal response
- Oriented - 5
- Confused - 4
- Inappropriate words - 3
- Incomprehensible words - 2
- None - 1

△ Motor response
- Obeys commands - 6
- Localises pain - 5
- Flexion to pain - 4
- Abnormal flexion - 3
- Extension to pain - 2
- None - 1

Interpretation:
- Total score: 15
- Mild head injury: 13-15
- Moderate head injury: 9-12
- Severe head injury: < 8 (3-8)
med_life_easy
AVPU Scale
Levels of Consciousness
- A - Alert
- V - Verbal Stimuli (Verbally responsive)
- P - Painful Stimuli (Physically responsive)
- U - Unresponsive
- Awake
- Verbally responsive
- Physically responsive
- Unresponsive
Note: Rapid assessment but Rough method, not suitable for long follow up.
Correlation with the GCS:
- A = GCS 15
- V = GCS 12-13
- P = GCS 5-6
- U = GCS 3
CRANIAL NERVE EXAMINATION
- Examination of cranial nerves should be done to complete any neurological examination done to the patient. However, in case of OSCE, because of shortness of time, you will be asked to do solely cranial nerves. Kindly see the following slides which will show you the function of every cranial nerve and how it is examined.
- In OSCE, if you were asked to do general neurological examination, you must comment at the end “I will complete my neurological examination by doing the cranial nerve examination”.
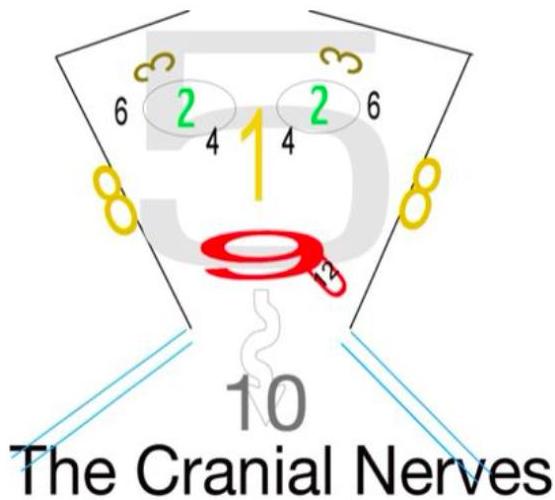
Origin of Cranial Nerves
- Cortex: CN 1, CN 2
- Midbrain (Brainstem): CN 3, CN 4
- Pons (Brainstem): CN 5 – CN 8
- Medulla (Brainstem): CN 9 – CN 12
CN I: Olfactory Nerve
- Function: Sense of smell.
- This is tested for specific cases.
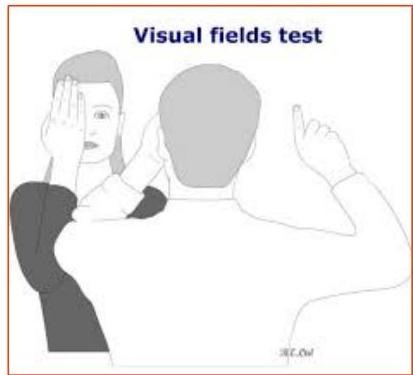
CN II: Optic Nerve
- You examine the visual acuity by using Snellen chart.
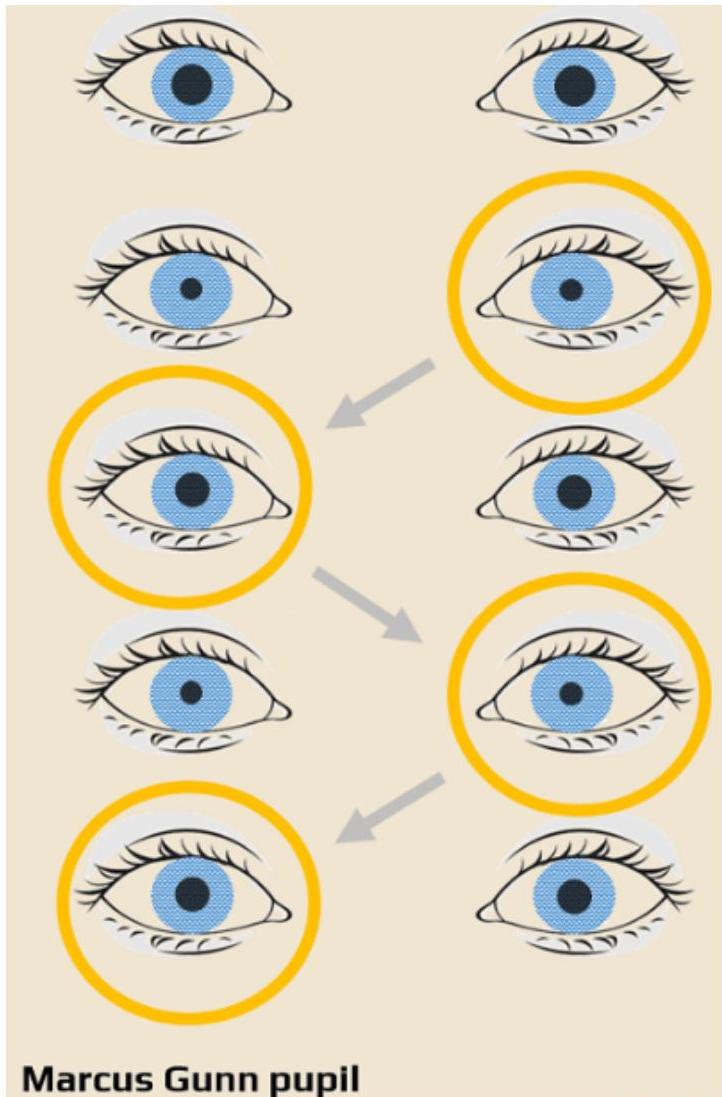
- You will examine also the pupils reaction to light through swinging flashlight test.
