Initial Assessment and Management
Suspicion of Spinal Injury
Cervical Spine Indicators:
- Head injury
- Loss of consciousness
- Severe facial injuries
- Blunt injury above clavicle
- Pain/stiffness in neck/back
Thoracolumbar Spine Indicators:
- Fall from height
- Crushing accident
- High-speed deceleration
- Neurological symptoms in limbs
- Rib fractures or seat belt bruising
- Severe abdominal/pelvic injuries
Principles of Management
- Diagnosis and management go hand in hand
- Follow ATLS protocol: ABC
- Inappropriate movement & examination worsen the injury
- Must immobilize the spine if any suspicion of spinal injury
Clinical Examination
Initial Assessment
- Look: General, attitude, bruises on head, face, back
- Feel: Tenderness, swelling
- Do NOT Move: Maintain spinal immobilization

Spine Examination Protocol
- Protect spine
- Log-roll patient to see back



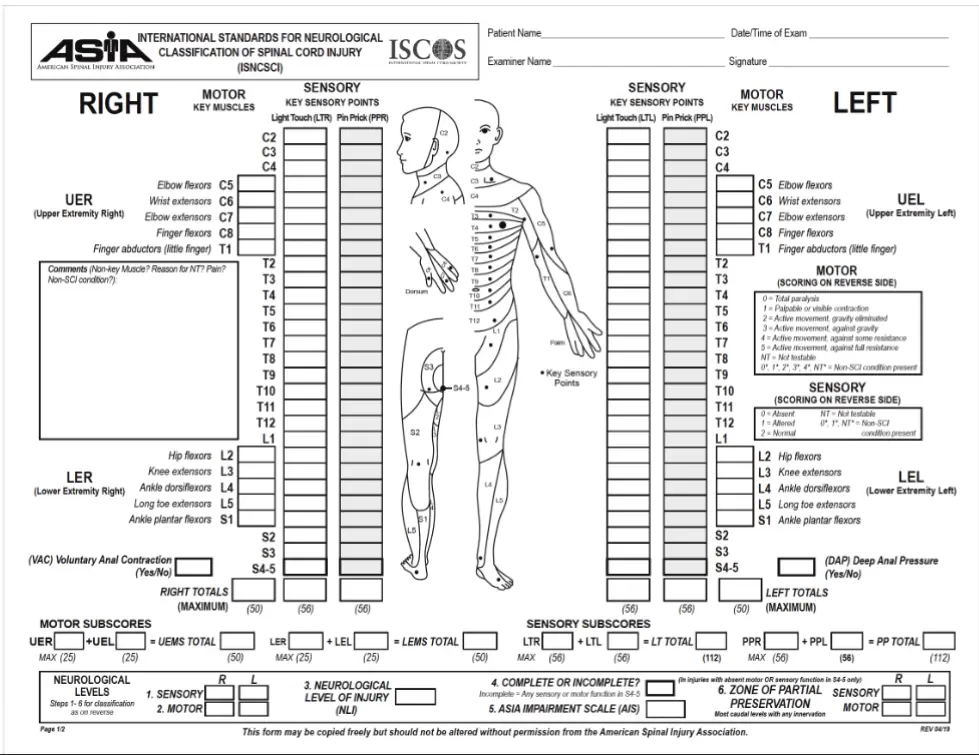
Neurological Examination
- Full neurological examination is a must
