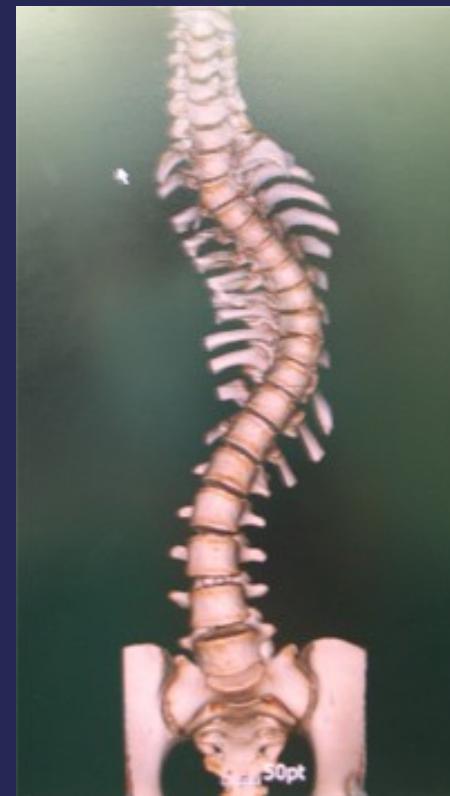
Scoliosis
- Definition: Lateral curvature of the spine >10° accompanied by vertebral rotation
- Types:
- Postural: Secondary to pathology outside the spine (e.g., limb length discrepancy, pelvic tilt)
- Correctable/Disappears with sitting
- Structural: Fixed deformity that does not disappear with sitting
- Congenital bony abnormality
- Idiopathic (most common)
- Postural: Secondary to pathology outside the spine (e.g., limb length discrepancy, pelvic tilt)