- Fundoscopy.
| E | 1 | 20/200 |
|---|---|---|
| FP | 2 | 20/100 |
| TOZ | 3 | 20/70 |
| LPED | 4 | 20/50 |
| PEC FD | 5 | 20/40 |
| EDF C Z P | 6 | 20/30 |
| F E L O P Z D | 7 | 20/25 |
| D E F P O T E C | 8 | 20/20 |
| L E F O D P C T | 9 | |
| F D P L T C E O | 10 | |
| P E R O L C F T D | 11 |
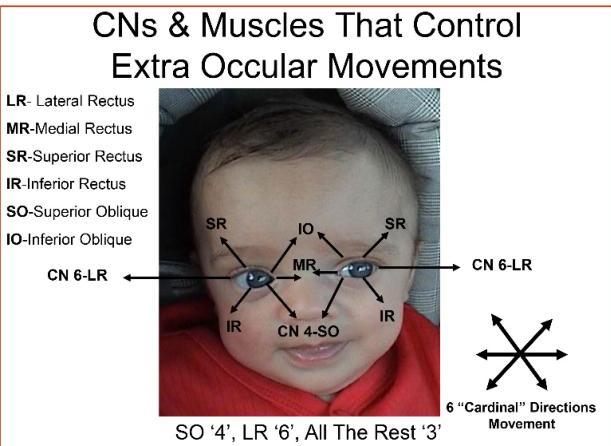
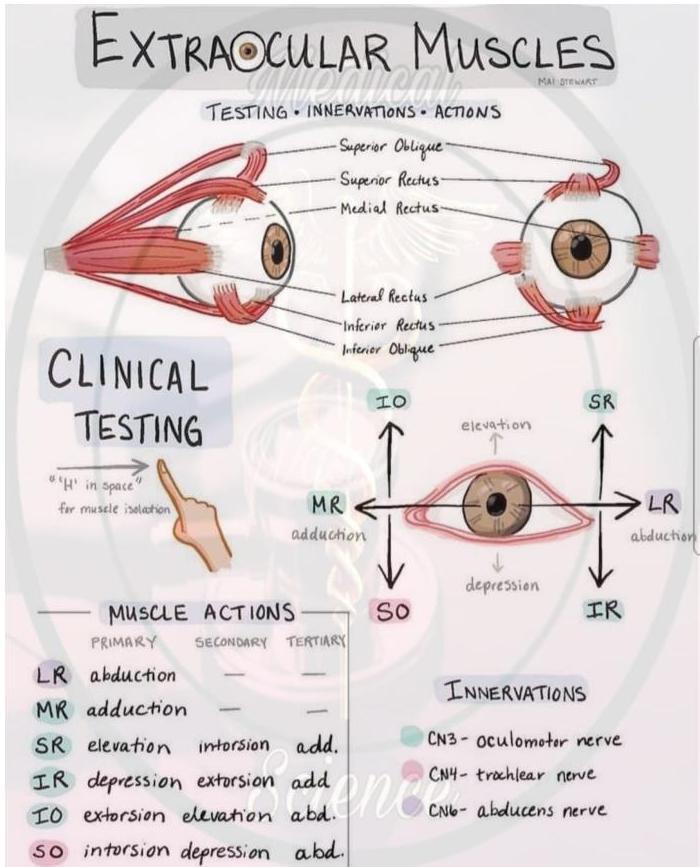
CN III, IV, VI: Oculomotor, Trochlear, Abducens
Examination
- You will examine two things: eyelid and all visual fields (shape of letter H).
- CN III (Oculomotor): all other extraocular movements.
- CN IV (Trochlear): controls superior oblique: pulls eye down and in.
- CN VI (Abducens): controls lateral rectus: abducts the eye.
- When you want to test the right eye, you must cover your left eye and vice versa.
Mnemonic: Extraocular Muscles
LR6-SO4-R3
- Lateral Rectus is 6th CN
- Superior Oblique is 4th CN
- Rest are all 3rd CN
Cranial Nerve Palsy & Findings
Evidence of incomitance
Right 3rd Nerve Palsy
- Down and out, with associated ptosis.


- Direction of gaze: Smaller angle of horizontal squint.
- Findings: No obvious squint / Unable to adduct right eye / Larger angle of squint / Double vision further apart.
Right 4th Nerve Palsy
- Up and out, with vertical diplopia.



- Primary position: Right eye turns downwards and outwards / Right eye turns upwards and outwards.
- Direction of gaze: Unable to adduct right eye / Larger angle of squint / Double vision further apart.
Right 6th Nerve Palsy
- Inward, inability to move the eye outward (Nonspecific sign of increased ICP).



- Right eye elevates more as it moves medially / Double vision further apart / Right eye turns medially.
- Able to adduct right eye / No obvious squint.
Specific Notes
- Marcus Gunn Pupil: afferent pupillary defect.
- Horner Syndrome: sympathetic innervation of pupil.
- Figure 5. Case 2 showing miosis prior to apraclonodine hydrochloride. 0.5% testing.

- Figure 5. Case 2 showing miosis prior to apraclonodine hydrochloride. 0.5% testing.
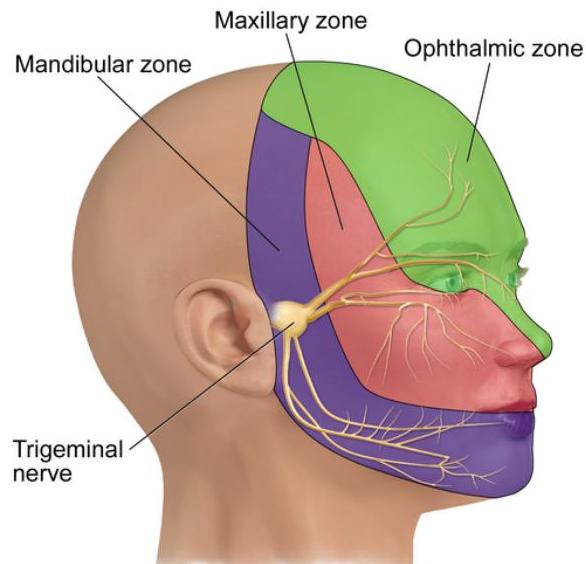
CN V: Trigeminal Nerve
- Trigeminal nerve has three main branches: ophthalmic, maxillary and mandibular.
- Functions: facial sensation, corneal sensation, muscles of mastication.