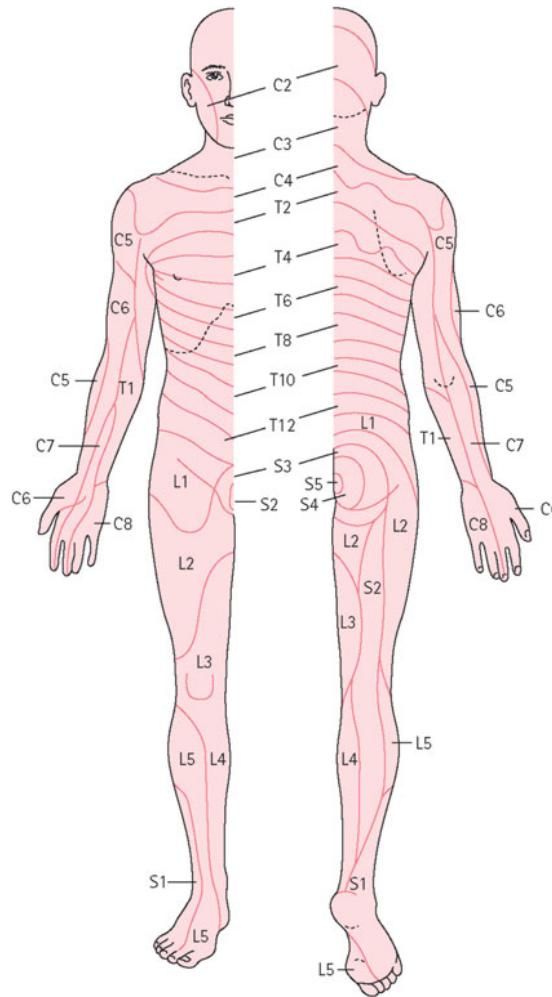
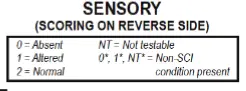
- Dermatomes
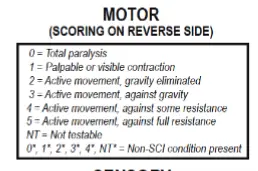
- Myotomes
- Reflexes
- To be repeated over days
Key Motor Assessment (Upper Extremity):
- C5: Elbow flexors
- C6: Wrist extensors
- C7: Elbow extensors
- C8: Finger flexors
- T1: Finger abductors (little finger)
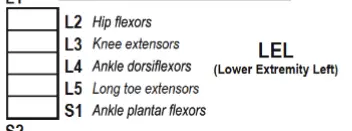
Key Motor Assessment (Lower Extremity):
- L2: Hip flexors
- L3: Knee extensors
- L4: Ankle dorsiflexors
- L5: Long toe extensors
- S1: Ankle plantar flexors
Sensory Assessment Points:
- Light touch and pin prick testing at key dermatomal levels
- Voluntary anal contraction (VAC) and deep anal pressure (DAP) assessment


Imaging Techniques
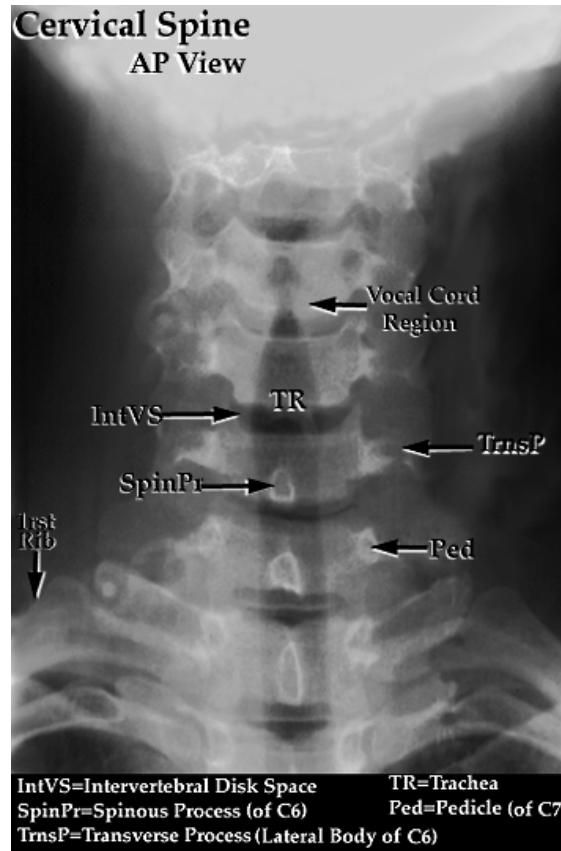
Cervical Spine Radiographs
Anteroposterior (AP) View:
- Intact lateral outline
- Spinous processes & Trachea in the middle
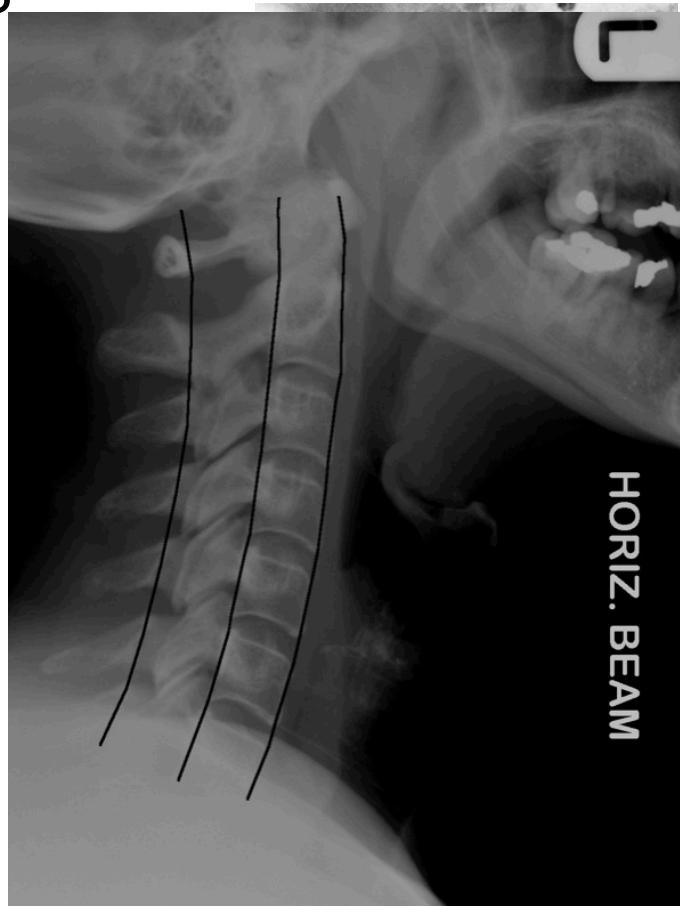
Lateral View:
- All C-vertebrae & upper T1
