Viral Hepatitis
Prepared by: Dr. Salma ElGazzar

Lecture Objectives: Acute Viral Hepatitis in Children
By the end of this lecture, you should be able to:
- ☐ Define acute viral hepatitis and recognize its significance as a cause of liver disease in children.
- ☐ Identify common viral etiologies that can cause acute hepatitis.
- ☐ Describe the typical clinical presentation of acute viral hepatitis in children.
- ☐ Outline the essential investigations for a child with suspected acute viral hepatitis.
- ☐ Discuss the general principles of management for acute viral hepatitis.
- ☐ Formulate a differential diagnosis for children presenting with jaundice and/or signs of liver involvement.
- ☐ Explain the importance of prevention, including the role of vaccinations.
- ☐ Briefly describe the typical prognosis for acute viral hepatitis.
Introduction to Viral Hepatitis
Viral hepatitis continues to be a major global health problem, though there has been significant progress in recognizing and treating infected individuals.
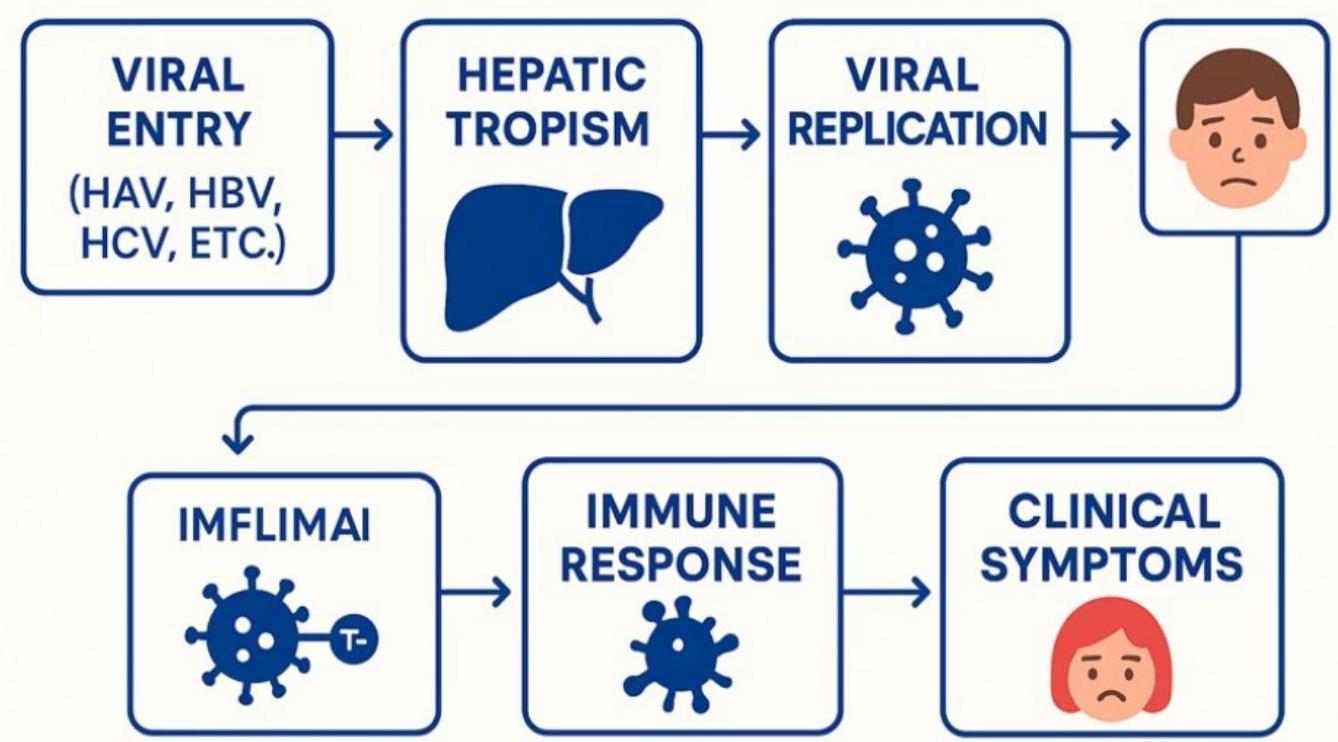
Pathogenesis of Acute Viral Hepatitis
The pathogenesis involves a complex response of the liver to hepatotropic viruses, involving either direct cytopathic effect or immune-mediated injury.