 Trigeminal nerve
Trigeminal nerve
| Branch | Motor | Sensory |
|---|---|---|
| Ophthalmic | • Light touch using cotton • Corneal reflex | |
| Maxillary | ||
| Mandibular | Motor component – supplies the muscles of mastication. i. Ask the child to open their mouth, whilst you try to close it. It will deviate to the side of weakness. ii. Clench teeth. |
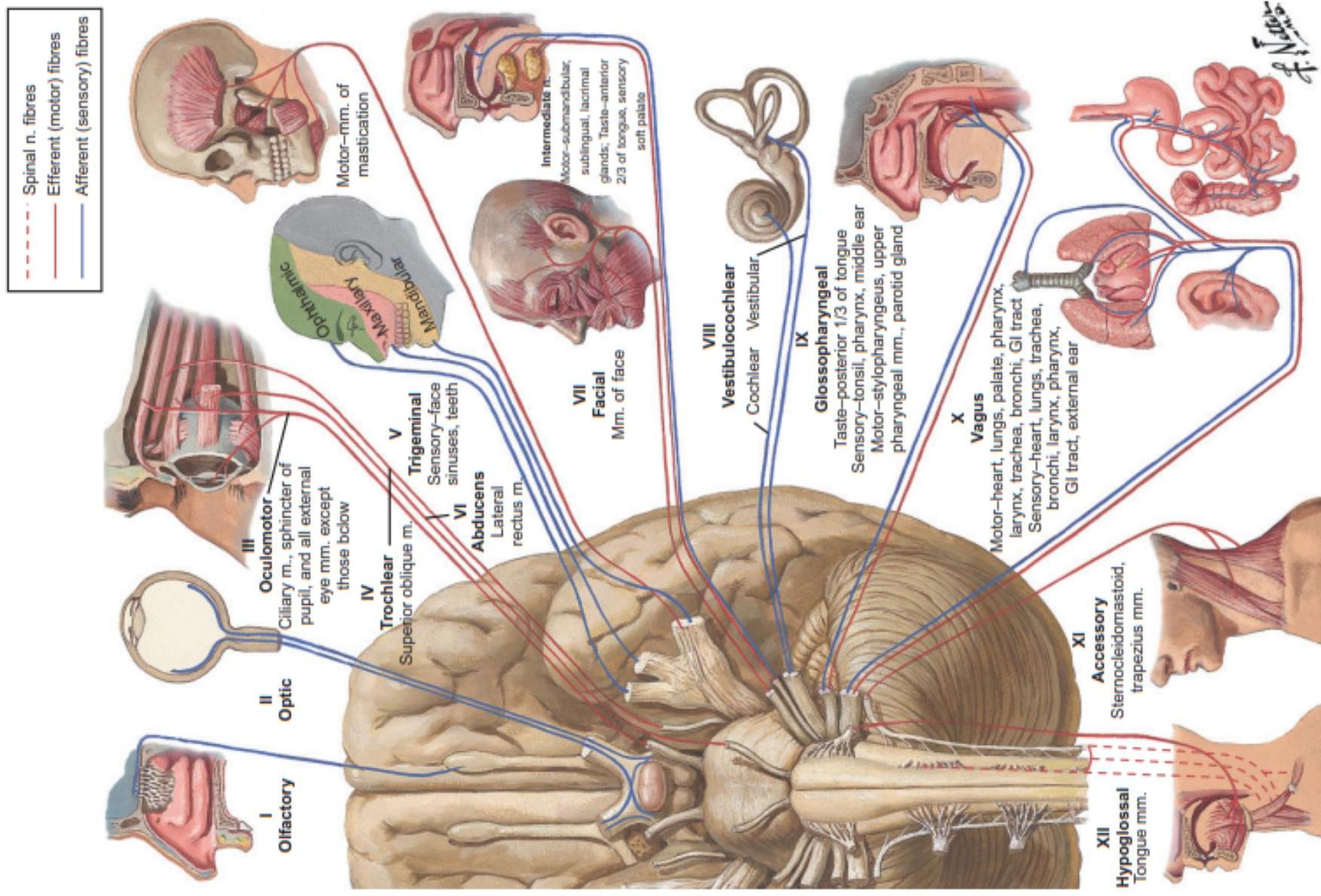 Fig. 28.5 The cranial nerves. (© 2016 Elsevier Inc. All rights reserved. www.netterimages.com)
Fig. 28.5 The cranial nerves. (© 2016 Elsevier Inc. All rights reserved. www.netterimages.com)
CN VII: Facial Nerve (Face Ear Taste Tear)
- Mnemonic: Face Ear Taste Tear.
- You must examine the motor and the sensory. Also Inspect the symmetry of the face.
Inspection
- Facial symmetry, flattening of nasolabial folds, deviation of angle of mouth, opening of eye.
Motor Examination
- Raise the eyebrows noticing the wrinkles. (temporal branch)
- Close their eyes and you try to gently open them (zygomatic branch)
- Blow their cheeks. Tap with finger over each cheek noticing the ability to close their lips. (Buccal, Mandibular)
- Whistle (orbicularis oris).
Sensory Examination
- Taste and sensation of the anterior two thirds of the tongue.
Branches
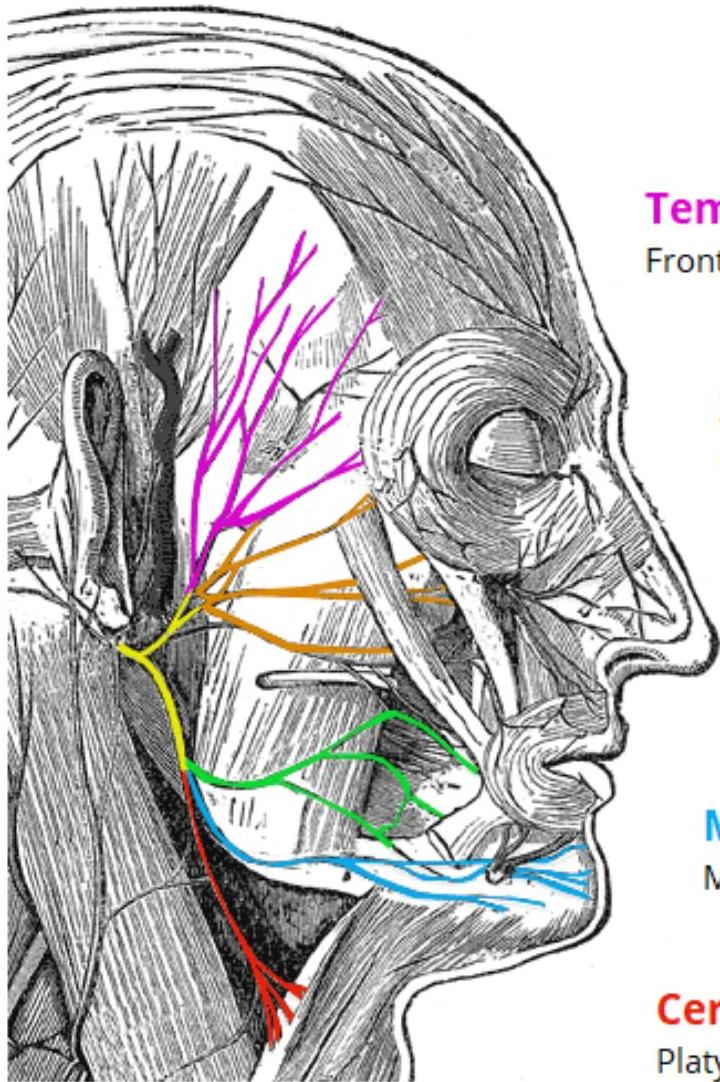
- Temporal branches: Frontalis, orbicularis oculi, corrugator supercilii
- Zygomatic branches: Orbicularis oculi
- Buccal branches: Orbicularis oris, buccinator, zygomaticus
- Marginal mandibular branches: Mentalis, depressor labii inferioris, depressor anguli oris
- Cervical branches: Platysma
TeachMeSeries.com - Educational Healthcare Resources
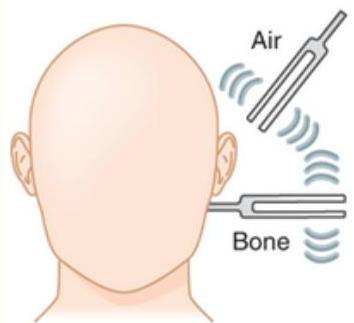
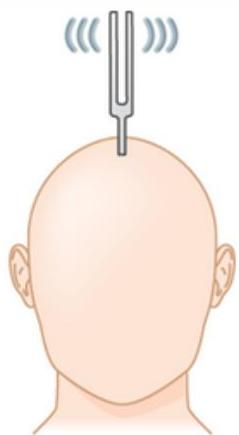
CN VIII: Vestibulocochlear Nerve
- Tests: Rinne’s / Weber’s test.
