Rotational Deformities of Lower Limb
In-toeing / Ex-toeing
Clinical Features:
- Frequently seen
- Concerns parents
- Frequently prompts varieties of treatment
- Often unnecessary / incorrect
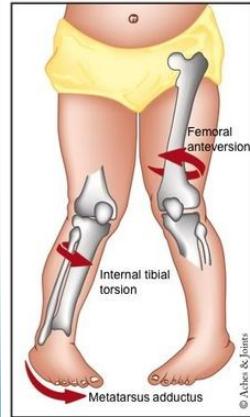
Level of Affection
- Femur
- Tibia
- Foot

Femoral Rotation
Terminology
- Ante-version = more medial rotation
- Retro-version = more lateral rotation
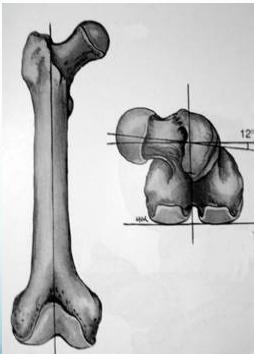
Normal anteversion

Increased anteversion
Normal Developmental Pattern
Age-Based Progression
Femur (Ante-version):
- 30 degrees at birth
- 10 degrees at maturity
Tibia (Lateral rotation):
- 5 degrees at birth
- 15 degrees at maturity
Growth Patterns
Key Principle: Both Femur and Tibia laterally rotate with growth in children
Conditions with Developmental Trajectory:
Improves with Growth
- Femoral ante-version
- Medial tibial torsion
= Improves (reduces) with growth
Worsens with Growth
- Lateral Tibial torsion
⇒
Increases (worsens) with growth
Clinical Examination
Rotational Profile Assessment
Purpose:
- Determine severity of rotational deformity
- Identify level of rotational deformity
Four Components:
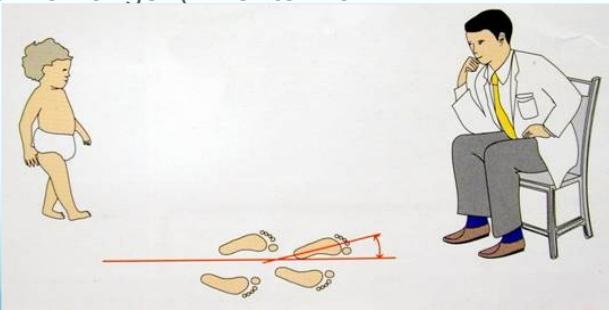
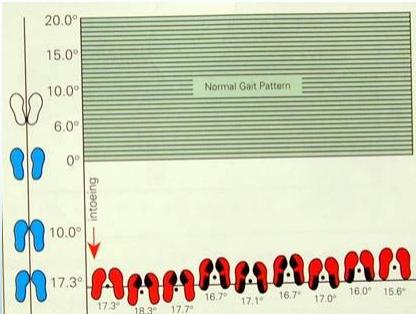
- Foot progression angle (walking)
- Femoral rotational arc assessment
- Tibial rotational arc assessment
- Foot assessment
Rotational Profile Components
1. Foot Progression Angle (Walking)
Normal Range: (+10° to -10°)
- In Eastern Societies: Normal range may be (+25° to -5°)
2. Femoral Rotational Arc Assessment
Position: Supine, Extended

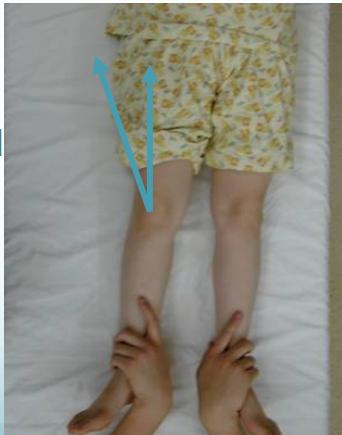
Position: Supine, Flexed


3. Tibial Rotational Arc Assessment
Techniques:
- Foot-thigh angle in prone position
- Bimalleolar axis measurement


4. Foot Assessment
Conditions to Evaluate:
- Metatarsus adductus
- Abducted great toe (“searching big toe”)
- Everted / Inverted foot
- Flat foot
In-Toeing Most common during second year (at beginning of walking)
Causes:
- Medial (internal) tibial torsion: does not need treatment
- Metatarsus adductus: may need treatment
- Abducted great toe: resolves spontaneously


In-toeing: due to medial femoral torsion
Out-toeing: in late childhood
- lateral femoral / tibial torsion
Management of Rotational Deformities
Key Principles
Clinical Challenge: Dealing effectively with family concerns and expectations
Natural History:
- In-toeing spontaneously corrects in vast majority of children as lower limbs externally rotate with growth
- Best approach: Wait and observe
Statistics: Only < 1% of femoral & tibial torsional deformities fail to resolve and may require surgery in late childhood
Ineffective Treatments
Shoe Wedges - Ineffective
Research shows minimal impact on correcting rotational deformities.
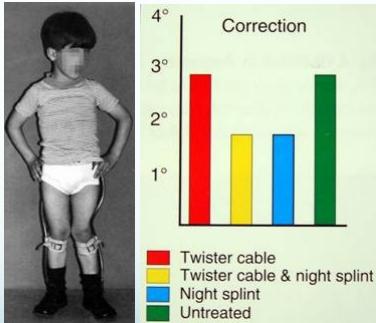
Twister Cables - Ineffective
Studies show minimal correction compared to untreated cases.
Referral Criteria for Rotational Deformities
Indications for Specialist Referral
- Severe & persistent deformity
- Age > 8-10 years
- Causing functional disability
- Progressive worsening