SYNCOPE IN CHILDREN
Objectives
- Understand the term syncope.
- Differentiate the serious causes of syncope from those that are benign.
- Know the appropriate testing needed in the evaluation of syncope based upon the presenting history.
Definitions to Know
- Palpitations: Sensation of strong, rapid, or irregular heart beats.
- Syncope: Transient loss of consciousness and postural tone due to generalized cerebral ischemia with rapid and spontaneous recovery.
- Presyncope: No complete loss of consciousness occurs.
Syncope Mimics
Disorders without impairment of consciousness
- Drop attacks.
- Cataplexy/Narcolepsy.
- Psychogenic pseudo-syncope.
- Transient ischemic attacks.
Disorders with loss of consciousness
- Metabolic disorders.
- Epilepsy.
- Intoxications.
- Vertebrobasilar transient ischemic attacks.
Epidemiology & Characteristics Z
- Affects 15% of children between 8-18 Y.
- Uncommon under age 7 Y therefore think about:
- Seizure disorders.
- Breath holding.
- Primary cardiac dysrhythmias.
- Cardiovascular causes unusual but life-threatening:
- Congenital malformations.
- Valvular disease.
- Electrical abnormalities.
Vasovagal Events
- 30% to 50% of cases.
- Decreased PVR.
- Decreased venous return.
- Decreased cardiac output.
- Hypotension.
- Bradycardia.
- In teens - think about pregnancy and drug abuse.
Likely Causes in Children
- Vasovagal.
- Situational.
- Psychiatric.
- Long QT.
- WPW syndrome.
- RV dysplasia.
- Hypertrophic cardiomyopathy.
- Catecholaminergic VT.
- Other genetic syndromes.
Differential Diagnosis: Seizures vs Hypotension
| Observation | Seizure | Inadequate Perfusion |
|---|---|---|
| Onset | Sudden | More gradual |
| Duration | Minutes | Seconds |
| Jerks | Frequent | Rare |
| Headache | Frequent (after) | Occasional (before) |
| Confusion after | Frequent | Rare |
| Incontinence | Frequent | Rare |
| Eye deviation | Horizontal | Vertical (or none) |
| Tongue biting | Frequent | Rare |
| Prodrome | Aura | Dizziness |
| EEG | Often abnormal | Usually normal |
Causes of True Syncope Z
Neurally-Mediated
- Vasovagal
- Carotid Sinus
- Situational
- Cough
- Post-Micturition
Orthostatic
- Drug-Induced
- Autonomic Nervous System Failure
- Primary
- Secondary
Cardiac Arrhythmia
- Brady
- SN Dysfunction
- AV Block
- Tachy
- VT
- SVT
- Long QT Syndrome
Structural Cardio-Pulmonary
- Acute Myocardial Ischemia
- Aortic Stenosis
- HCM
- Pulmonary Hypertension
- Aortic Dissection
Unexplained Causes = Approximately 1/3
Clinical Evaluation
Key Questions to Address with Initial Evaluation
- Is the loss of consciousness attributable to syncope or not?
- Is heart disease present or absent?
- Are there important clinical features in the history that suggest the diagnosis?
Important Historical Features
Circumstances just prior to attack Z
- Position (supine, sitting, standing)
- Activity (rest, change in posture, during or immediately after exercise, during or immediately after urination, defecation or swallowing)
- Predisposing factors (crowded or warm place, prolonged standing post-prandial period) and of precipitating events (fear, intense pain, neck movements)
Onset of the attack
- Nausea, vomiting, feeling cold, sweating, pain in chest
The Attack (Eye witness)
- Skin color (pallor, cyanotic).
- Duration of loss of consciousness.
- Movements (tonic-clonic, etc.).
- Tongue biting.
End of the attack
- Nausea, vomiting, diaphoresis, feeling cold, muscle aches, confusion, skin color, wounds.
Background
- Number and duration of syncope spells.
- Family history of arrhythmic disease or sudden death.
- Presence of cardiac disease.
- Neurological disease.
- Medications (Hypotensive, negative chronotropic and antidepressant agents).