 Rinne test
Rinne test
 Weber test
Weber test
| Hearing loss | Rinne test (Conduction) | Weber test (Localization) |
|---|---|---|
| None | Air > bone | Midline |
| Sensorineural | Air > bone | Normal ear |
| Conductive | Bone > air | Affected ear |
 WEBER TEST: “Where do you hear the sound?”
WEBER TEST: “Where do you hear the sound?”
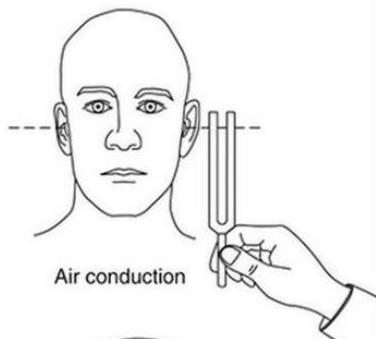 RINNE TEST: Air conduction
RINNE TEST: Air conduction
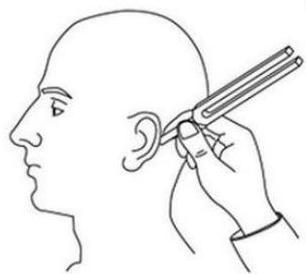 Bone conduction
Bone conduction
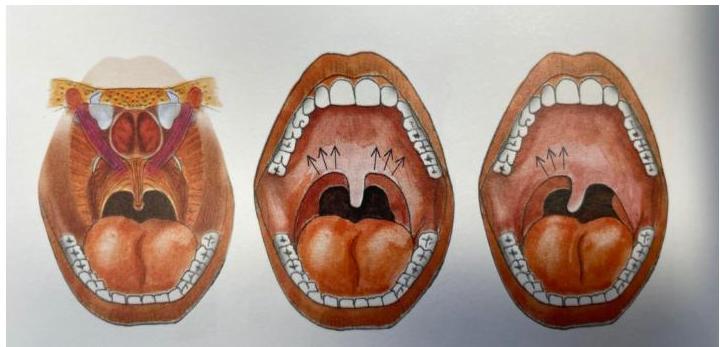
CN IX & X: Glossopharyngeal & Vagus Nerves
- Sensory (CN 9): Taste of Posterior third of tongue.
- Motor (CN 9 & CN 10):
- Ask the child to open their mouth and say ‘ahh’.
- Comment on motion of the soft palate and position of the uvula.
- Comment on strength of sucking and act of swallowing.
- Comment on voice.
CN XI: Accessory Nerve
You will examine the sternocleidomastoid and trapezius muscles.
- If infant: let the mother throw a toy or mother call his name and when he turns his head to look at her, comment on sternomastoid muscle of opposite side.
- If older child:
- Ask the child to shrug his shoulder.
- Put your hand on the medial side of the child’s jaw and ask him to push against your hand while you are palpating the opposite sternocleidomastoid muscles.
- Put your hand on the forehead of the child and ask him to flex his head forward against the resistance of your hand and compare the 2 sternocleidomastoid muscles.
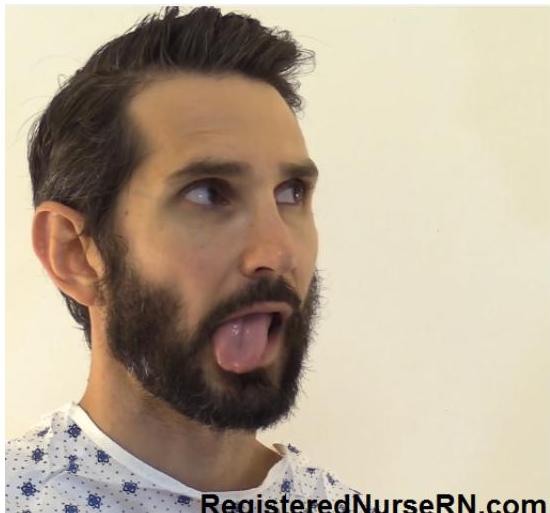
CN XII: Hypoglossal Nerve
- Look at the child’s tongue, while inside the mouth and comment on size, position, wasting, fasciculation.
- Ask the child to stick out their tongue.
- Remember: tongue deviates to the side of the lesion.