Adolescent Idiopathic Scoliosis (AIS)
Most common type of scoliosis
Clinical Presentation
- Demographics: Adolescent girls (10-16y) more common than boys (12-16y)
- Presenting complaint: Back deformity or shoulder inequality
- Key feature: Painless (pain suggests tumor or infection)
- Progression: Curves progress continuously until maturity, then slower after maturity
- Complications: Severe curves may affect pulmonary function
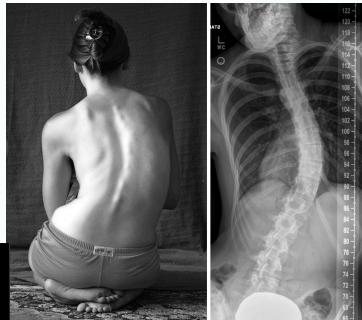
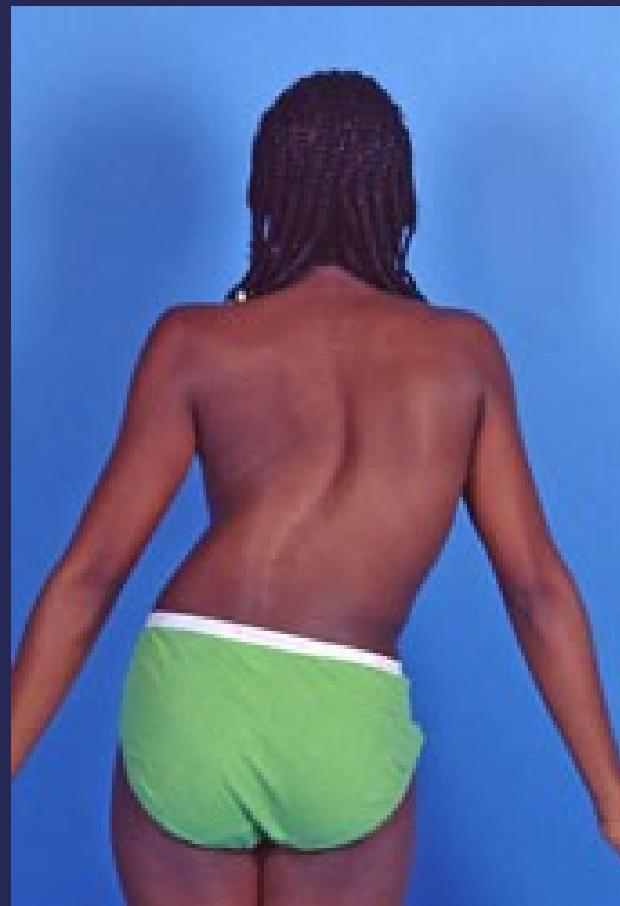
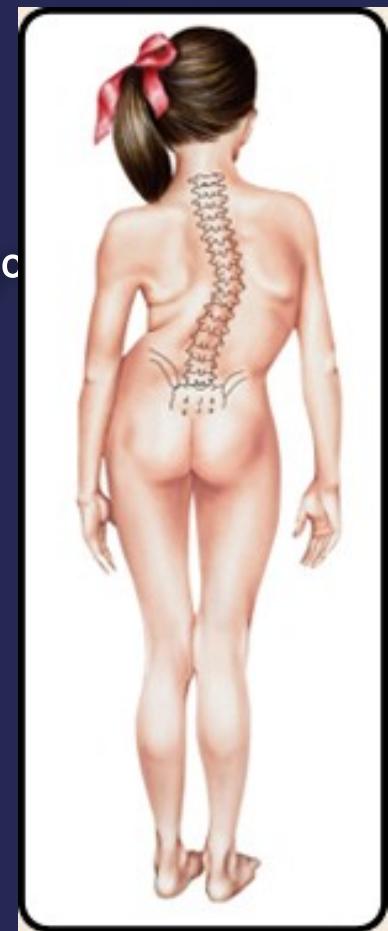
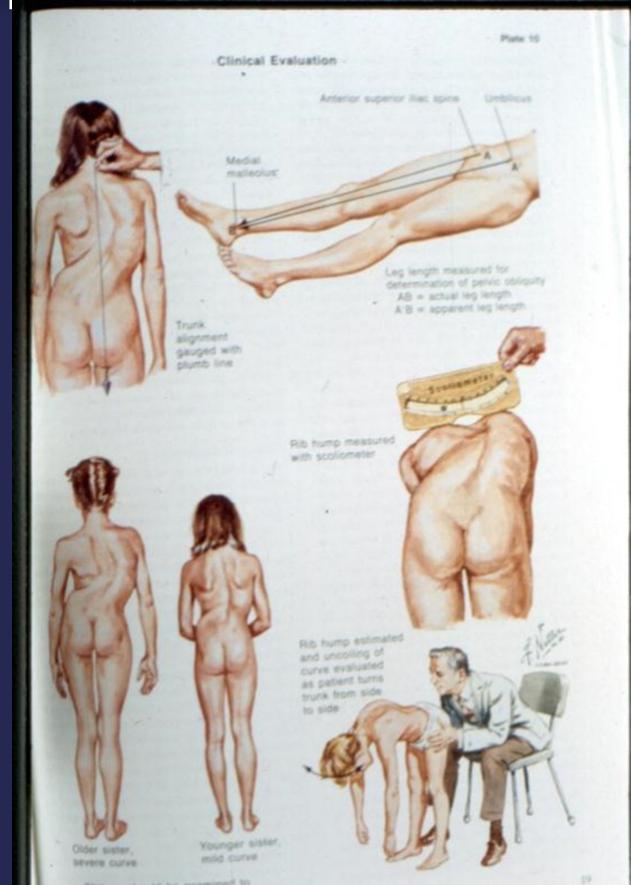
Clinical Findings
- Leaning of entire body to one side
- Head not centered directly above the pelvis
- Shoulders at different heights
- One shoulder blade more prominent than the other
- Rib cages at different heights (due to vertebral rotation)
- Uneven waist
- Raised, prominent hip
- Curve increases on forward flexion
- Compensatory scoliosis disappears on flexion


Diagnostic Measurements
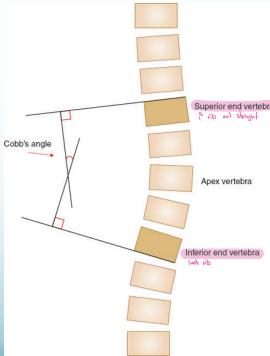
Cobb’s Angle
- Measures the amount of curve
- Angle between perpendicular lines to the uppermost and lowermost vertebral bodies in the curve

Risser’s Sign
- Measures potential for growth progression
- Ranges from 0 (no ossification) to 5 (complete bony fusion)
- Lower grade = Higher progression potential


