Acromio-clavicular (AC) Dislocation
- Direct fall on shoulder tip
- More seen in cyclists
- Not an emergency because no major vascular involvement
- If open dislocation → semi-emergency
Treatment
- According to the stage (stages 1-3)
- Usually conservative: Sling
- Surgery:
- In unstable joints
- Completely displaced joints








Glenohumeral (Shoulder) Dislocation
- The most commonly dislocated joint
- Factors:
- Shallow glenoid socket
- Wide range of motion
Types
- Anterior: (the commonest)
- Posterior: (rare; less than 2%)
Stability Factors
- Static stabilizers: Ligaments, Labrum, Capsule
- Dynamic stabilizers: Muscles
Special Considerations
Think about the 3 E’s that can cause dislocations:
- Epilepsy
- Electric shock
- ETOH (Ethanol)
Even with these 3 conditions, the most common dislocation is still Anterior
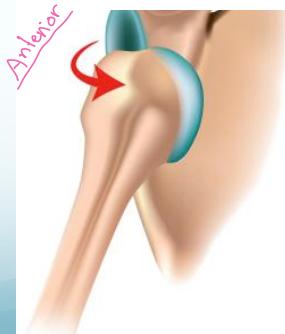
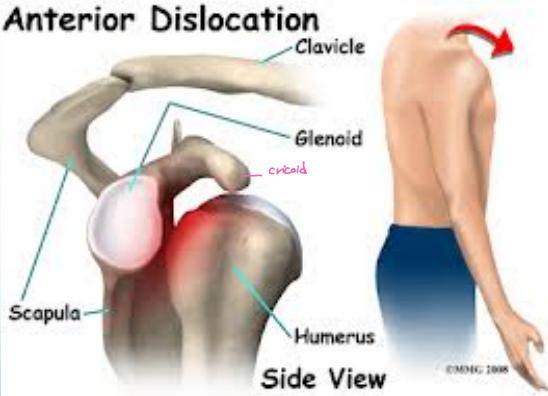
Anterior Shoulder Dislocation
Definition: The humeral head lies anterior to the glenoid
Mechanism of Injury:
- Forced abduction, external rotation:
- Throwing/catching a ball
- Hitting ball with racket
- Forced in weight-lifting
- A fall on the backward stretching hand
Clinical Picture:
- Patient holding the affected arm in adduction
- The lateral outline of the shoulder is flattened
- Bulge seen and felt below the clavicle
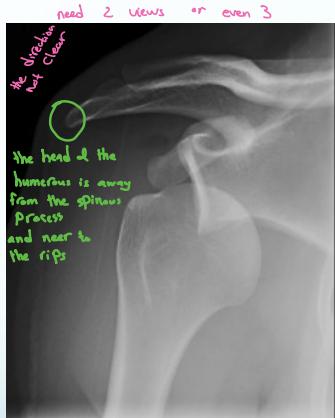
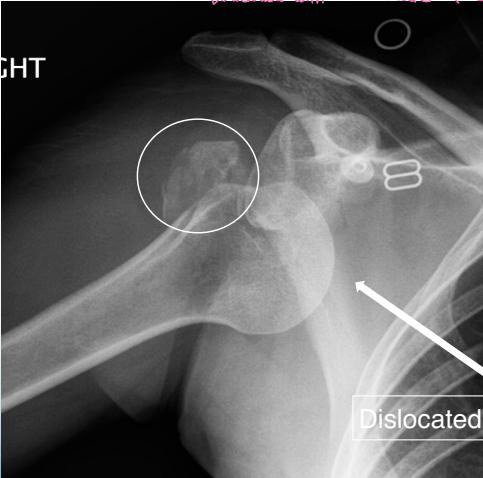
X-rays:
- AP (& lateral scapular) views
- Overlapping shadows of humeral head and glenoid
- Humeral head lies below and medial to glenoid
Important: Rule-out greater tuberosity fracture







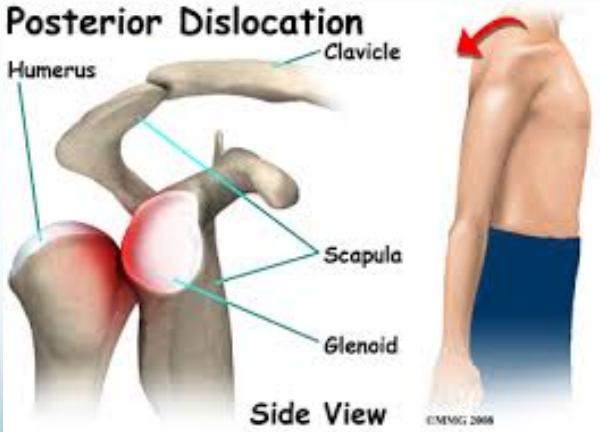
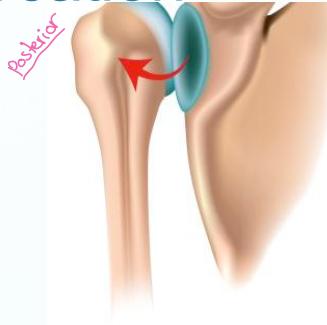
Posterior Shoulder Dislocation
Definition: The humeral head lies behind the glenoid
- Rare
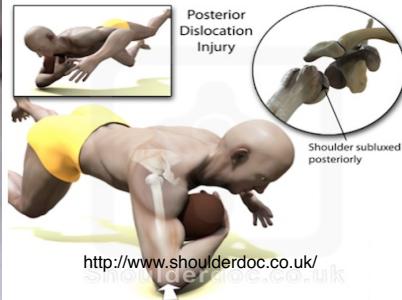
Mechanism of Injury:
- Indirect force producing marked (internal rotation & adduction)
- Convulsion, with an electric shock
- Direct fall on elbow with shoulder internally rotated
Clinical Picture:
- The diagnosis is frequently missed (>50%)
- The arm is held & locked in internal rotation
- The front of the shoulder looks flat with a prominent coracoid
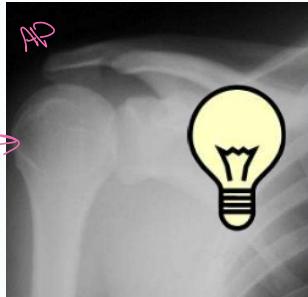
X-ray Findings:
- AP view:
- The humeral head is medially rotated → “Electric light bulb” sign
- The empty glenoid sign
- Posterior displacement
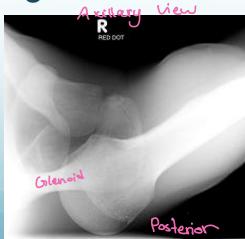
- Axillary & Scapular views are essential
- Rule-out fractures: neck, lesser tuberosity, glenoid
- CT Scan if still in doubt