 RegisteredNurseRN.com
RegisteredNurseRN.com
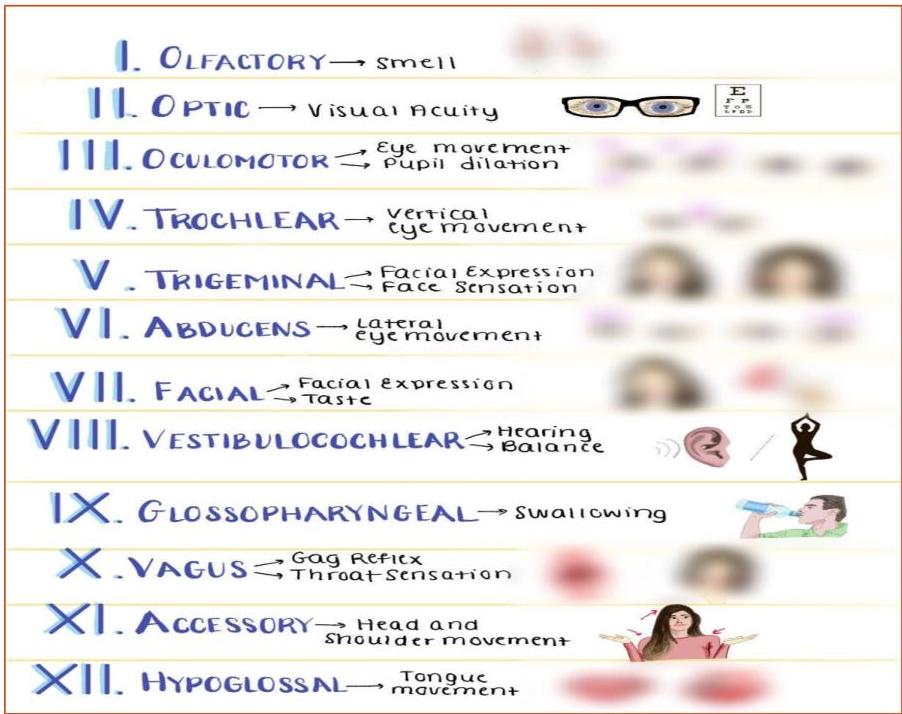
Summary of Cranial Nerve Functions
- Olfactory (CN I): Smell
- Optic (CN II): Vision
- Oculomotor (CN III): Eye movement, eyelids, pupils
- Trochlear (CN IV): Eye movement
- Trigeminal (CN V): Chewing, corneal reflex, face & scalp
- Abducent (CN VI): Lateral eye movement
- Facial (CN VII): Expressions-forehead, eye, mouth and taste
- Acoustic (CN VIII): Hearing Balance
- Glossopharyngeal (CN IX): Swallowing, Saliva, taste
- Vagus (CN X): Swallowing, gag reflex, talking, Sensations of throat, larynx, abdominal & thoracic visceral
- Accessory (CN XI): Shoulder movement, Head rotation
- Hypoglossal (CN XII): Tongue movement
MOTOR & SENSORY EXAMINATION: GENERAL PRINCIPLES
Causes of Weakness
Four major reasons why muscle weakness occurs:
- UMN lesion
- LMN lesion (spinal cord or peripheral nerve)
- Abnormalities in neuromuscular junction such as MG
- Disease of the muscle
Components of Limb Examination
Examining limbs consist of motor system examination and sensory system examination.
| Motor | Sensory |
|---|---|
| • Posture | • Pain and temperature |
| • Muscle Bulk | • Abnormal movements |
| • Abnormal movements | • Vibration and proprioception |
| • Fasciculations | • Light touch |
| • Tone | |
| • Power reflexes | |
| • Coordination |
Grading of Power
MRC Scale
| Grade | Muscle Power | Muscle Response (Detailed) |
|---|---|---|
| 0 | Zero | No muscle contraction is seen or identified with palpation. Generally seen in case of complete paralysis. |
| 1 | Trace | Flicker or Trace of contraction is seen (palpable), but insufficient to produce joint movement. |
| 2 | Poor | Active movement only with gravity eliminated (can move joint full range if gravity eliminated). |
| 3 | Fair | Active movement against gravity but not resistance (full range against gravity). |
| 4 | Good | Active movement against gravity with some resistance. |
| 5 | Normal | Active movement against gravity with full resistance. |
If power is reduced, look for:
- Symmetrical or asymmetrical?
- One muscle or group of muscles?
- Associated with joint pain?
UMN vs LMN Lesions
| Upper Motor Neuron (UMN) Lesions | Lower Motor Neuron (LMN) Lesions |
|---|---|
| Loss of muscle strength | Loss of strength |
| Hypertonia (Spasticity) | Decreased tone (Hypotonia/Flaccidity) |
| Hyperreflexia | Absent deep tendon reflexes |
| Upgoing plantar (Babinski) | Normal or absent plantar response |
| Little muscle wasting | Atrophy and muscle wasting (Prominent) |
| Clonus often associated | Fasciculations may be present |
| Weakness patterns: • Lower limb: marked in flexors/abductors • Upper limb: marked in abductors/extensors | Weakness: • More obvious distally than proximally • Flexor and extensor muscles equally involved |
Tone Assessment
You assess tone looking for one of the following:
-
Spasticity:
- “Velocity-dependent”, meaning the faster you move the limb, the worse it is.
- Increased tone in the initial part of the movement which then suddenly reduces past a certain point (known as “clasp knife spasticity”).
- Typically accompanied by weakness.
- Associated with pyramidal tract lesions (e.g. cerebral palsy).
- Video Reference
-
Rigidity:
- “Velocity independent” meaning it feels the same if you move the limb rapidly or slowly.
- Associated with extrapyramidal tract lesions.
-
Clonus:
- A series of involuntary rhythmic muscular contractions and relaxations.
- Associated with upper motor neuron lesions of the descending motor pathways (e.g. cerebral palsy).

UPPER LIMB EXAMINATION
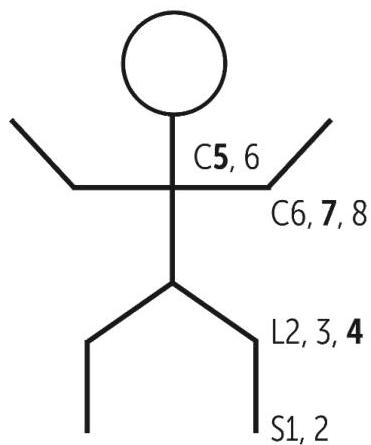
Myotomes (Power Testing)
- Shoulders:
- Abduction: deltoid and supraspinatus muscle (C5)
- Adduction: pectoralis major muscle (C7, C8)
- Elbow:
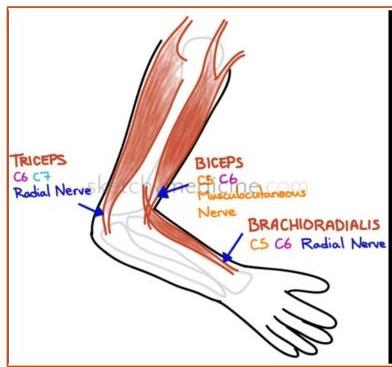
- Flexion: biceps and brachialis (C5, C6)
- Extension: triceps (C7, C8)
- Wrist:
- Flexion: flexor carpi ulnaris and radialis
- Extension: extensor carpi group
- Fingers:
- Extension and flexion
- Hands test: Squeeze fingers / Spread fingers out wide.