Progression Determinants
- Patient gender: Female > Male (3:1 ratio)
- Curve magnitude: Higher curves progress more
- Future growth potential: More growth = more/quicker progression
- More growth potential = more and quicker progression
- Less growth potential = less and slower progression
- This is assessed using: Risser’s sign
Scoliosis Treatment Guidelines
Goal: Prevent curve progression
Monitoring:
- Follow-up every 6 months
- Exclude other causes (tumor, infection)
by photography, clinical evaluation and radiological measuring the curve every 4m necessary before deciding conservative or surgical treatment
Treatment Options:
| Curve Severity | Treatment Approach |
|---|---|
| <10° | No treatment needed |
| 20°-40° | Bracing (23/24 hours) |
| >40° (in skeletally immature) | Surgical intervention |
Bracing 20°-40°
- Worn 23/24 hours daily
- Compliance is crucial
- Reduces rate of progression
- Conservative approach with stretching exercises



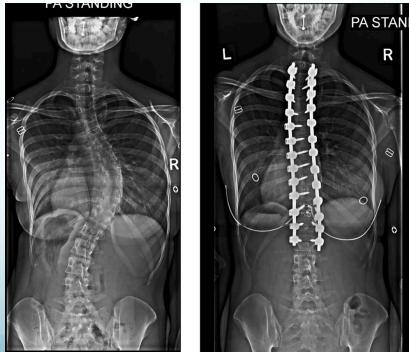
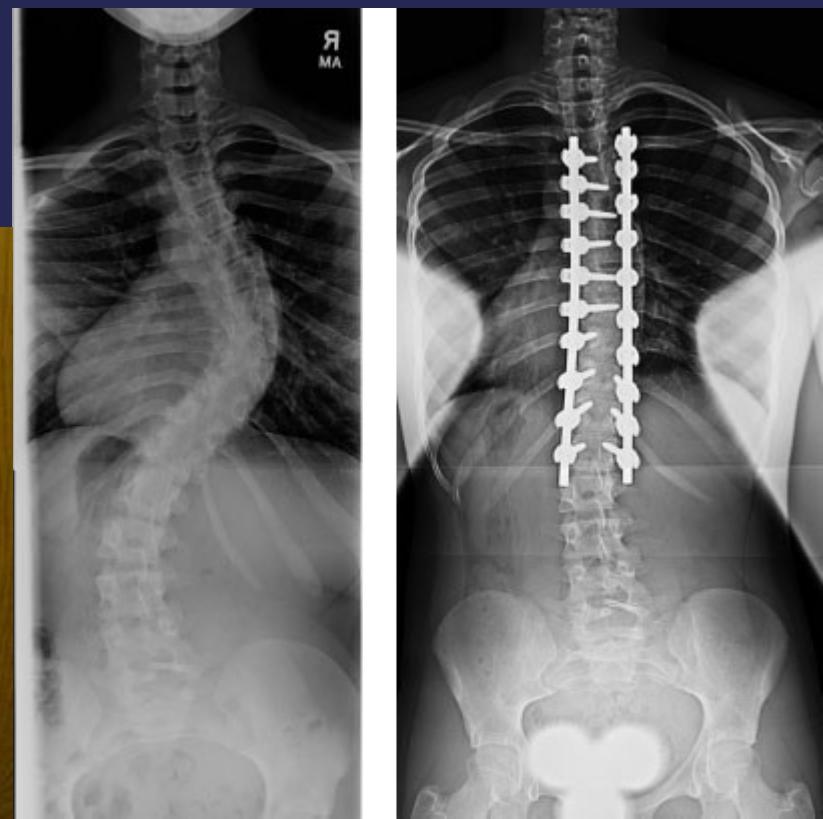
Surgical Treatment
Indications:
- Curves >40° in skeletally immature patients
- Progressive curves
Procedure:
- Correction
- Instrumentation
- Fusion


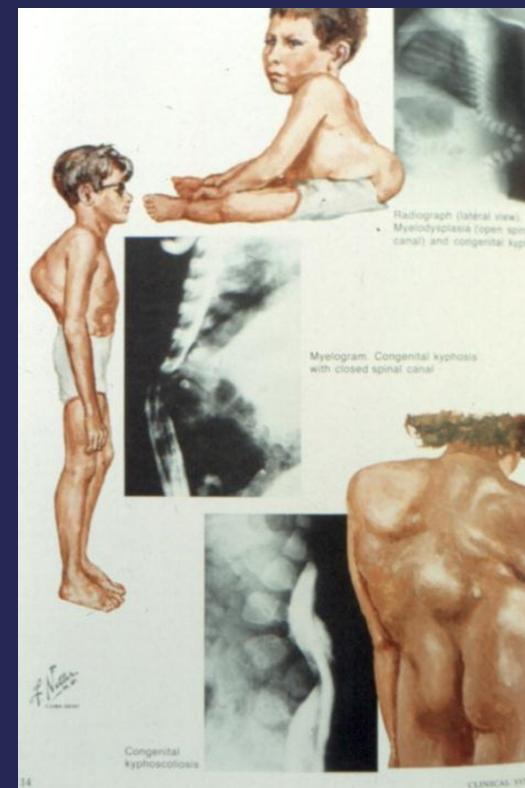
Kyphosis
Less common than scoliosis
- Kyphosis: Abnormal thoracic curve >40°
- Kyphos: Sudden angular deformity (e.g., congenital/TB)



