ASCITES
Dr WAQar
MBBS, MRCP, Int. Medicine (London)
Specialist cert. exam, Endocrinology & DM (London)
ASST. PROFESSOR
Leenah Turjoman ♥
Definition
Accumulation of more than 25 cc of fluid in the peritoneal cavity is called ascites.
- Normally, only about 25 cc fluid is present in the cavity
- A little amount of fluid is needed in the cavity so there is no friction among intestines
Detection Threshold:
At least 1.5 L fluid should be present in the abdomen so as to be detected by examination. If less than this, shifting dullness and fluid thrill will be negative.
Confirmation:
- 25cc - 1.5L of fluid can be detected by US (Ultrasound)
Etiologies of Ascites
-
Liver disease (cirrhosis)
- Cancer
- Leads to lack of albumin
- So fluid goes out into interstitial spaces
- Results in ascites
- Normally, albumin keeps fluid in bed by oncotic pressure
-
Portal HTN
- Could be due to blood clot or pancreatitis
-
Low serum albumin due to any cause (cirrhosis, low protein diet, protein malabsorption, urinary albumin loss)
- e.g., nephrotic syndrome
-
Heart failure (due to backpressure)
- On the right side
- Causes hepatomegaly
- Fluid comes out
-
Renal failure (due to fluid retention)
- Leads to fluid accumulation, causing:
- Ascites
- Pleural effusion
- Pulmonary edema
- Pedal edema
- Leads to fluid accumulation, causing:
-
Peritonitis
- Infection causes all fluid to come out into peritoneal cavity
-
Mets to the peritoneum
- Peritoneum becomes inflamed and fluid comes out in the cavity