Detailed Examination Steps (Box 28.4)
- General observation – take note of clues such as the child’s wheelchair, orthoses or splints, helmet or dysmorphic features.
- Exposure - Ask the child and parent to expose the chest and arms fully.
- Inspection – with the child standing inspect for:
- Posture
- Contractures
- Muscle bulk, wasting and (pseudo) hypertrophy
- Involuntary muscles and fasciculations
- Scars
- Limb shortening
- Tone – whilst holding on to their hand passively, move their arm in unexpected, irregular movements.
- Power – compare both sides (see Myotomes above).
- Reflexes – compare both sides:
- Biceps (C5, C6)
- Triceps (C7, C8)
- Brachioradialis (supinator) (C5, C6)
- Coordination:
- Finger-nose test (assess for dysmetria) – ask the child to touch their nose with their index finger, and then your finger. You must move your finger to different sites at different arm lengths.
- Hand-tapping (assess for dysdiadochokinesia) – get them to tap one hand on the back of another and to alternate tapping between the palm and back of the hand.
- Sensation:
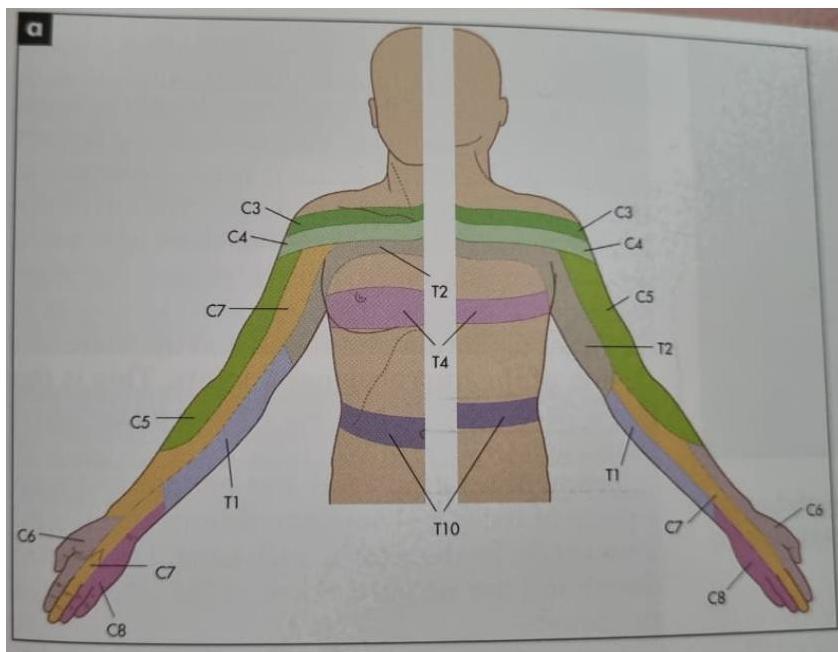
- Important to have a rough idea about dermatomes:
- C4 – tip of shoulder
- C5 – lateral surface of upper arm
- C6 – lateral surface of forearm
- C7 – radial surface of middle finger
- C8 – ulnar border of hand
- T1 – medial surface of forearm
- T2 – medial surface of upper arm
- Important to have a rough idea about dermatomes:
- Function: assessed by asking the child to draw/write/pick up objects.
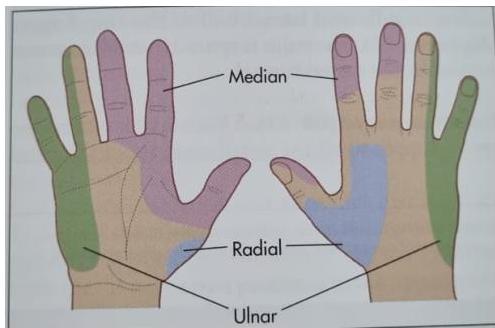
Nerve Lesions Notes
- Wrist drop: radial nerve (C5-C8)
- Claw like hand: ulnar nerve (C8-T1) and median nerve (C6-T1)
- Erbs: C5, C6
- Klumpke (+horner syndrome): C8, C11
LOWER LIMB EXAMINATION
Myotomes (Power Testing)
- Hip:
- Flexion: psoas and iliacus (L1, L2)
- Extension: gluteus maximus (L5, S1)
- Abduction: gluteus medius and minimus, sartorius
- Adduction: adductor longus, brevis, magnus
- Knee:
- Flexion: hamstring (L3, L4)
- Extension: quadriceps femoris (S1)
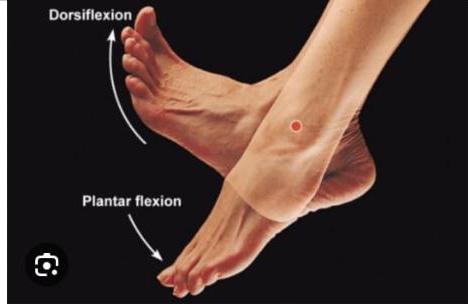
- Ankle:
- Plantar flexion: Gastrocnemius, plantaris (S1, S2)
- Dorsiflexion: Tibialis anterior, extensor digitorum longus (L4)
- Tarsal joint
Detailed Examination Steps (Box 28.5)
- General observation – take note of clues such as the child’s wheelchair, orthoses or splints, helmet or dysmorphic features.
- Exposure - Ask the child and parent to undress to their underpants only.
- Assess the child’s gait (see Gait Examination section).
- Inspection – with the child lying on the bed, inspect the child’s legs and spine. Note: Posture, Contractures, Muscle bulk, Wasting and (pseudo) hypertrophy, Involuntary muscles/fasciculations, Scars.
- Assess Tone:
- Roll the legs from side to side taking note of movement of the foot at the ankle.
- Place the palmar surfaces of both one’s hands underneath the child’s thighs and lift the thighs up slightly off the bed and then let them fall.
- Flex and extend at the hip, knee and ankle joints.
- Clonus – test both ankles by rapidly dorsiflexing the foot – more than 3 beats of ankle clonus is abnormal.
- Power (see Myotomes above).
- Reflexes – compare both sides:
- Knee jerk (Patellar) (L3-L4)
- Ankle jerk (Achilles) (S1-S2)
- Plantar Reflex (Babinski) (L5, S1, S2) - an abnormal reflex (positive Babinski) is for the great toe to be up-going and therefore the toes to be splayed when stroking the lateral aspect of the sole of the foot and medially across the ball of the foot. (Positive Babinski is a normal finding in infants).