Clinical Features Suggesting Specific Cause of Syncope Z
Neurally-Mediated Syncope Z
- Absence of cardiac disease.
- Long history of syncope.
- After sudden unexpected, unpleasant sensation.
- Prolonged standing in crowded, hot places.
- Nausea vomiting associated with syncope.
- During or after a meal.
- With head rotation or pressure on carotid sinus.
- After exertion.
Syncope due to Orthostatic Hypotension
- After standing up.
- Temporal relationship to taking a medication that can cause hypotension.
- Prolonged standing.
- Presence of autonomic neuropathy.
- After exertion.
Cardiac Syncope
- Presence of structural heart disease.
- With exertion or supine.
- Preceded by palpitations.
- Family history of sudden death.
Physical Examination
Initial Exam: Complete Physical Examination
- Vital signs:
- Heart rate.
- Orthostatic blood pressure change.
- Cardiovascular exam: Is heart disease present?
- ECG: Long QT, pre-excitation, conduction system disease.
- Echo: LV function, valve status, HCM.
- Neurological exam.
Orthostatic Measurements
- Classically, abnormal if systolic BP decreases by more than 20 points and/or pulse increases in pulse rate of more than 20 beats per minute after a change from supine to standing.
- If there is only a pulse increase but no drop in blood pressure, the test is less significant.
Diagnostic Testing & Management
Diagnostic Objectives
-
Distinguish true syncope from syncope mimics.
-
Determine presence of heart disease and risk for sudden death.
-
Establish the cause of syncope with sufficient certainty to:
- Assess prognosis confidently.
- Initiate effective preventive treatment.
Electrocardiogram (ECG)
- Yield for specific diagnosis low (5%).
- Risk free and relatively inexpensive.
- Abnormalities (BBB, previous MI, nonsustained VT) guide further evaluation.
- Recommended in almost all patients.
Laboratory Tests
- Routine use not recommended
- May be glucose?
- Should be done only if specifically suggested by H&P.
- Laboratory is often normal but may include:
- Electrolytes / Ca++, Mg++, PO4.
- CBC with differential.
- Cardiac enzyme.
Neurologic Testing
- EEG - not useful unless seizures.
- Brain imaging - not useful unless focality.
- Neurovascular studies.
- No studies.
- May be useful if bruits, or hx suggests vertebrobasilar insufficiency.
Radiology
- CXR offers little.
- CT or MRI of the brain and neck may be indicated if considering seizures or injury.
Advanced Cardiac Studies
- ECG/Holter.
- Echocardiography
- Cardiac MRI
- Continuous cardiac monitoring
- Stress ECG
- Genetic testing
Mortality Risk & Prognosis
“…CARDIAC SYNCOPE CAN BE A HARBINGER OF SUDDEN DEATH.”
- Survival with and without syncope (adults and children).
- 6-month mortality rate of greater than 10%.
- Cardiac syncope doubled the risk of death.
- Includes cardiac arrhythmias.
