HEMOPHILIAS
General Overview:
- Hemophilia A: Deficiency of factor VIII (commonest type).
- Hemophilia B: Deficiency of factor IX (Christmas factor).
- Hemophilia C: Deficiency of factor XI (plasma thromboplastin antecedent).
- All produce similar manifestations but differ in severity.
Hemophilia A (Classical Hemophilia)
- Most serious bleeding disorder (though VWD is most common).
- Severe hereditary coagulation disorder.
- Deficiency of factor VIII.
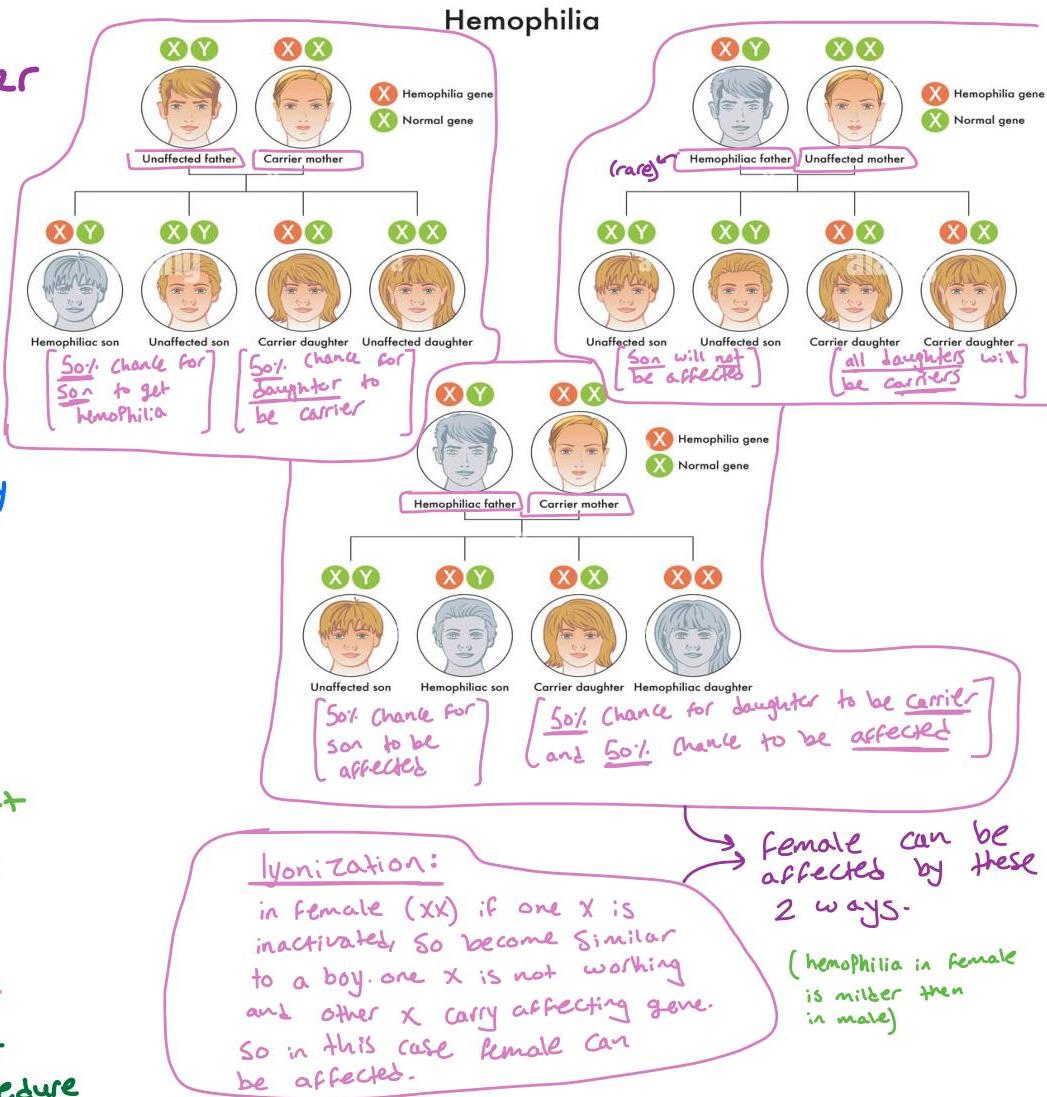
- Transmission: X-linked recessive trait (carrier female, affected male; typically from mother’s side).
- Family History: Positive in most cases, but can be de novo mutation.
Severity Classification
| Classification | Factor level (%) | Bleeding phenotype |
|---|---|---|
| Severe | <1 | Spontaneous bleeding (especially large joints) |
| Moderate | 1 - 5 | Bleeding on minor trauma |
| Mild | 6 - 40 | Bleeding on major trauma/surgery |
Clinical Picture
Can appear from very early life (median age of discovery around 10 months when crawling/walking):
- Easy bruising and large subcutaneous hematomas.