- Coordination:
- Heel-shin test (test both sides). Best demonstrated to them using their foot rather than explaining verbally.
- Sensation:
- Test light touch, vibration and joint proprioception (pain sensation is not usually expected to be tested).
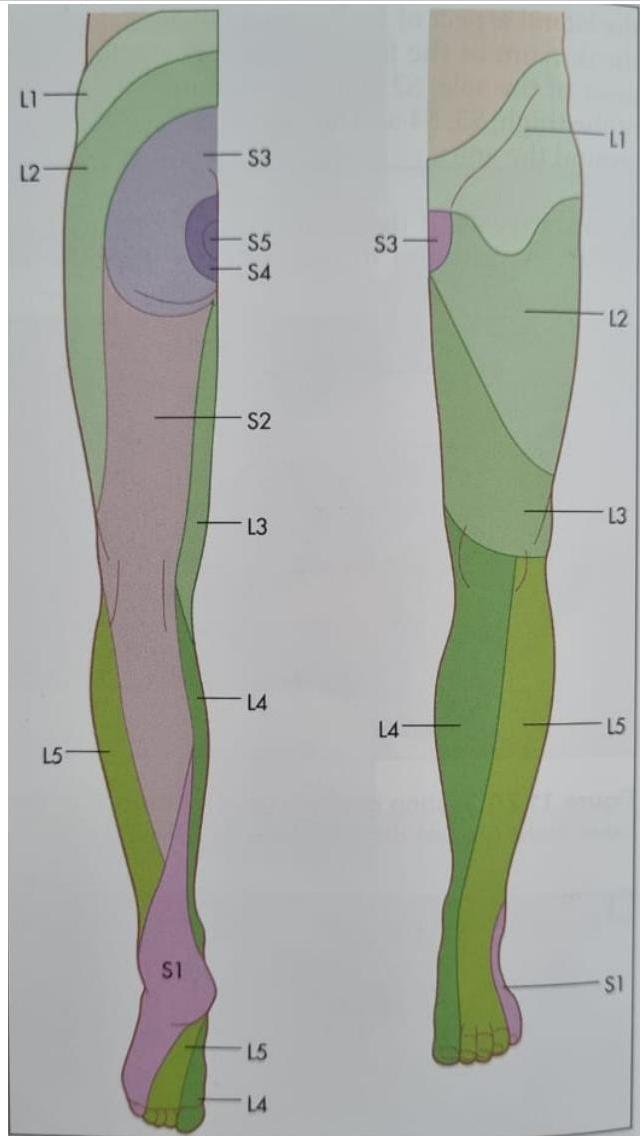
- Dermatomes:
- L1 – upper outer thigh
- L2 – middle anterior thigh
- L3 – anterior knee
- L4 – medial calf
- L5 – lateral calf
- S1 – sole of the foot
- S2 – strip up posterior and thigh
Quick Lower Limb Tests
- Stand up on toes: S1
- Stand up on heels: L4, L5
- Squat and stand up again: L3, L4
REFLEXES (GENERAL & GRADING)
Deep Tendon Reflex Grading
| Grade | DTR Response |
|---|---|
| 4+ | Very brisk, hyperactive, with clonus |
| 3+ | Brisker than average, slightly hyperreflexic |
| 2+ | Average, expected response; normal |
| 1+ | Somewhat diminished, low normal |
| 0 | No response, absent |
Clinical Correlation
- Reflexes reduced: Muscle disease, Neuropathy, Anterior spinal cord root, Anterior horn cell, Sensory nerve.
- Reflexes increased (+/- clonus): UMN lesions.
Specific Reflex Roots
- Biceps: C5, C6
- Triceps: C7, C8
- Brachioradialis: C5, C6
- Knee: L3, L4
- Ankle: S1, S2
- Plantar (Babinski): L5, S1, S2
- Abdominal reflexes: Epigastric (T6-T9), Midabdominal (T9-T11), Lower abdominal (T11-L1)
- Cremasteric Reflex: L1-L2
- Anal reflex: S2, S3, S4
SENSORY EXAMINATION
Pathways
- Pain and temperature: Spinothalamic pathway
- Vibration and proprioception: Posterior Columns
In pediatrics, you check sensation by two main steps: light touch and vibration. More steps are used as indicated.
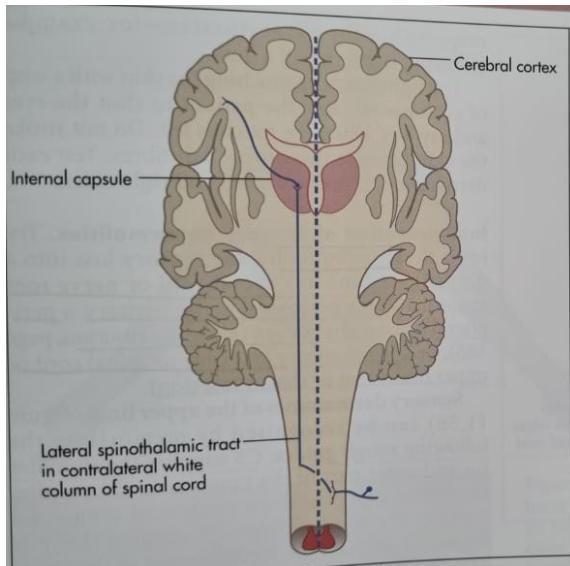 Figure 11.53 Pain and temperature pathways (Adapted from Snell RS, Westmoreland BF, Clinical neuroanatomy for medical students, 4th edn. Boston: Little Brown, 1997.)
Figure 11.53 Pain and temperature pathways (Adapted from Snell RS, Westmoreland BF, Clinical neuroanatomy for medical students, 4th edn. Boston: Little Brown, 1997.)