Types of Kyphosis
- Mobile: Associated with ligament laxity
- Fixed:
- Ankylosing spondylitis
- Scheuermann’s disease (Adolescent kyphosis)
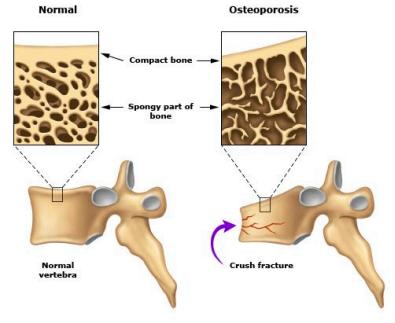
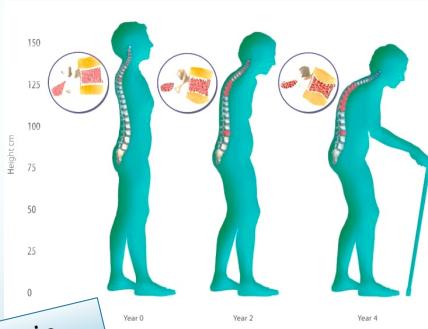
- Senile osteoporosis (Elderly patients)
Senile Osteoporosis
- Pathology: Anterior wedge compression of several vertebrae
- Result: Rounded back in elderly people
- To be discussed in “Metabolic Bone Disorders”
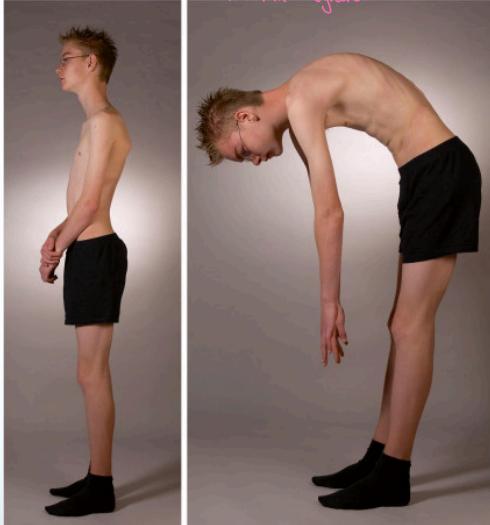
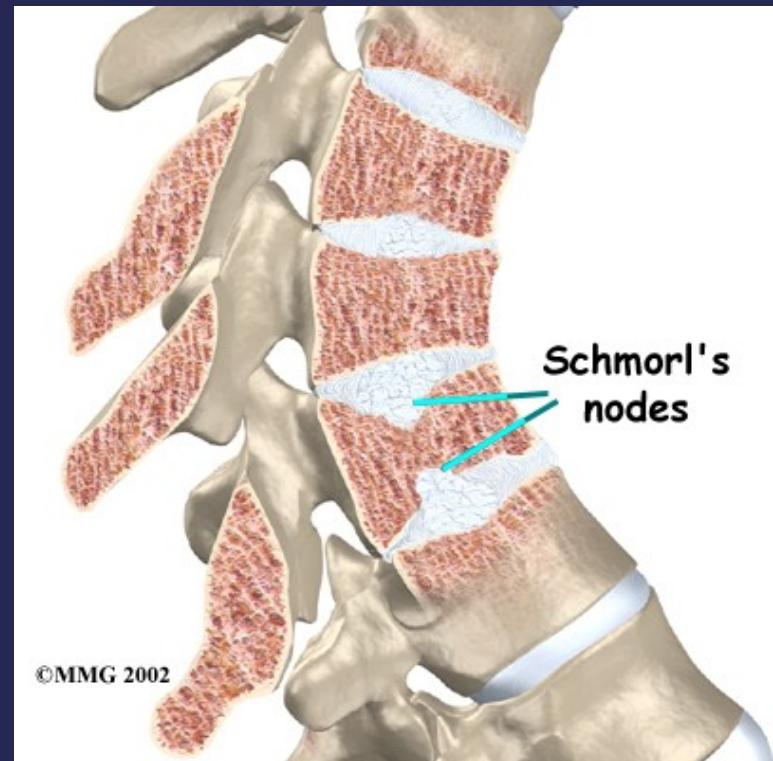
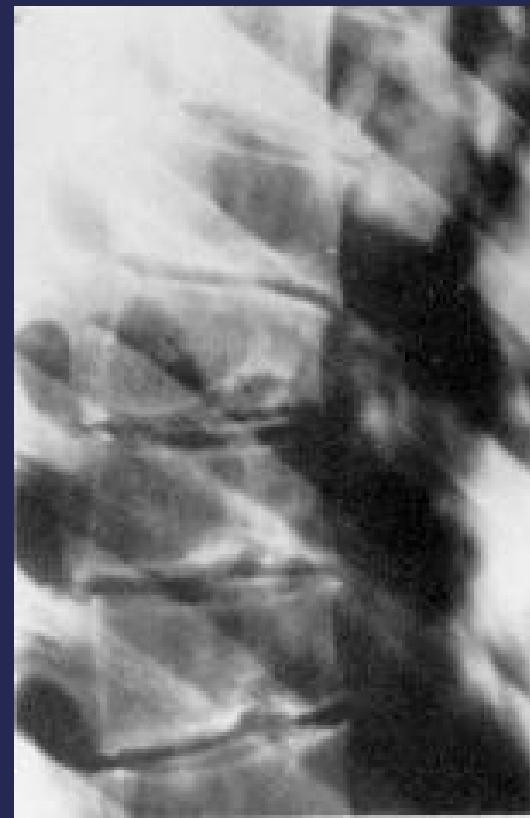
Scheuermann’s Disease
Pathology:
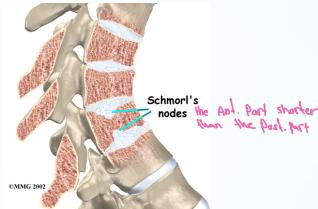
- Irregular ossification of vertebral body epiphysis
- Central herniation of disc material into the body (Schmorl’s Node)
- Wedging of vertebrae
Clinical Features:
- Developmental condition affecting teenagers
- Boys > Girls
- Gradually increasing rounded fixed kyphosis
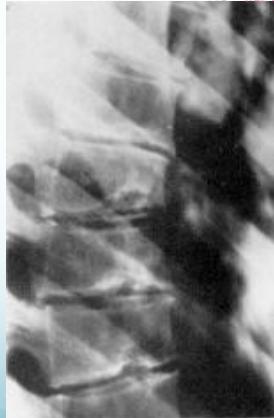
Radiographic Findings:
- Irregular ossification of vertebral body epiphysis
- Schmorl’s nodes -Central herniation of disc material into the body
- Wedging of vertebrae
Treatment:
- Mild: Reassurance
- Mild early: Bracing
- Severe: Surgery (correction & fusion)