Step Wise Approach
- Take a detailed history (keeping in view all the etiologies)
- Physical examination (keeping in view all the etiologies)
- CBC, LFTs, Electrolytes, creatinine
- Ascitic fluid analysis
- Imaging studies (keeping in view all the etiologies)
Classification
Ascites can be divided into 2 main types according to the protein concentration of the fluid:
- TRANSUDATE: Protein less than 30g/L in the ascitic fluid
- EXUDATE: Protein more than 30 g/L
A better way of classification is the SAAG ratio (Serum to Ascites Albumin Gradient) - (difference)
What is SAAG?
Serum albumin minus ascitic fluid albumin (albumin difference)
- This difference can be more than 1.1g/100cc or less than 1.1g/100cc
Classification:
| SAAG Value | Category |
|---|---|
| SAAG > 1.1 | High gradient |
| SAAG < 1.1 | Low gradient |
Causes of Ascites by SAAG
SAAG > 1.1
a) Cirrhosis with/portal HTN
b) Portal HTN due to any other cause
c) Heart failure
d) Renal failure
SAAG < 1.1
a) Bacterial & fungal peritonitis
b) Tuberculous peritonitis
c) Nephrotic syndrome
d) Pancreatitis
e) Low serum albumin
f) Mets to the peritoneum
Some Other Types of Ascites
-
Hemorrhagic ascites: due to malignancy
- Either mets or malignancy of Peritoneum
-
Chylous ascites: Collection of lymph in the abdominal cavity
- Rich in fats → milky appearance
- e.g., in lymphomas, TB peritonitis
- These conditions cause damage to lymphatic channels so lymph comes out into peritoneal cavity