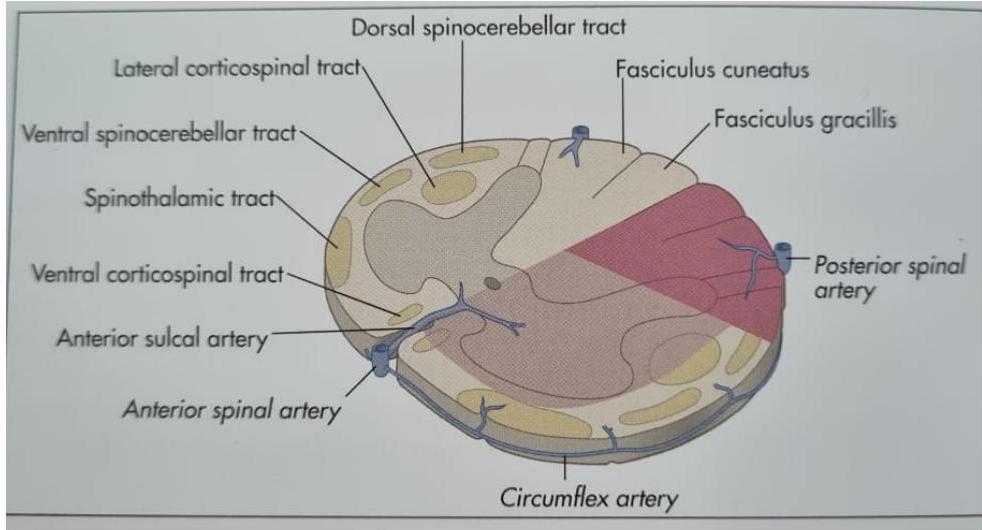
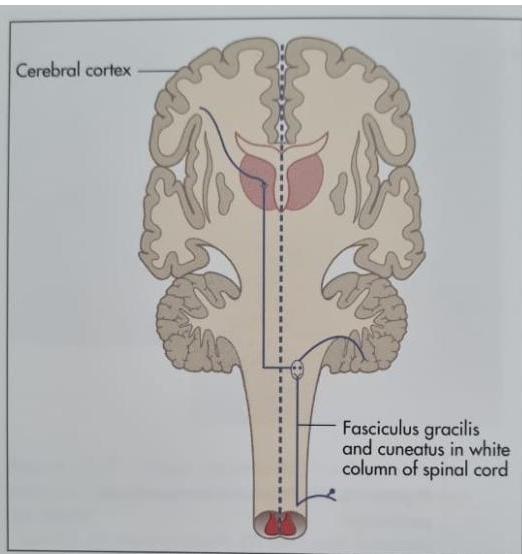 Figure 11.55 Vibration and joint position sense pathways
Figure 11.55 Vibration and joint position sense pathways
Dermatome Maps
COORDINATION (CEREBELLAR)
Tests
- Finger-nose test
- Dysdiadochokinesia test
- Heel-Shin test
- Toe-finger test
- Foot-tapping test
Additional Assessments
- Any general abnormal movements and telangiectasia on conjunctiva.
- Assess speech for dysarthria.
- Look at eyes for any nystagmus.
GAIT EXAMINATION
Do not forget to examine the gait. You can do it either at the beginning or at the end of your examination.
Examination Steps (Box 28.6)
- General observation: Wheelchair, orthoses, splints, helmet, dysmorphic features.
- Exposure: Undress to underpants only.
- Inspection (standing):
- Posture, Contractures, Muscle bulk, Wasting/(pseudo) hypertrophy, Involuntary muscles/fasciculations, Scars, Limb shortening.
- Spine: scars or lesions (overlying tuft of hair → spina bifida).
- Shoes: abnormal wear and tear.
- Walk across the room (Frontward and Backward):
- Assess heel-strike/toe-off phases.
- Foot position (varus/valgus).
- Noise (slapping gait → foot drop).
- Limp, Arm position/swing, Abnormal movements.
- Comment on: posture, speed, symmetry, balance.
- Heel-to-toe gait: assess cerebellar pathways (exclude mid-cerebellar lesions).
- Walk on the toes (S1).
- Walk on heels: exclude foot drop (L4, L5).
- Walk on outsides of feet (Fog’s test): exacerbates signs of subtle hemiplegia.
- Run across the room: exacerbates signs of subtle hemiplegia.
- Romberg test.
- Squat-stand: assess for proximal myopathy.
- Trendelenburg’s sign: for proximal (hip) muscle weakness.
- Ask child to stand in front of you facing away and lift one foot.
- Normal: pelvis rises on side of lifted leg.
- Abnormal: pelvis sags on side of lifted leg.
- Gower’s sign: assess for proximal muscle weakness.
- Child unable to stand from supine without turning prone and ‘walking’ hands up legs.
Gait Abnormalities
- Hemiplegic: foot is plantar flexed.
- Spastic: scissoring gait; bilateral legs stiff. The child’s feet may be inverted and “scissor”. This type of gait is typically associated with spastic paraplegia (CP).
- Cerebellar: wide-based.
- Footdrop: high stepping gait.
- Proximal myopathy: waddling gait.
- Ataxic gait: associated with either cerebellar pathology or sensory ataxia.
- Hemiparetic gait: one leg held stiffly and swings round in an arc with each stride (circumduction). This type of gait is commonly associated with individuals who have had a stroke.
NOTES & CHECKLISTS
Upon completing your neurological examination, done forget the following:
- Gait
- Skin and back (Deformity, Scars, Tenderness, Bruits)
- Anal reflex
- GCS
- Saddle region sensation
QUICK GUIDE: 4 UPPER LIMBS EXAMINATION
- General inspection (patient sitting to begin with):
- Scars
- Skin (e.g. neurofibromata, café-au-lait)
- Abnormal movements
- Shake hands.
- Motor system:
- Inspect arms, shoulder girdle (extend both arms): Wasting, Fasciculation, Tremor, Drift.
- Palpate: Muscle bulk, Tenderness.
- Tone: Wrist, Elbow.
- Power: Shoulder, Elbow, Wrist, Fingers.
- Ulnar, median nerve function.
- Reflexes: Biceps, Triceps, Supinator, Finger.
- Coordination: Finger—nose test—intention tremor, past-pointing, Dysdiadochokinesis, Rebound.
- Sensory system: Pain (pinprick), Vibration (128 Hz tuning fork), Proprioception—distal interphalangeal joint (each hand), Light touch (cottonwool).
QUICK GUIDE: 5 LOWER LIMBS EXAMINATION
(Patient lying)
- General inspection: Scars, skin, Urinary catheter.
- Gait.
- Motor system:
- Inspect: Wasting, Fasciculation, Tremor.
- Palpate: Muscle bulk, Muscle tenderness.
- Tone: Knee—and test for clonus, Ankle—and test for clonus.
- Power: Hip, Knee, Ankle, Foot.
- Reflexes: Knee, Ankle, Plantar.
- Coordination: Heel—shin test, Toe—finger test, Foot tapping test.
- Sensory system: Pain, Vibration, Proprioception, Light touch.
- Saddle region sensation.
- Anal reflex.
- Back: Deformity, Scars, Tenderness, Bruits.
THANK YOU