PSORIASIS
Dr Sami Aldaham
What is Psoriasis?
- Psoriasis is chronic inflammatory non contagious T-cell mediated disease.
- Psoriasis may be associated with certain health related conditions as:
- Cardiovascular diseases
- Obesity
- Smoking
- Infections
Clinical features
- Psoriasis is the most common chronic papulosquamous disease.
- The classic lesion of psoriasis is a well-demarcated erythematous plaque with a silvery scale.
- Removal of the scale commonly results in bleeding whish is Auspitz sign; gently remove scales - pin point bleeding
The classical presentation

Epidemiology
- Psoriasis affects roughly 2% of the population.
- Equal sex distribution.
- Can occur at any age, but usually the onset is bimodal, between 20-30 and 50-60 years of age.
- Familial cases are not uncommon.
Etiology/Pathogenesis
- Genetic factors
- Environmental trigger factors
- Trauma – Koebner phenomenon; C
- Stress
- Streptococcal infection
- Drugs – e.g. lithium, beta blockers, possibly antimalarial agents
- Withdrawal of corticosteroid therapy as Pustular psoriasis Z - contraindication of systemic steroids for psoriasis
Clinical Variants
- Psoriasis vulgaris
- Psoriatic arthritis
- Guttate psoriasis
- Pustular psoriasis
- Inverse psoriasis
- Erythrodermic psoriasis
Psoriatic arthritis
- Affects between 7 to 21% of patients with psoriasis.
- May occur prior to, concurrent with or subsequent to psoriasis.
- More common in patients with moderate to severe cutaneous disease and those with nail involvement.
winter - tinea versicolor
Psoriasis Vulgaris
Skin scalp nail

 scalp at margins, without affecting hair
scalp at margins, without affecting hair
Nail Disease in Psoriasis


Guttate Psoriasis
red erythematous rain drops


Pustular Psoriasis
Generalized Pustular Psoriasis
 Localized Pustular Psoriasis
Localized Pustular Psoriasis

Erythrodermic Psoriasis

Koebner Phenomenon


Psoriatic Arthritis




Diagnosis of Psoriasis
- Usually is clinically diagnosis.
- Histopathology to confirm diagnosis and exclude other papulosquamous diseases and chronic eczemas. , tinea
Management of Psoriasis
- Patient education: Patient should be know:
- The disease could be not curable.
- Not contagious.
- Psoriasis is a common disorder.
- The exacerbating factors.
Treatment Categorization
Before starting treatment psoriasis should be categorized into:
Localized disease
- Topical steroid treatments
- Tar
- Corticosteroids
- Calcipotriene (vitamin D analogues)
- Tacrolimus and pimecrolimus
- Tazarotene
- Intense light or laser therapy (excimer laser 308 nm)
 Generalized disease
Generalized disease
- Phototherapy
- Systemic therapy