- Triglycerides are carried with proteins in the blood, they are not water soluble
- (Chilomicrons = Triglycerides = Fat)
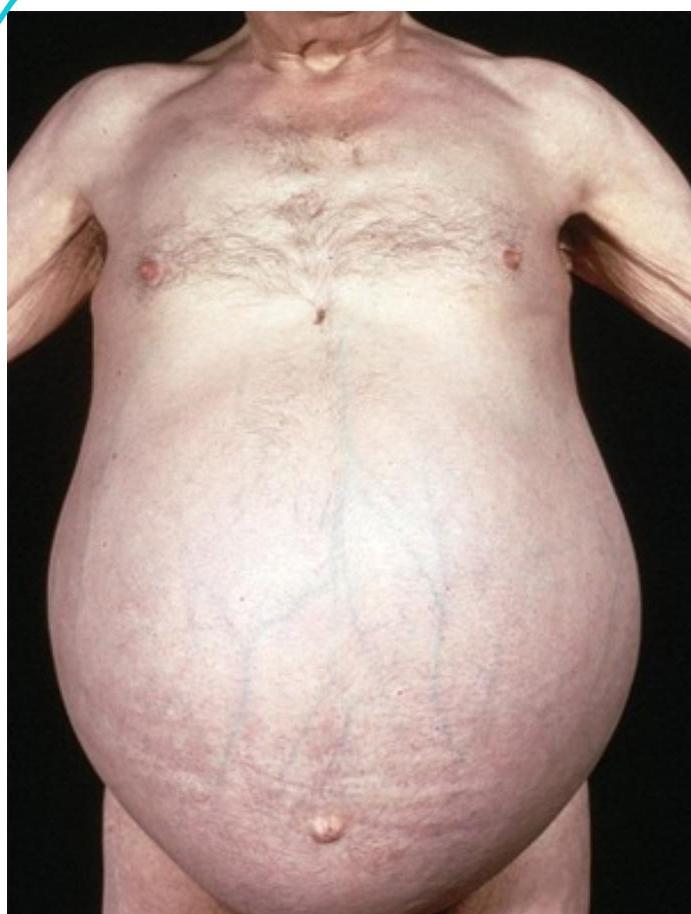
Clinical Images
Ascites
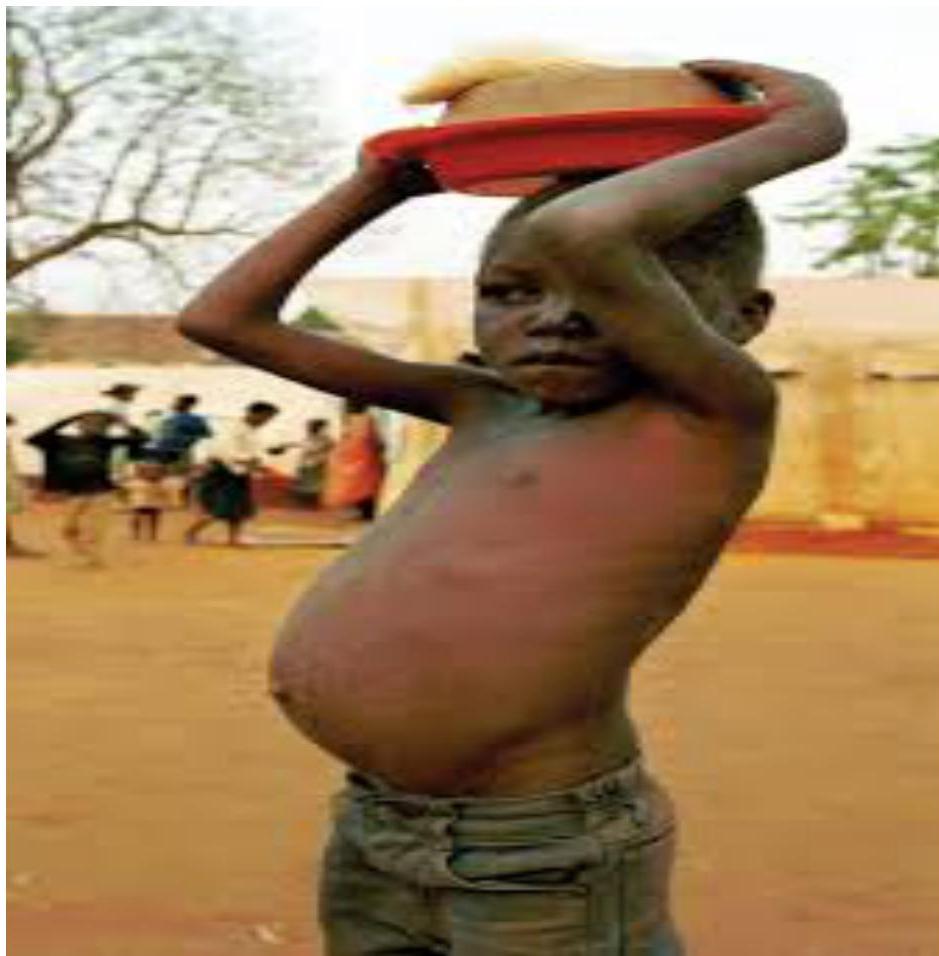
Ascites Due to Kwashiorkor
Investigations in Ascites
Paracentesis (Ascitic Tap)
Every new patient with ascites should get a “diagnostic” tap:
- Take out 10-20 cc fluid
- Check:
- Albumin (to calculate SAAG)
- Neutrophils (to see infection)
- RBC
- Gram stain & culture
- Cytology (malignant cells)
- Amylase levels (in suspected pancreatic ascites) → not routinely done
Management of Ascites
General Principles
- Low salt & Diuretics
- Water intake restriction (because salt retains water in the body)
- Paracentesis
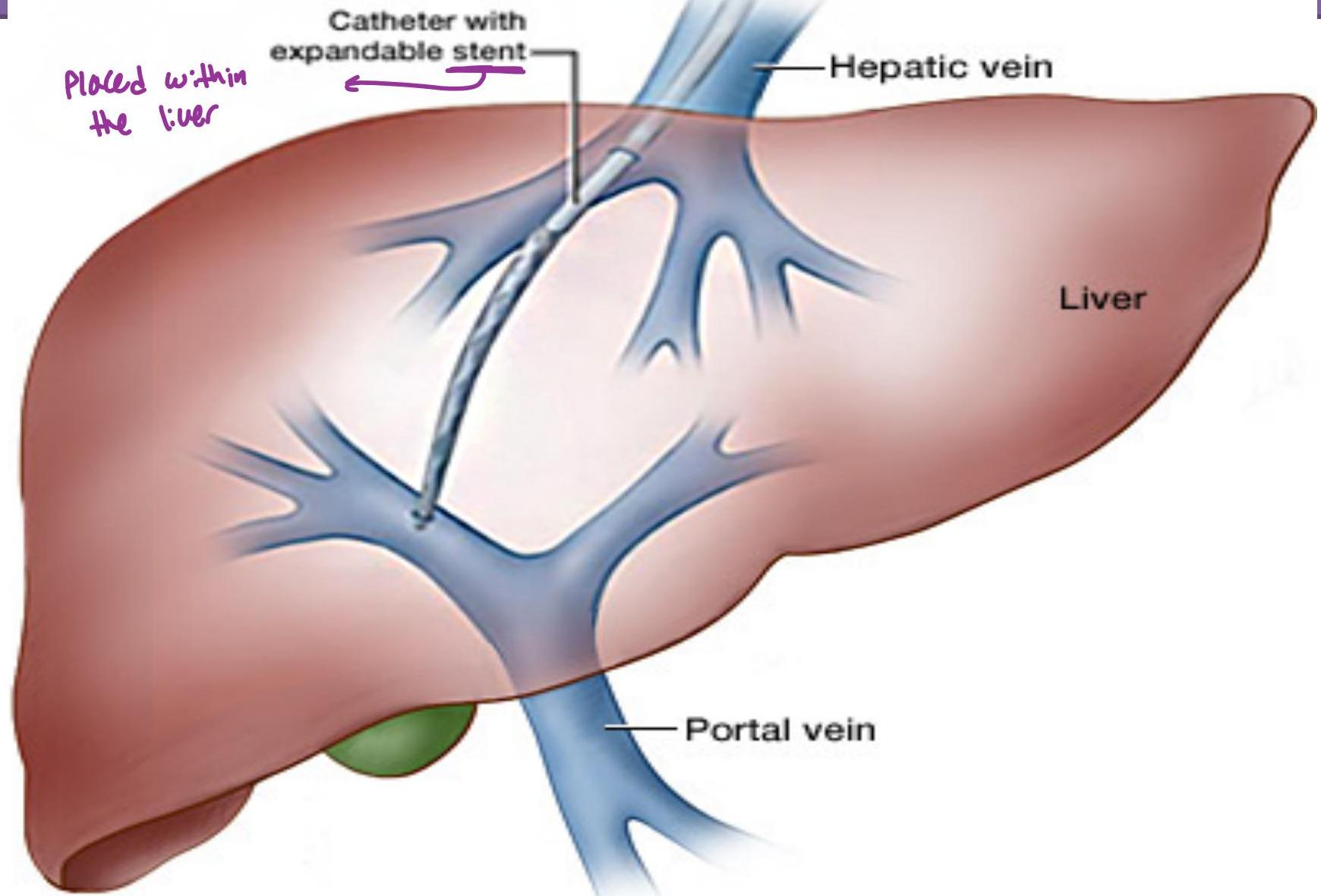
In very resistant ascites, a procedure called TIPS is sometimes used (transjugular intrahepatic porto-systemic shunt).
TIPS Mechanism: Joining Portal with hepatic circulation so pressure in Portal vein is diverted to hepatic system (reducing pressure in Portal vein)
TIPS Procedure
Medical Management
1) Low salt & water restriction
- Less than 2 g/d of salt (less than ½ teaspoon)
2) Diuretics
First Choice:
- Spironolactone (Aldactone) → in liver disease
- Side effects: gynecomastia, hyperkalemia
Additional:
- Can add Lasix (Furosemide) if needed
Important: Reduce ascites gradually (0.5 to 1 kg weight loss daily). Too much weight loss “suddenly” is not good!
In 95% of cases, ascites can be controlled by low salt & diuretics alone.