- Prevertebral soft tissue width
- Four parallel curves:
- Front of vertebral bodies
- Back of vertebral bodies
- Posterior borders of lateral masses
- Bases of spinous processes
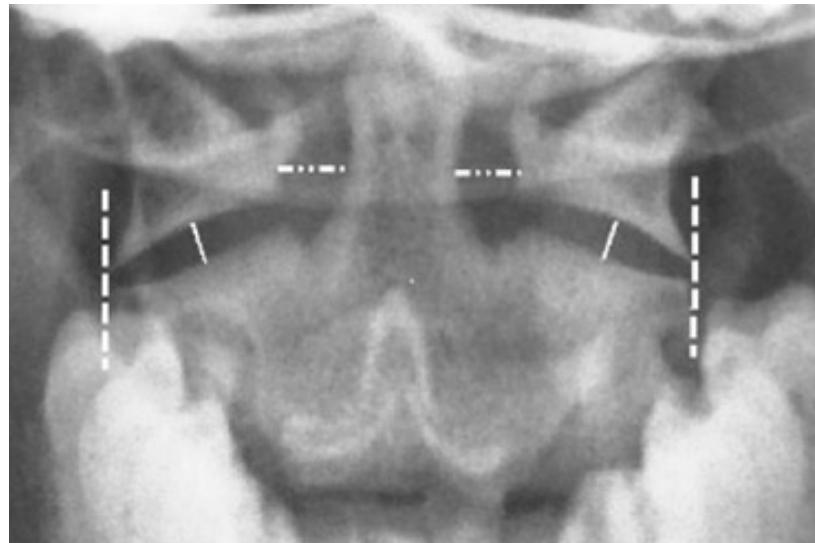
Open-mouth View:
- For C1 and C2 assessment
- Odontoid fractures
- Lateral mass fractures
- Look for: Symmetry and Continuity of bone
Treatment Approaches
Treatment Objectives
- Preserve neurological function
- Relieve reversible neural compression
- Restore alignment of spine
- Stabilize the spine
- Rehabilitate the patient
Treatment Decision Factors
- Stable/Unstable
- With/without neurological injury
Conservative Management
Indications:
- Stable without neurological injury
- Support by orthotics, rest



Surgical Management
Indications:
- Unstable with/without neurological injury
- Progressive neurological deficits
Stabilization Methods:
- Skin/Skeletal traction
- Surgery ± Decompression
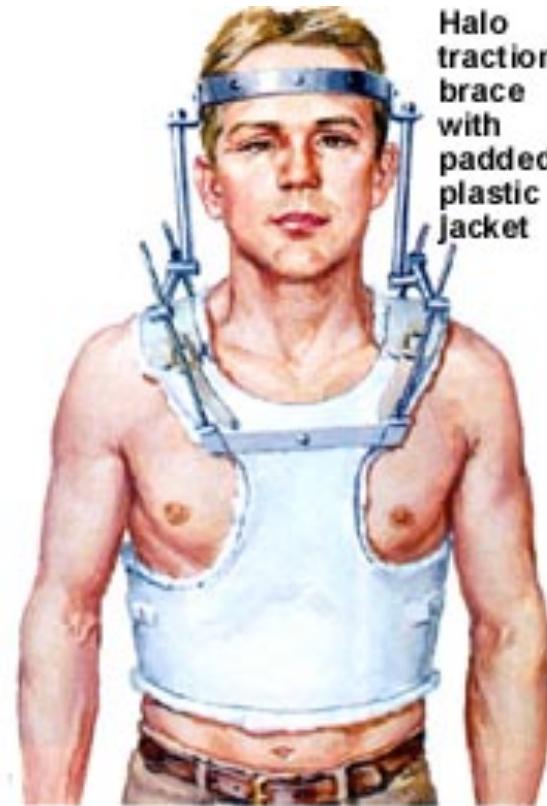