Direct Cytopathic and/or Immune-Mediated Injury
The liver’s acute response involves either direct damage to liver cells or an injury mediated by the body’s immune system.
Widespread Liver Involvement
The entire liver is affected. Necrosis (cell death) is typically most prominent in the centrilobular areas. An acute mixed inflammatory infiltrate is present, predominantly in the portal areas, but also extends into the lobules.
 Pathogenesis of Acute Viral Hepatitis in Children
Pathogenesis of Acute Viral Hepatitis in Children
Cellular and Architectural Changes
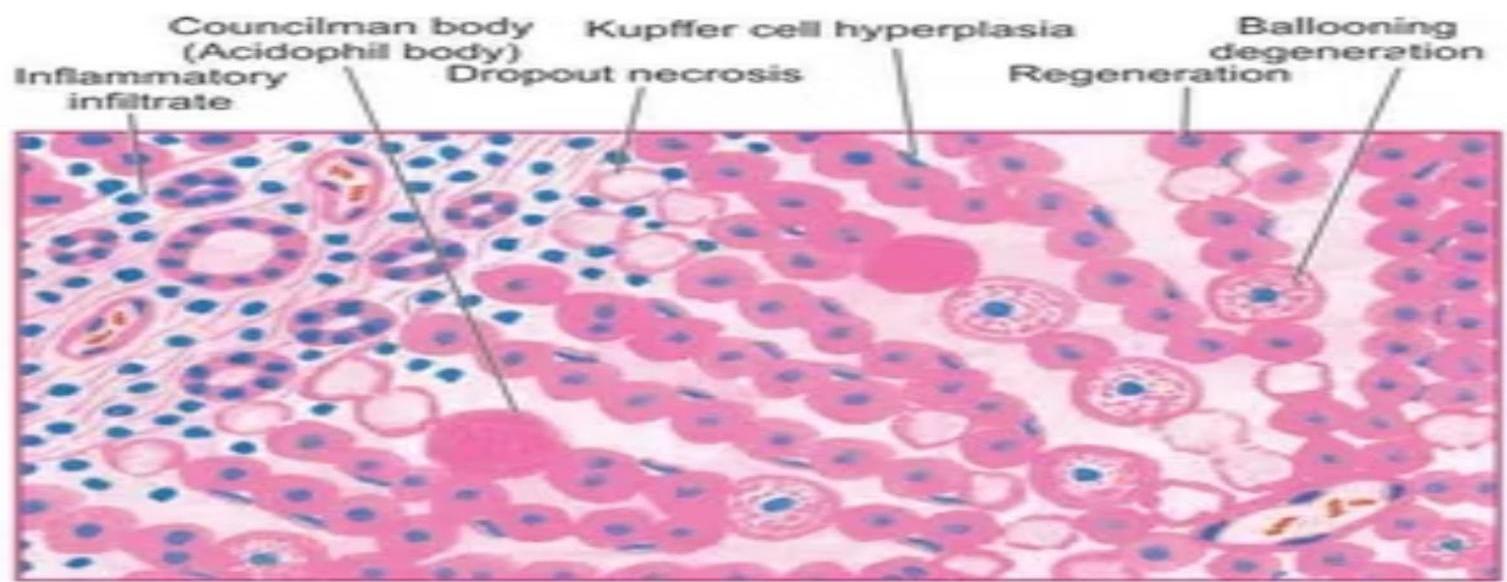
- Lobular architecture: Generally remains intact during the acute phase.
- Balloon degeneration: Common, alongside necrosis of individual or groups of parenchymal cells.
- Fatty change: Rare.
- Bile duct proliferation: Common, although damage to the bile ducts is not.
- Kupffer cell hyperplasia: Diffuse hyperplasia is noticeable in the sinusoids.
- Fulminant hepatitis: Parenchymal collapse occurs.
Prognosis and Recovery
- Recovery: Liver morphology typically returns to normal within 3 months.
- Chronicity: Persistent inflammatory infiltrate in periportal areas often leads to progressive scarring.
- Fulminant hepatitis: Characterized by parenchymal collapse.
Clinical Manifestations of Acute Viral Hepatitis
Hepatotropic viruses result in similar acute clinical illnesses.
- Asymptomatic/Mild illness: Common, especially in young children (HAV, HBV, HCV).