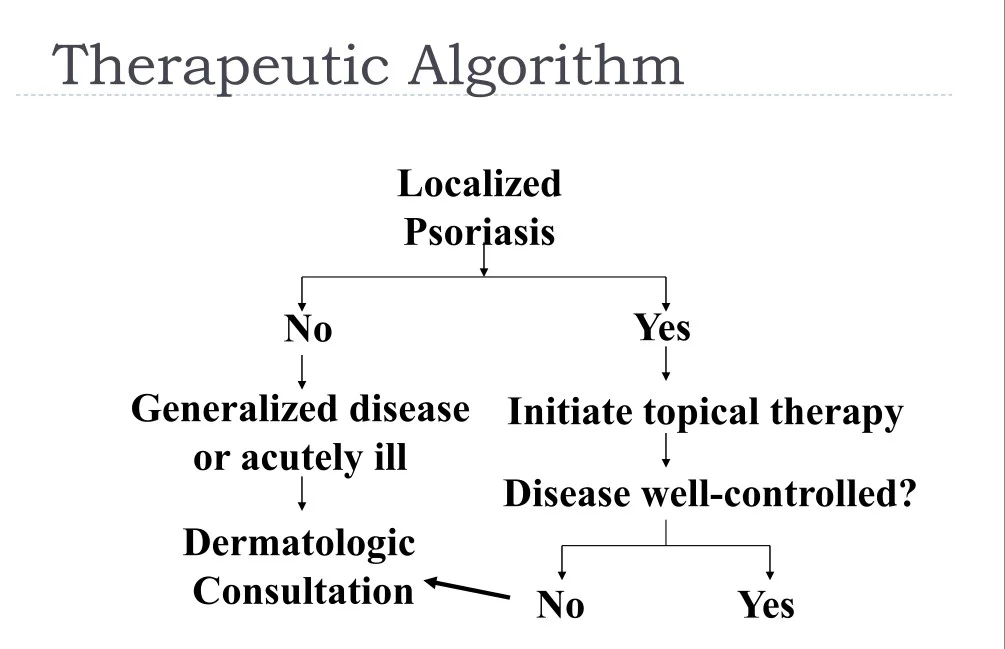
Therapeutic Algorithm
Treatment with 308 nm laser

Control the aggravating factors
- Obesity
- Smoking
- Drugs
Differential Diagnosis
- Chronic Dermatitis
- Seborrheic Dermatitis
- Pityriasis rosea
- Lupus erythematosus
- Dermatophyte infection
- Cutaneous T-cell lymphoma (mycosis fungoides)
- Lichen planus
Psoriasis treatment
- For limited psoriasis (less than 5% of BSA), topical therapies are first-line choices
- Potent topical steroids should be used once or twice daily for thickened plaques on the body
- For extensive psoriasis, systemic therapy is often necessary
- Narrow-band ultraviolet B phototherapy is very helpful in guttate psoriasis
Chronic Dermatitis

Pityriasis Rosea



Secondary Syphilis


Cutaneous Lupus Erythematosus


Dermatomyositis

Dermatophyte Infection


Onychomycosis


Cutaneous T-cell Lymphoma


Case Four
Case Four: History
- HPI: Wleed is a 15-year-old who presents with one week of small pink scaly round spots on his chest, abdomen, back, upper arms, thighs, and forehead. They itch somewhat.
- PMH: none
- Allergies: none
- Medications: none
- Family history: sister had strep throat a month ago
- Social history: lives with mother, father and three siblings (ages 3, 7, and 9)
- ROS: mild sore throat for past two weeks
Case Four: Skin Exam



Case Four, Question 1
- Waleed ‘s exam shows many guttate (raindrop-like) scaly pink to bright red circinate papules. They do not follow skin tension lines, and there is no oral, palm, or sole involvement. What is the first test you should perform?
a. Fungal culture b. Potassium hydroxide (KOH) exam c. Rapid plasma reagin d. Shave biopsy
Case Four, Question 2
- You perform a KOH exam to rule out tinea corporis, and it is negative. What is the most likely diagnosis for Waleed? a. Guttate psoriasis b. Nummular dermatitis (not associated with strep throat) c. Pityriasis rosea (follows skin tension lines) d. Secondary syphilis (can present this way and it is never wrong to order a screening test; no strep throat) e. Tinea corporis (should have positive KOH)
Psoriasis
- Psoriasis is a common, chronic, inflammatory multi-system disease that mostly involves skin and joints
- **Classic plaque psoriasis presents as pink to bright red well-demarcated plaques with silvery scale
- Usually located on extensor knees and elbows
- Commonly involves scalp, umbilicus, gluteal cleft, and nails
- Guttate psoriasis presents as small “drop-like” scaly papules and plaques mostly on the trunk and extremities
- Often follows group A beta hemolytic streptococcal infections

Now let’s look at a few examples of different psoriasis presentations
Classic psoriasis





Guttate psoriasis


Inverse psoriasis (in the folds)