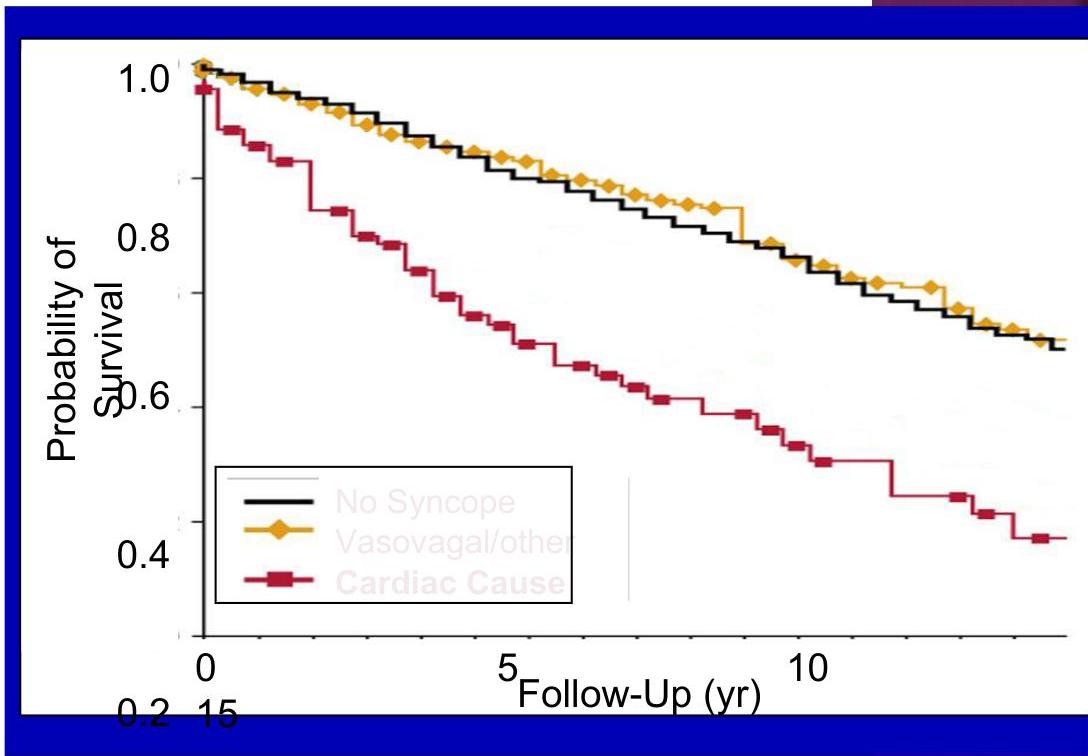
Soteriades ES, et al. N Engl J Med. 2002;347:878.
Case Study 1
Presentation:
- 11-year-old girl passed out during reading; awoke after 3 min.
- She was stiff with eyes rolled back ~ approx. 3 min.
- Now awake and alert; no retractions; skin color is normal.
- Normal appearance, normal breathing, normal circulation.
- Vital signs: HR 70; RR 20; BP 90/60; T 37.7° C Wt 39 kg; O₂ sat 99%.
- Three similar episodes; Preceded by palpitations, one of them associated with “exercise.” Z
- PMH and FH: Negative.
Discussion:
- What is your general impression of this patient?
Clinical Features: Your First Clue
- Loss of consciousness.
- Lasted only a few minutes.
- Minimal or no postictal state.
- No stigmata of seizure: Urinary incontinence, bitten tongue, witnessed tonic-clonic activity.
Key Questions to Address (Review):
- Is the loss of consciousness attributable to syncope or not?
- Is heart disease present or absent?
- Are there important clinical features in the history that suggest the diagnosis?
Status:
- Stable
- Patient with syncope.
- In no distress; normal exam.
- Concerning/ominous history.
Question:
- What are your initial management priorities?
Differential Diagnosis:
- Structural heart defect:
- Known Congenital heart disease (Ebstein’s anomaly, LTGA, ASD)
- Hypertrophic cardiomyopathy
- Anomalous origin of the LCA
- Myocarditis
- Arrhythmogenic RV dysplasia
- Coronary artery disease
- Primary or secondary pulmonary hypertension.
- Normal heart structure:
- WPW syndrome.
- Long or short QT syndrome.
- Brugada syndrome.
- CPVT.
