DISSEMINATED INTRAVASCULAR COAGULOPATHY (DIC)
DIC is due to widespread activation of coagulation in the circulation due to severe illness resulting in: ➢ Consumption of some coagulation factors and platelets. ➢ Fibrin deposition and fibrin thrombi ➢ Secondary fibrinolysis.
Etiology
Critically ill children with:
- Severe infections (e.g., meningococcal septicemia, sepsis).
-
- Intravascular hemolysis (e.g., ABO-incompatible transfusion).
- Shock and Burns.
- Liver disease and Malignancy.
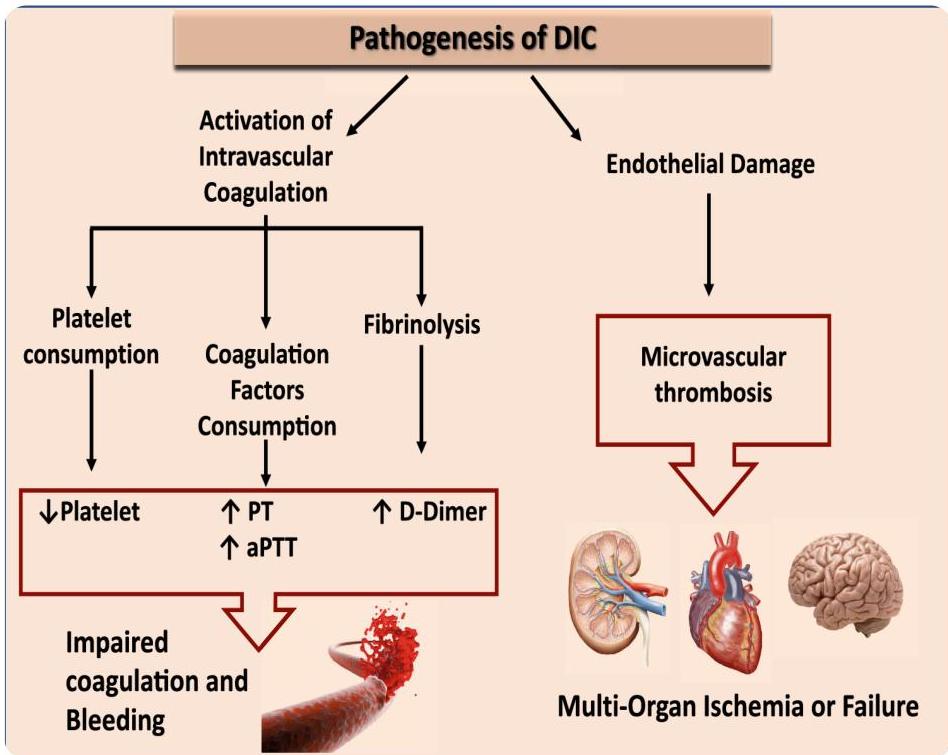
Pathophysiology
- Consumption of coagulation factors and platelets.
- Fibrin deposition and thrombi throughout the body.
- Secondary fibrinolysis.
- Organ failure due to small vessel thrombosis (lung, liver, kidney, CNS, GI, brain, pancreas) causing dysfunction of these organs.
Clinical Picture
Range of features including both bleeding and thrombosis:
- Bleeding: Venipuncture sites, GIT (melena, hematemesis), Pulmonary, Epistaxis, Hematuria, Intracranial.
- Skin: Petechiae, ecchymoses, purpura, and peripheral tissue necrosis.
- Organ Failure: Manifestations of thrombosis in vital organs.
Investigations
“Everything abnormal”:
- Prolonged PT and aPTT.
- Decreased Fibrinogen and Platelets.
- Decreased Factors V, VIII, XIII.
- Increased FDPs and D-dimers.
- Blood Smear: Helmet cells, schistocytes (evidence of microangiopathic hemolysis).
- Increased Markers: PF4 (platelet factor 4), FPA (fibrinopeptide A).
Treatment
DIC is an end-stage process with poor prognosis; management focuses on compensation:
- Treat underlying cause (e.g., sepsis).
- Intensive Care support.
- Replacement: Fresh frozen plasma, cryoprecipitate, and platelets.
- Concentrates: Antithrombin and protein C.
- Heparin: Small doses to manage microvascular thrombi.