- Anicteric illness: Infection without jaundice (icterus) is frequent.
Common Symptoms of Acute Infection
Acute Symptoms:
- Jaundice
- Nausea, vomiting
- Abdominal pain
- Dark urine
- Joint pain
- Low/no appetite
- Fatigue
- Liver failure (rare)
Acute Histopathology:
- Ballooning degeneration
- Spotty necrosis
- Mononuclear cells
- Councilman bodies
Hepatitis A & E (Acute Only)
- Transmission: Fecal-oral route, contaminated water.
- Carrier state: None.
- Nature: Typically mild & self-limiting.
- Hepatitis E Specifics: High mortality in pregnant women.
- Malaise, Abdominal pain, Nausea, Vomiting, and Diarrhea.
- These non-specific systemic symptoms are often followed by jaundice.
Presentations
General Investigations & Management
Essential Investigations
- Liver Function Tests (LFTs): ALT, AST, GGT, Albumin.
- Bilirubin: Total and conjugated (>20% conjugated is significant).
- Viral Serology/PCR: As indicated by clinical suspicion.
- Coagulation Screen: PT/INR is critical for identifying severe dysfunction.
- Full Blood Count (FBC).
- Imaging: Abdominal ultrasound to assess liver and biliary tree.
Principles of Management
- Supportive Care: Fluid and nutritional management.
- Monitoring: Close observation for encephalopathy and coagulopathy (indicators of liver failure).
- Specialist Consultation: Required for regional liver units or ID teams.
Primary Hepatotropic Viruses
| Hepatitis A virus (HAV) | Hepatitis B virus (HBV) | Hepatitis C virus (HCV) |
|---|---|---|
| Hepatitis D virus (HDV) | Hepatitis E virus (HEV) |
Characteristics of Hepatitis Viruses
| Characteristic | Hepatitis A Virus | Hepatitis B Virus | Hepatitis C Virus | Hepatitis D Virus | Hepatitis E Virus |
|---|---|---|---|---|---|
| Nucleic acid | RNA | DNA | RNA | * | RNA |
