Retina
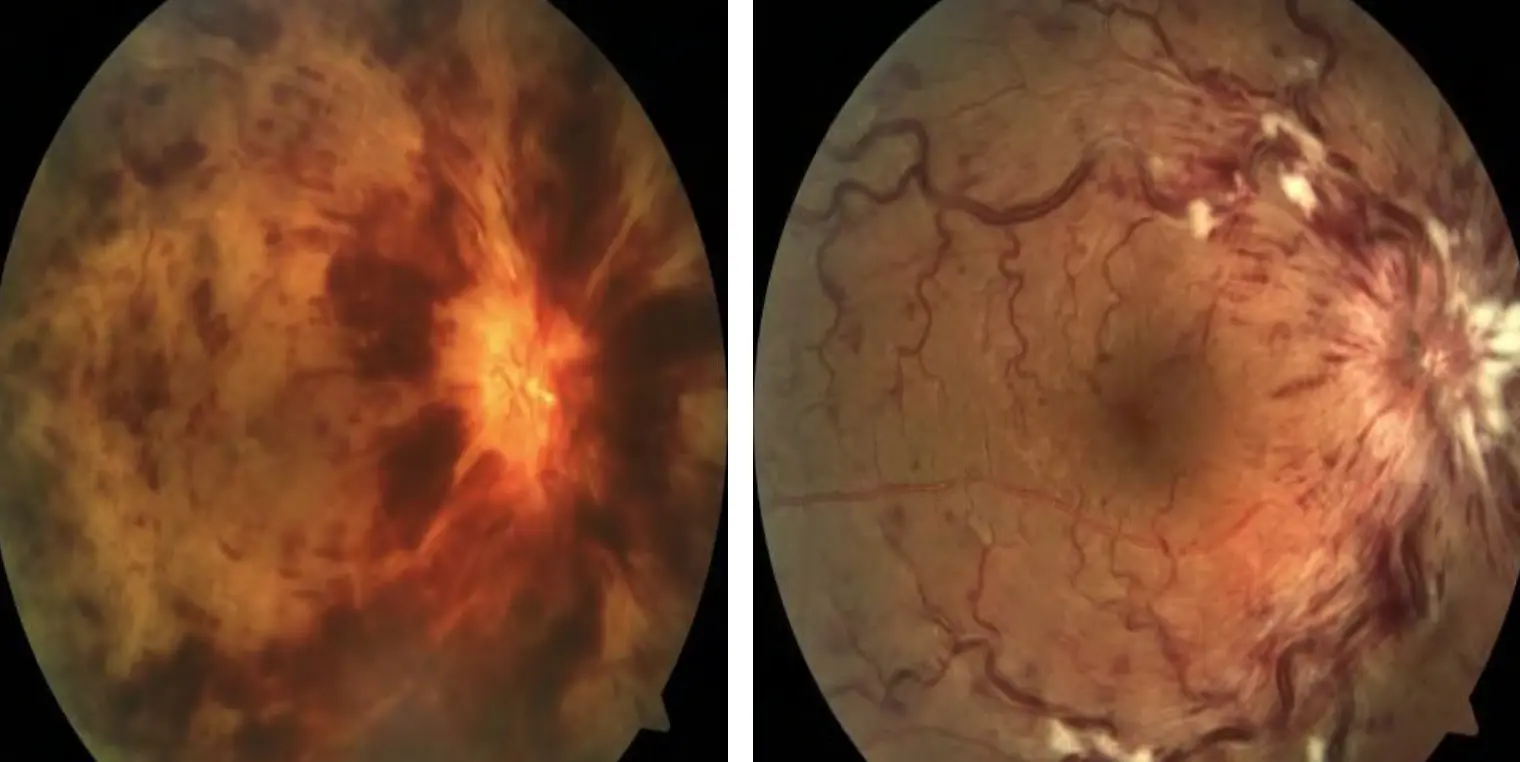
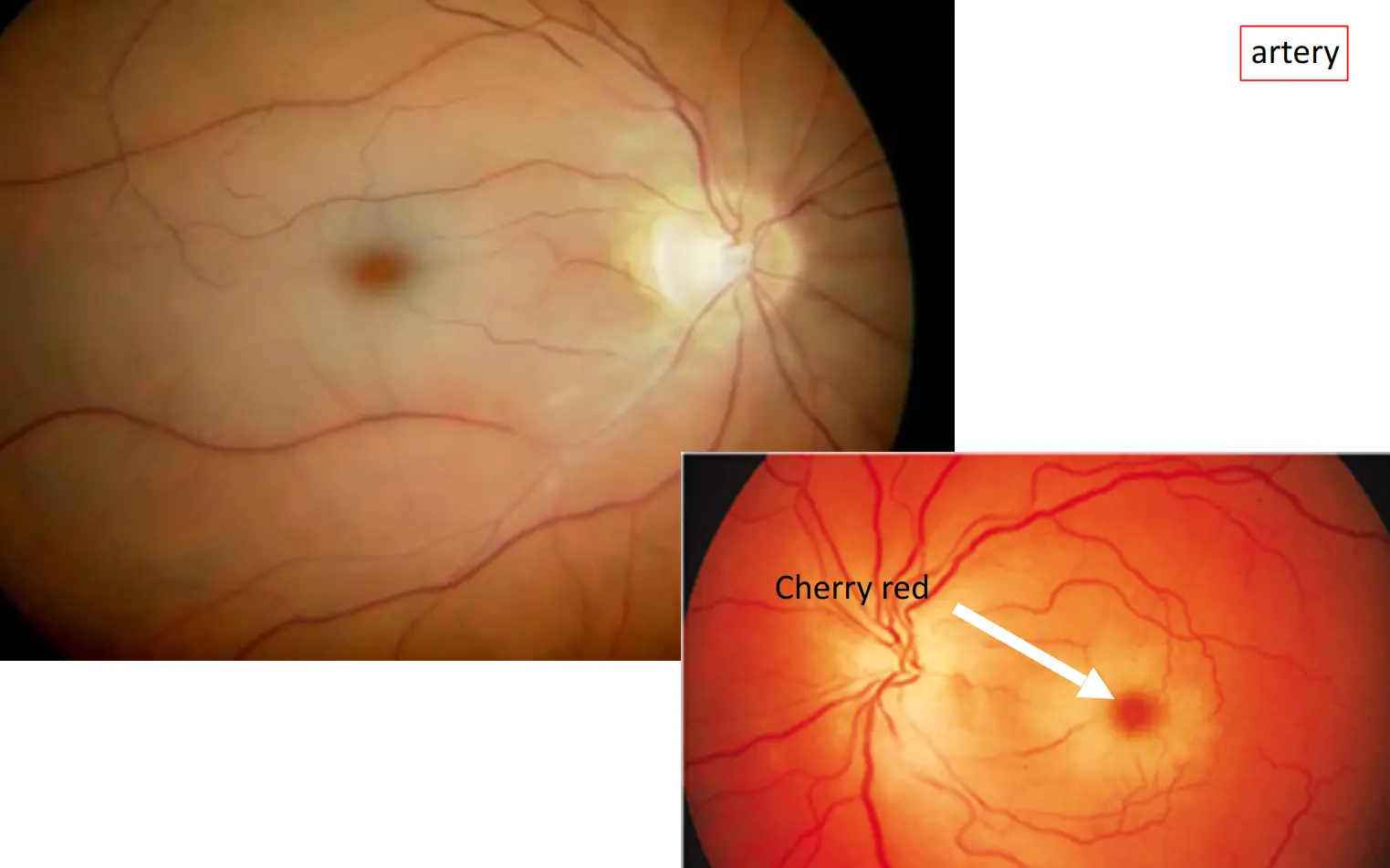
A 60-year-old woman noticed that her vision had become “dim” in her left eye one day ago. She felt well otherwise and had no pain. She came to the emergency room. History of hypertension 10 years. Vision was limited to light perception in the left eye, but right eye was 6/9. There was a left afferent pupiullary defect. Bilateral pseudophakia . IOP was 16 mmhg in OD and 14mmhge in OS.The fundus of the left eye showed narrowed vessels. Most of the retina was abnormally pale, and the macula showed a “cherry red spot”.
1- What is diagnosis?
Left Central retinal artery occlusion showing cherry red spot characteristic of Sudden loss of vision
2- Differential diagnosis
- Vitreous Hge
- CRVO
- AION (anterior ischemic optic neuropathy)
- Retinal detachment (RD)
3- Clinical Examination & Investigations
Clinical Exam
- ophthalmic examination ( VA - visual field - Slit lamp – Retinal and Pupil exam )
Investigations
- Flourescein Angiography and OCT
- Systemic Medical assessment eg Echo, ECG, CBC to save the other eye
4- Treatments
-
Treat the cause
-
*Target to reestablish retinal circulation & function
-
*Timing: the earlier the better
-
*Drugs: vasodilator (tropical or systemic) + reduce IOP
- Vasodilator : antispasm or pushing thrombus to the smaller branch Z
-
2. Oxygen inhalation:
- Mixture of 95% oxygen & 5% carbon dioxide
-
3. Reducing IOP: Z
- (1) Massage
- (2) Anterior chamber paracentesis
- (3) Diamox 500mg st; 250mg bid
- NaHCO3 500mg bid ~ tid
-
4. Fibrolytic enzyme: for patients suspect of thrombosis
- Urokinase 5 000 ~ 10 000U iv qd Z
![[Central Retinal Artery Occlusion CRAO-1745140572398.webp|357x198]] CRAO with cherry red
Clinical features Y
Retina
- History
- Retina
- Visual acuity
- Pupil
this is venous