- Prolonged bleeding after circumcision or cuts.
- Newborns: Risk of intracranial hemorrhage (rare).
- Deep Hematomas: Intramuscular (e.g., calf, spinal muscles) after slight trauma.
- Mucous Membrane Bleeding: Epistaxis, dental, GIT bleeding.
- Hematuria.
- Hemarthroses (Hallmark): Bleeding into large joints (Knee, Ankle, Elbow) causing pain, swelling, and potential crippling/loss of motor function.
- Dangerous Sites: CNS (intracranial/spinal), intraocular, neck (retropharyngeal), retroperitoneal.








 deep echymosis
deep echymosis 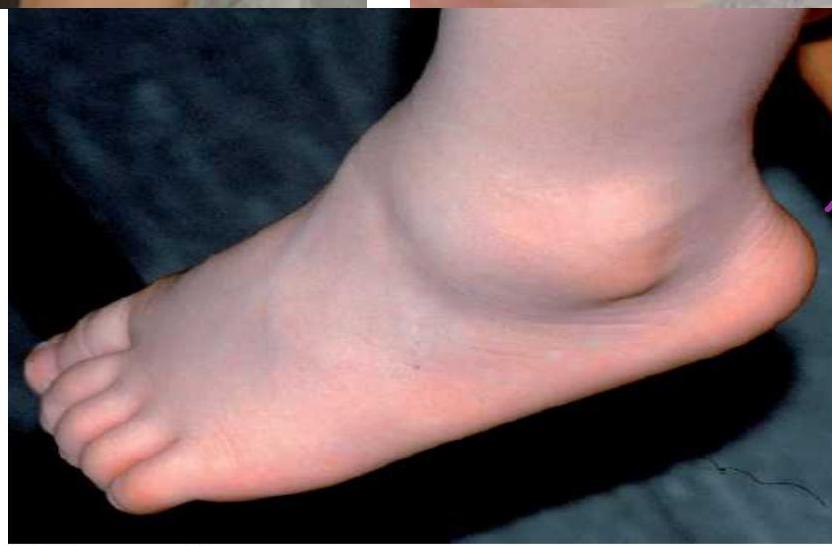 hemarthrosis in ankle -
hemarthrosis in ankle -  bracelet should be worn all the time
bracelet should be worn all the time
Investigations
- Coagulation Profile:
- Prolonged aPTT: Usually >120 seconds.
- Normal PT (intrinsic pathway affected).
- Normal Bleeding Time.
- Normal Platelet Count (CBC).
- Factor VIII Assay: Reduced level (assess degree for severity).
- Prenatal Diagnosis: Available for families with history.
- Clinical context: Large hematoma after IM vaccination.
Treatment
General Considerations:
- Prevention: Avoid trauma, wear medical bracelet at all times.
- Injections: Avoid IM; use subcutaneous, nasal, or oral routes for vaccinations.
- Blood sampling: Avoid large veins.
- Monitoring: Mother should observe for changes in joint size (early hemarthrosis).
Replacement Therapy (Factor VIII):
- Prophylactic: Regular doses to normalize hemostasis.
- Severe (<1%): 3x weekly for Hemophilia A; 2x weekly for Hemophilia B.
- Start if joint hemorrhage occurs or in mild/moderate cases with hemarthrosis.
- Active Bleeding/Surgery: Every 12 hours.
- Mild-Moderate: Raise factor to 35–50%.
- Severe/Life-threatening: Raise level to 100%.
- Products: Plasma-derived, monoclonal-antibody purified, recombinant FVIII.
Pharmacotherapy:
- Desmopressin (DDAVP): IV, SC, or intranasal. Stimulates endogenous release of FVIII:C and vWF. Sufficient for mild forms.
Multidisciplinary Care:
- Physiotherapy: Preserve muscle strength, avoid immobilization damage.
- Orthopedic: Treatment for arthritis.
- Psychological support.



Rox Factor VIII (Technical Specifications)
For qualitative changes in distribution of Factor VIII activity in plasma and Factor VIII containing hemophilia:
- 2 x Reagent 1: 0.015
- 2 x Reagent 2: 0.025
- 1 x Tris: (Kcal buffer, 1000)
- 2 x FITC: (Cytosine, 1000)
- 1 x 10^6 U/ml (pH 4.4)
- 1 x 10^6 U/ml (pH 4.4)
Hemophilia B (Christmas Disease)
- Transmission: X-linked recessive trait.
- Deficiency: Factor IX. (9)
- Manifestations: Similar to Hemophilia A but often milder.
- Treatment: Factor IX concentrate (prophylaxis 2x weekly).