| Serologic diagnosis | IgM anti-HA | HBsAg | Anti-HCV | Anti-HDV | Anti-HEV |
| Major transmission | Fecal-oral | Blood | Blood | Needle | Water |
| Incubation period (days) | 15–50 | 40–180 | 20–120 | 30–180 | 14–60 |
| Epidemics | Yes | No | No | No | Yes |
| Chronicity | No | Yes | Yes | Yes | No |
| Liver cancer | No | Yes | Yes | Yes | No |
Table 406.3 Diagnostic Blood Tests: Serology and Viral Polymerase Chain Reaction
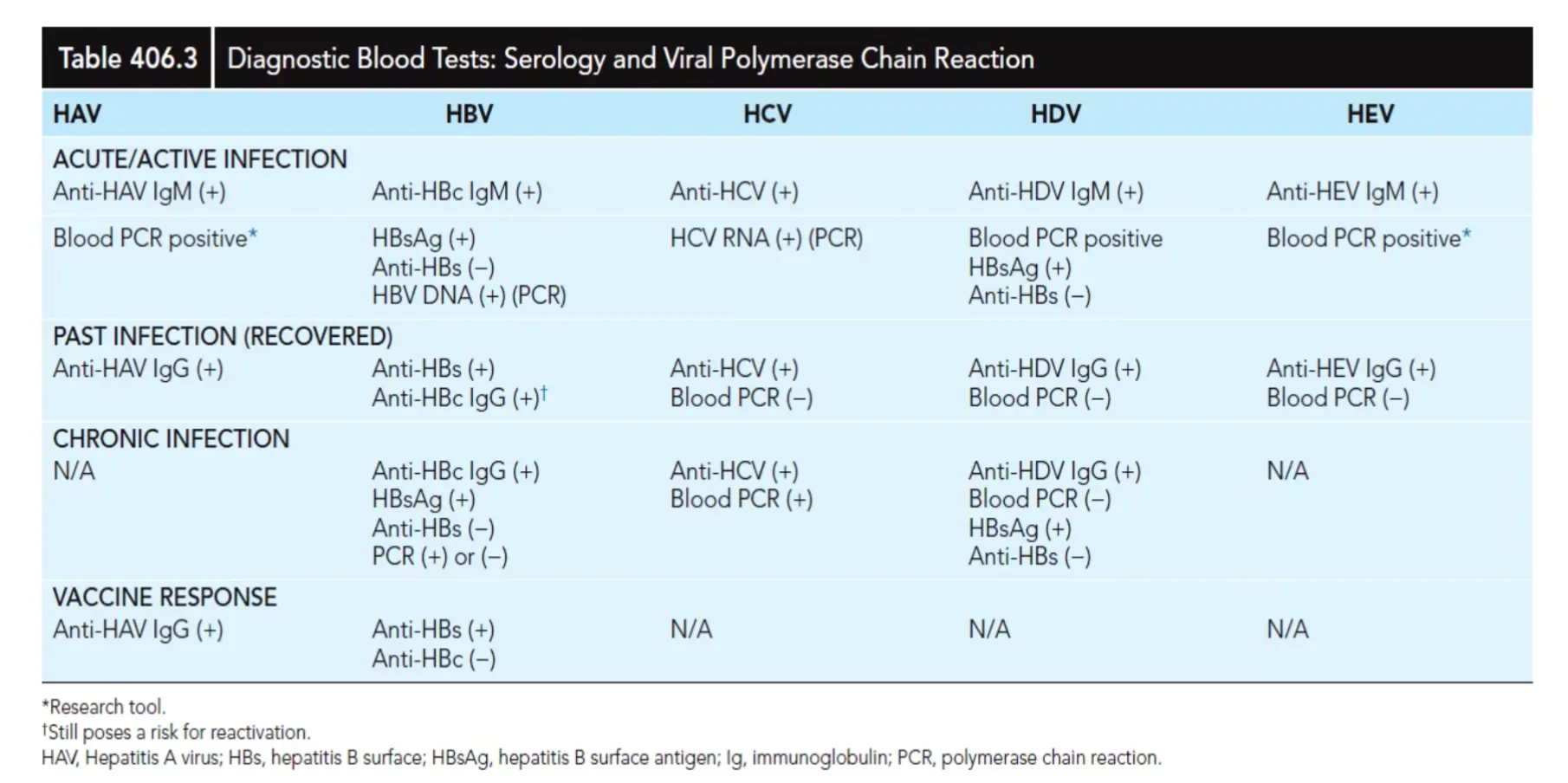
| HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|
| ACUTE/ACTIVE INFECTION | ||||
| Anti-HAV IgM (+) | Anti-HBc IgM (+) | Anti-HCV (+) | Anti-HDV IgM (+) | Anti-HEV IgM (+) |
| Blood PCR positive* | HBsAg (+) | HCV RNA (+) (PCR) | Blood PCR positive | Blood PCR positive* |
| Anti-HBs (-) | HBsAg (+) | |||
| HBV DNA (+) (PCR) | Anti-HBs (-) | |||
| PAST INFECTION (RECOVERED) | ||||
| Anti-HAV IgG (+) | Anti-HBs (+) | Anti-HCV (+) | Anti-HDV IgG (+) | Anti-HEV IgG (+) |
| Anti-HBc IgG (+)† | Blood PCR (-) | Blood PCR (-) | Blood PCR (-) | |
| CHRONIC INFECTION | ||||
| N/A | Anti-HBc IgG (+) | Anti-HCV (+) | Anti-HDV IgG (+) | N/A |
| HBsAg (+) | Blood PCR (+) | Blood PCR (-) | ||
| Anti-HBs (-) | HBsAg (+) | |||
| PCR (+) or (-) | Anti-HBs (-) | |||
| VACCINE RESPONSE | ||||
| Anti-HAV IgG (+) | Anti-HBs (+) | N/A | N/A | N/A |
| Anti-HBc (-) |
*Research tool. †Still poses a risk for reactivation. HAV, Hepatitis A virus; HBs, hepatitis B surface; HBsAg, hepatitis B surface antigen; Ig, immunoglobulin; PCR, polymerase chain reaction.
Other Viruses That Can Cause Hepatitis
- Herpes simplex viruses (1, 2, 6a, 6b)
- Cytomegalovirus (CMV)
- Epstein-Barr virus (EBV)
- Varicella-zoster virus (VZV)
- HIV
- Rubella
- Measles
- Adenoviruses
- Adeno-associated virus
- Enteroviruses
- Parvovirus B19
- Arboviruses
- Potentially SARS-CoV-2