- Halo-Vest immobilization


- • Unstable With/out Neurological Injury:
- • Secure stabilization:
- • Skin / Skeletal Traction
- • Surgery +/-Decompression
Common Fracture Patterns
Anatomical Classification
- Upper cervical (C1-C2)
- Sub-axial (C3-C7)
- Thoracic
- Thoracolumbar
- Lumbar
- Sacrum
- Coccyx
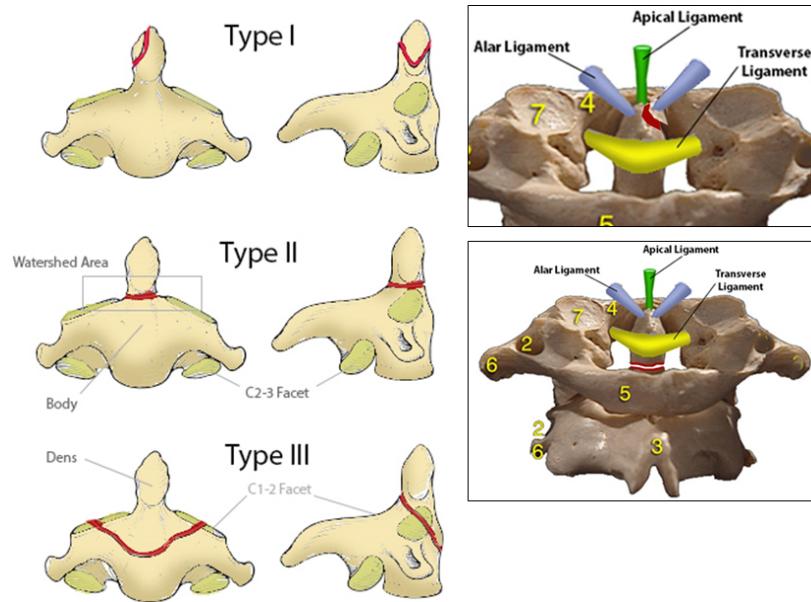
C2 Odontoid Fractures
- Seen in: Low-energy falls in elderly patients and high energy traumatic injuries in younger patients
- Diagnosis: Standard lateral and open-mouth odontoid radiographs; CT scan for difficult cases
- MRI: Rarely indicated as these fractures are usually not associated with neurologic symptoms
- Treatment: Nonoperative or operative depending on type and risk factors for nonunion
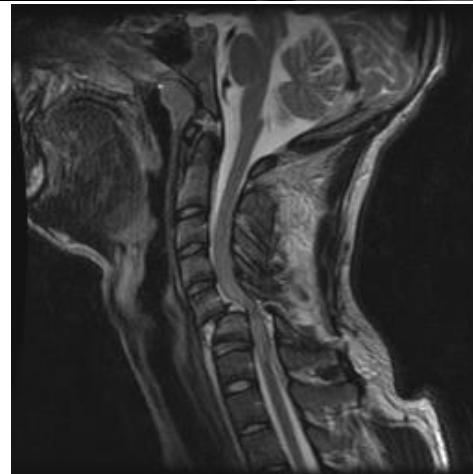
Cervical Facet Dislocations
- Spectrum of traumatic injuries with varying degrees of cervical instability and risk of spinal cord injury
- Diagnosis: Confirmed with radiographs or CT scan