Therapeutic Paracentesis
Indication:
- Done if medicines don’t help (resistant ascites) or very big ascites causing respiratory difficulty
Procedure Details:
- Upto 7 L can be removed at one time
- Removal of more than 7L can cause problems:
- Hypotension
- Renal failure
- Encephalopathy
- Can also occur if rapidly reduce ascites by diuretics
- I.V. albumin given at the time of paracentesis can prevent these complications
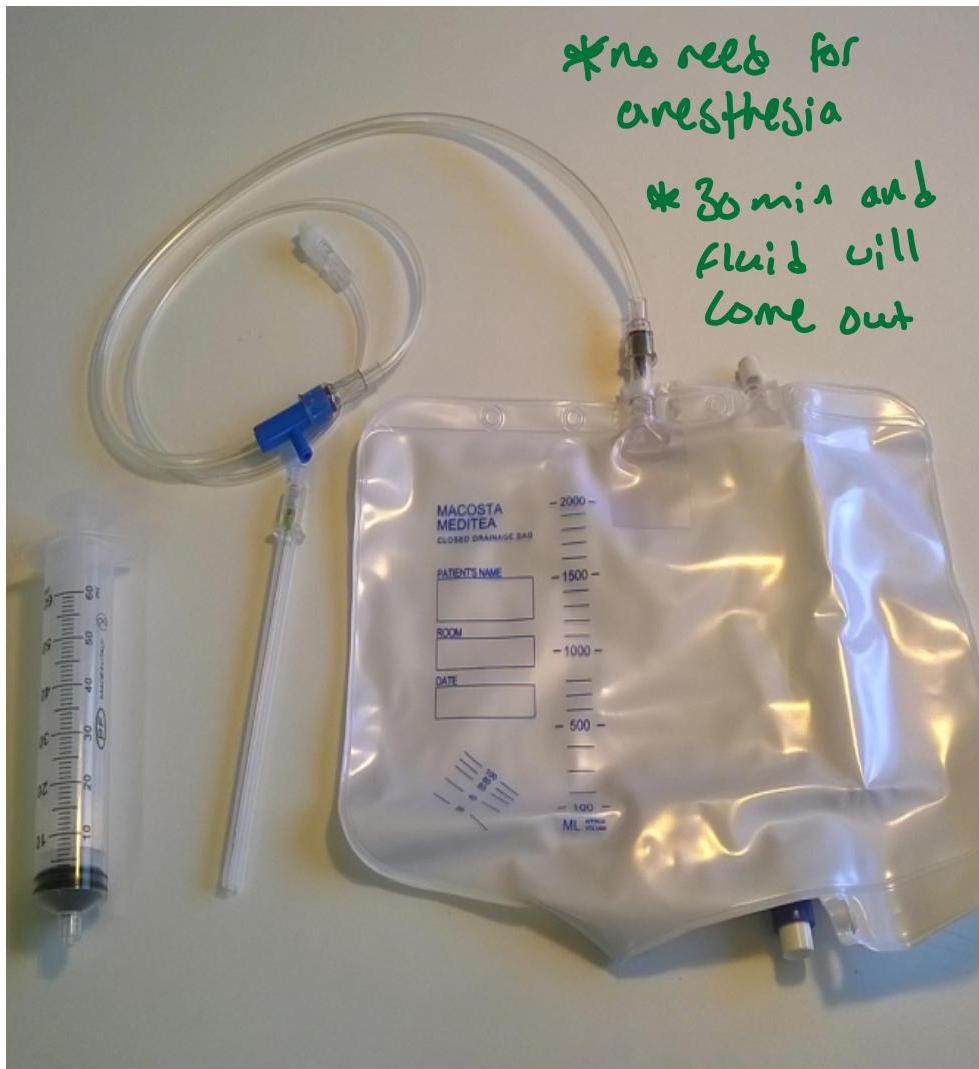
Procedure Notes:
- No need for anesthesia
- 30 min and fluid will come out

Complications of Ascites
Albumin Considerations
Patient with liver cirrhosis: albumin is not synthesized, leading to ascites, but albumin is not given as treatment because albumin has very short half life, so practically can’t be given for life.
- Albumin not given for nephrotic syndrome because if given, more albumin will be filtered through kidney and more damaging to kidney
Key Complications
Remember 3 complications of ascites:
- SBP (Spontaneous bacterial peritonitis)
- Respiratory distress
- Umbilical hernia
How to Approach the Patient
- Take a detailed history (keeping in view the causes of ascites)
- Do appropriate examination
- Order investigations
- Give treatment to remove the ascitic fluid
- Treat the cause
Summary Notes
Last slide is very important
Personal Reflection
Try to do 1 small good thing every day
- Greet people with a smile
- Give way to another car on the road
- Talk nicely to a person who is lower than you financially or in position
Merci