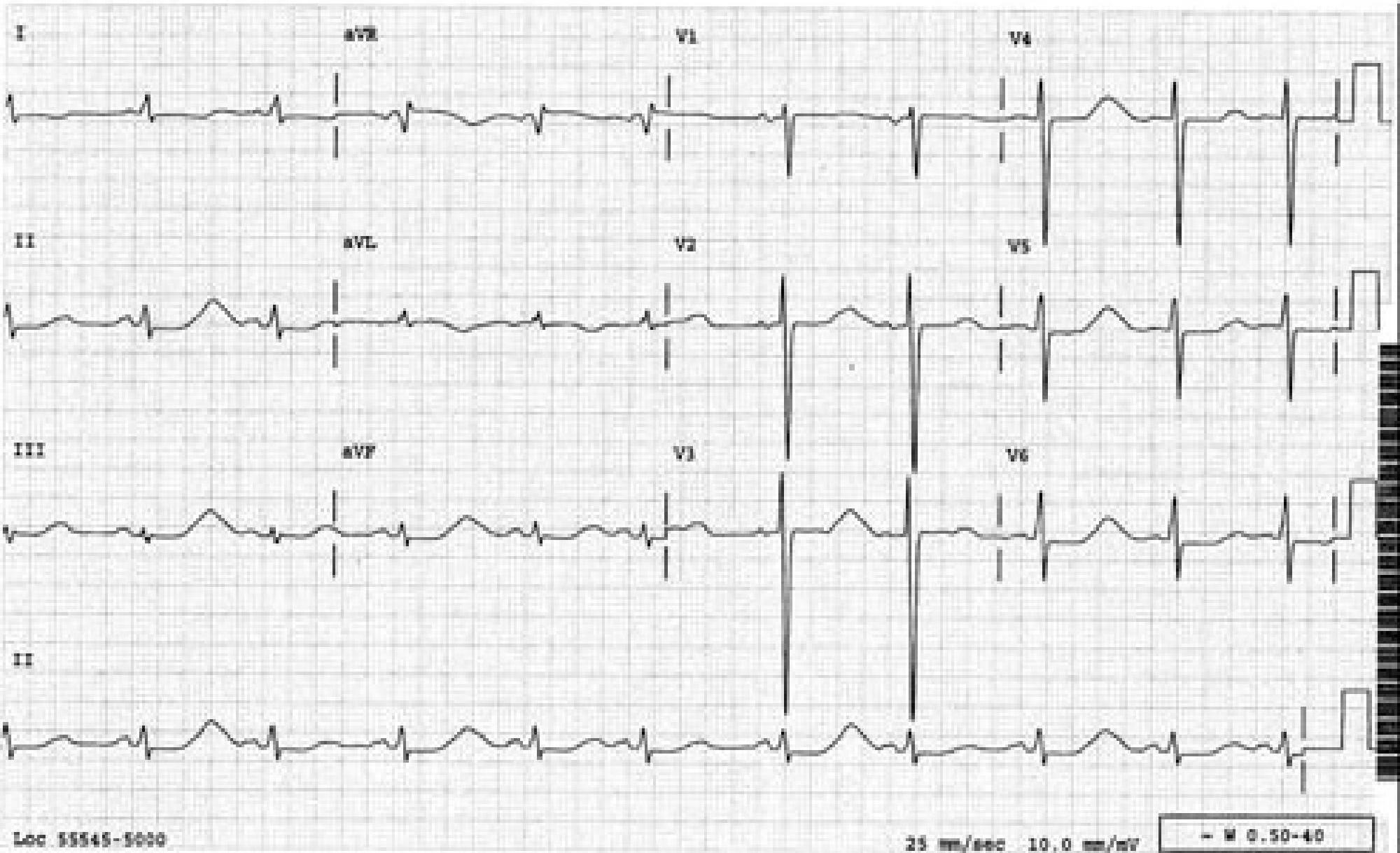
Loc 55545-5000 25 mm/sec 10.0 mm/mV W 0.50-40
Long QT Syndrome
Jervell-Nielson-Lange
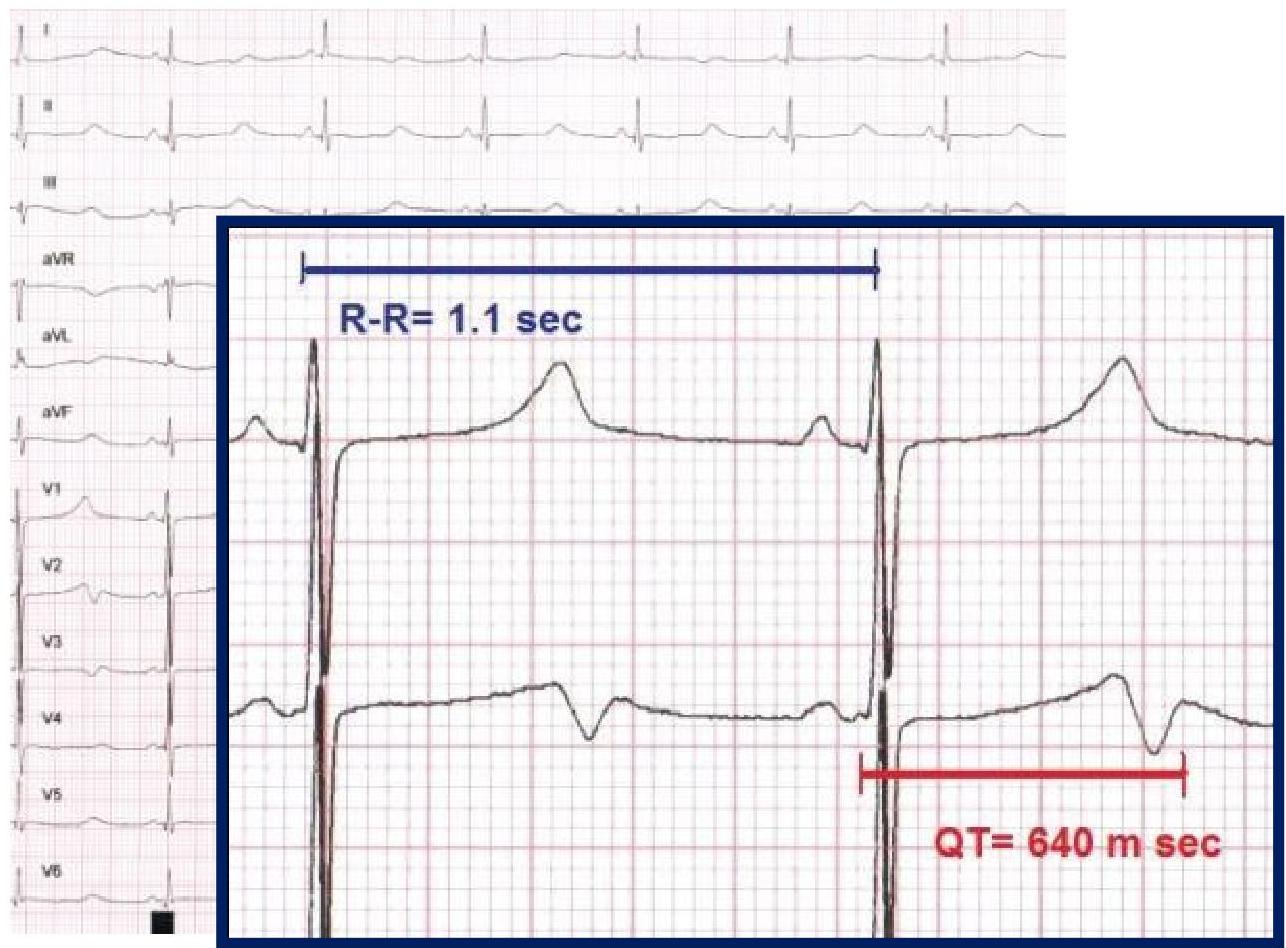
QT (corrected)
450 m sec is long
Overview
- Inherited genetic disorder that puts the child at risk for paroxysmal ventricular tachycardia /ventricular fibrillation and sudden death.
- May also result from electrolyte imbalance, malnutrition (anorexia and bulimia), myocarditis and CNS trauma
- Speculation that it may be associated with SIDS (unproven)
- No warning; results in death.
What to look for in the Department: EKG
- Long QT syndrome:
- Congenital long QT associated with hypertrophic cardiomyopathy.
- Long QT defined as corrected QT longer than 0.44 s
- T wave alternans sometimes present.
- Can have normal ECG in the department.
- Two clinical syndromes not associated with structural heart disease: Romano-Ward and Jervell-Lange-Nielsen.