- MRI: Should be performed before surgery to identify associated disk herniation
- Treatment: Closed or open reduction, followed by surgical stabilization

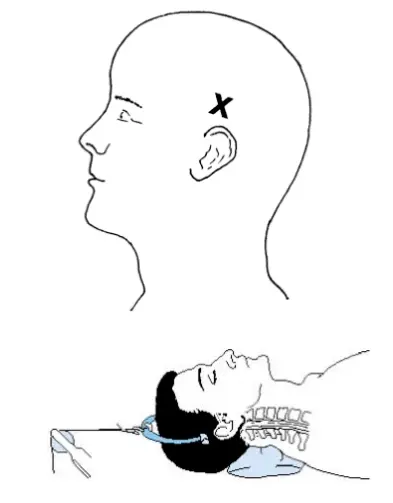
Closed Cervical Traction
maximum 70 kg traction on head
Whiplash Injury (Sprained Neck)
- Soft tissue sprain only - stable
- Mechanism: RTA rear-end collision
- Body thrown forwards, neck jerked backwards
- Pain/stiffness over 48 hours
- Treatment:
- Pain relief
- C-Collar
- Physiotherapy

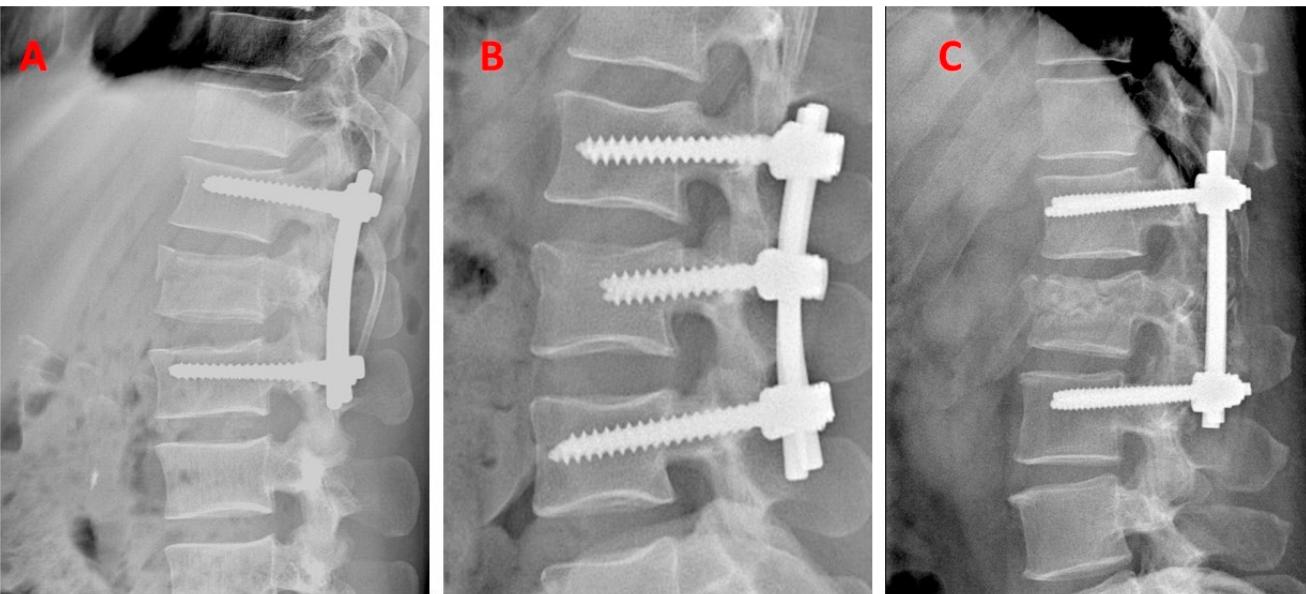
Thoracolumbar Burst Fractures
- Mechanism: High-energy traumatic vertebral fractures caused by flexion of the spine leading to compression force through the anterior and middle column
- Pathology: Retropulsion of bone into the spinal canal and compression of neural elements
- Gold standard investigation: CT scan
- Treatment: Bracing or surgical decompression and stabilization depending on neurologic deficits and instability risk

Surgical Fixation Techniques