COMBINE W/ ABOVE
Spinal Deformity
Definitions
- SCOLIOSIS: Lateral curvature of the spine >10° accompanied by vertebral rotation
- KYPHOSIS: Dorsal curvature of the spine >40°
Scoliosis
Types
Compensatory Scoliosis
- Secondary to pathology outside the spine
- Examples: Limb length discrepancy, pelvic tilt
- Disappears with sitting
Structural Scoliosis
- Fixed deformity that does not disappear with sitting
- Usually associated with bony abnormality

Structural Scoliosis Categories
- Idiopathic:
- Infantile
- Adolescent
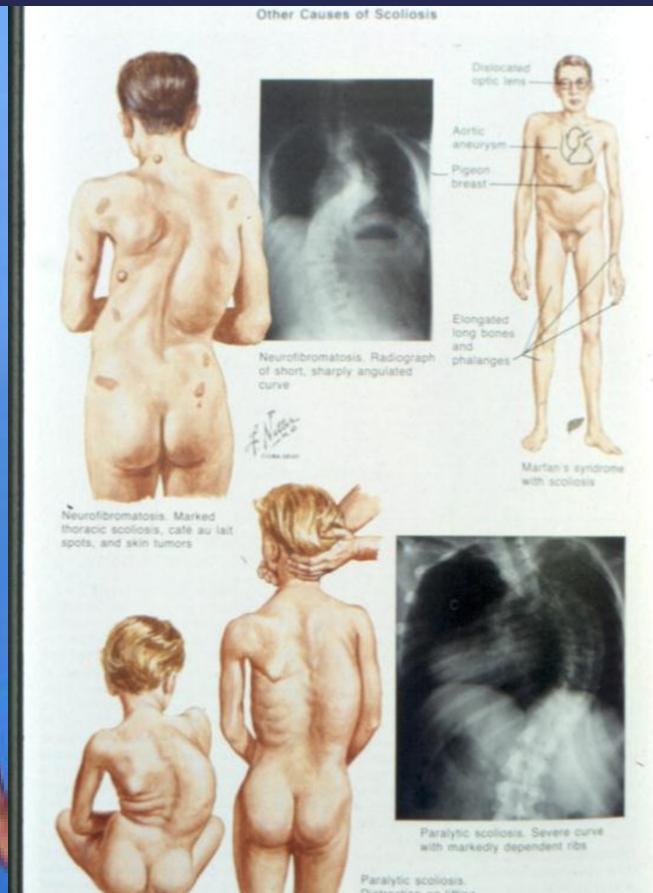
- Neuropathic (paralytic)
- Myopathy
- Neurofibromatosis
Adolescent Idiopathic Scoliosis (AIS)
Natural History
- Present in 2-4% of children aged 10-16 years
- Gender ratio: Equal for small curves (≤10°), but 10:1 female:male for curves >30°
- Progression: More common in girls (higher treatment requirement)
Clinical Features
- Shoulders at different heights – one shoulder blade more prominent
- Head not centered directly above the pelvis
- Raised, prominent hip
- Rib cages at different heights
- Uneven waist
- Skin texture changes overlying the spine
- Leaning of entire body to one side
Progression Factors
- Back pain not significantly higher in patients with scoliosis
- Curves <30° at bony maturity unlikely to progress
- Curves >50° at maturity progress 1° per year
- Life-threatening pulmonary effects occur only when curve >100°
Key Determinants of Progression
- Patient gender
- Future growth potential
- Curve magnitude at diagnosis
Growth Assessment: Risser Grading
- Measures bony fusion of iliac apophysis
- Range: 0 (no ossification) to 5 (complete bony fusion)
- Lower grade = higher progression potential

Imaging
- X-ray:
- AP and LAT of entire spine (Cobb angle measurement)
- AP pelvis (Risser grade)

Cobb Angle Measurement
- Select most tilted vertebrae above and below curve apex
- Angle between intersecting lines drawn perpendicular to superior vertebra top and inferior vertebra bottom

Treatment Guidelines
Treatment Goals
- Prevent curve progression
- Periodic evaluation through photography, clinical assessment, and radiological measurement
Treatment Indications
- No treatment for curves <10°
- Treatment initiated if:
- Skeletally immature curves <19° progress 10°/year
- Curves 20-29° progress 5°/year
Bracing
Indications:
- Curves between 20-40°
- Well-balanced double curves
- Young children awaiting surgery
- Prevention of recurrence

Surgery
Indications:
- Curves >40° in skeletally immature patients
- Adult documented progressive curves
Procedure:
- Correction
- Instrumentation
- Fusion



Kyphosis
Definition
Backward angulation above 40 degrees
Types
- Mobile:
- Compensatory
- Postural
- Structural:
- Angular (e.g., congenital, TB)
- Rounded:
- Scheuermann’s disease
- Senile osteoporosis
- Ankylosing spondylitis



Scheuermann’s Disease
Pathology
- Irregular ossification of vertebral body epiphysis
- Central herniation of disc material into the body (Schmorl’s Node)
- Wedging of vertebrae
Types
- Thoracic
- Thoracolumbar
Clinical Features
- Onset: Shortly after puberty (teenagers)
- Gender: Boys > girls
- Location: Mid-thoracic
- Presentation: Rounded shoulders, fixed rounded kyphosis


X-ray Findings
- Irregular ossification of vertebral body epiphysis
- Schmorl’s nodes (central disc herniation)
- Vertebral wedging

Treatment
- Mild cases: Often unnoticed
- Early mild cases: Bracing
- Severe cases: Surgical intervention