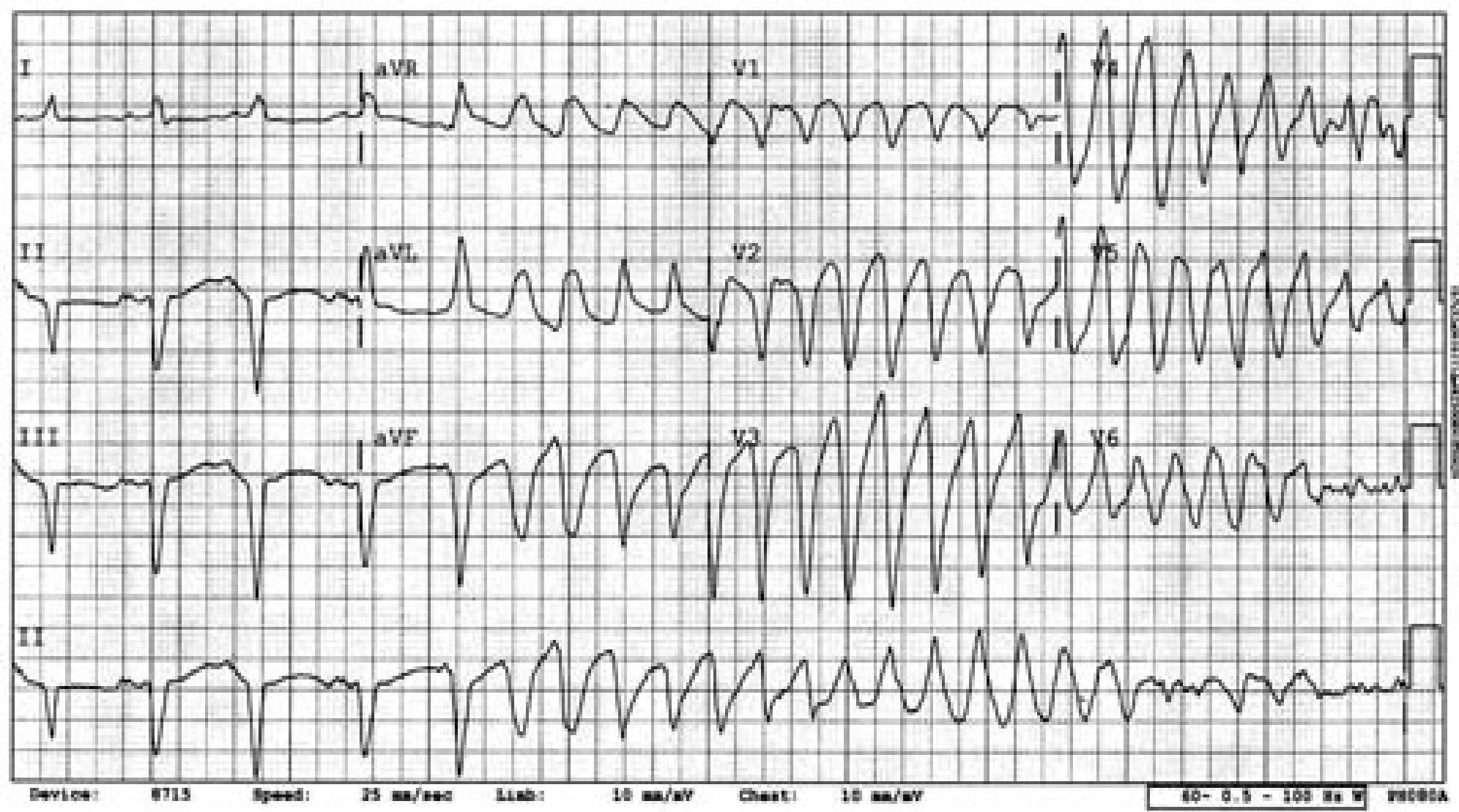
torrsado de pointes.
Final Words of Wisdom
-IS IT SYNCOPE?-
- History is key!!!!
- Orthostatics:
- Take the time to do them correctly.
- Cardiac vs Non-cardiac:
- If you are not confident that it is NOT cardiac → REFER.
- ECG
- Use it if you got ‘em!
.
which of following cardiac syncope, standing long time, dehydration, gym, family history of sudden death suggest qt -
or during exercise
Vasovagal attacks due .. .