Orthopedics Emergencies
- Acute Joint Dislocations
- Compartment Syndrome
- Septic arthritis
- Necrotising Fasciitis
Acute Joint Dislocations:/ Objectives
- To know mechanisms of joint dislocations
- To be able to make the diagnosis
- To know and interpret the appropriate x-rays
- To be able to describe principles of treatment
- To know the common complications and how to avoid them
Acute Joint Dislocations: General Principles
Definition
- An acute complete separation of contact of the joint articular surfaces
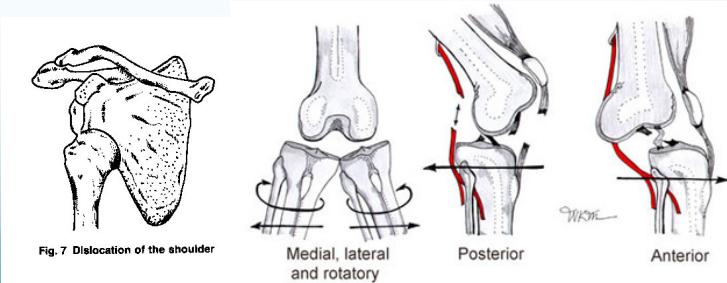
- Described according to position of distal fragment: Anterior, Posterior, Inferior, Superior, medial, lateral
- Results from significant trauma:
- ✓ Sport injuries
- ✓ RTA = MVA
Specific Joint Dislocations
Clinical Features
- Pain
- Abnormal shape of the joint
- Inability to move the limb
- The limb is held in a characteristic position
First Step (Most Important)
- Careful Neurovascular examination

Imaging
X-rays
- Adequate views – AP, (?lateral/others painful)
- ✓ Confirm the diagnosis
- ✓ Rule-out fractures (i.e. a fracture-dislocation)
- Reduce before X-rays in Knee, Ankle (due to vascular risks)
CT scan
- Needed in associated fractures (e.g. hip)
Clinical Note: Unless there’s absence of neurovascular function, perform reduction then X-ray. If neurovascularly intact, send patient to X-ray first.
General Treatment Protocol
1. Urgent Reduction
- Adequate analgesic, sedation, muscle relaxant or if failed: General Anesthesia
- Closed (or if failed: Open surgical)
- Check stability
Note: If reduction fails, consider:
- Fracture preventing reduction
- Wrong reduction technique
- Wrong diagnosis
2. Immobilization
- By splint (e.g. Knee), or traction (e.g. Hip)
3. Imaging After Reduction
- Confirms reduction
- Rules out fractures
4. Neurovascular Assessment
- Perform after reduction
5. Physiotherapy (Later)
- Initiate during recovery phase

General Complications
- Avascular necrosis of bone: Hip (10%), 40% if reduction is delayed by >12 hours
- Heterotopic ossification: Muscle soft tissue calcification around the joint
- Nerve injury:
- ✓ Axillary neuropraxia in shoulder
- ✓ Common peroneal nerve injury in knee (20%)
- ✓ Sciatic nerve injury in hip (10%)
- Recurrent dislocation: Shoulder most common joint
- Tendon tear: Rotator cuff in shoulder (more in elderly) above 40 y/o; in young patients more associated with fracture
- Vascular injury: Popliteal artery injury in Knee
Summary and Key Points
- Dislocation is an orthopedic emergency and needs urgent reduction
- Anterior shoulder dislocation is the commonest
- Obtain adequate imaging to rule out:
- Posterior shoulder dislocation (frequently missed)
- Fracture with posterior hip dislocation
- Always suspect vascular injuries with dislocated knee
- Neurovascular examination is mandatory before and after reduction
- Complications increase with delayed reduction, especially avascular necrosis in hip dislocations
References: