Hepatitis A (HAV)
Definition and Etiology
Hepatitis A virus is responsible for most forms of acute and benign hepatitis. It is a member of the picornavirus family and contains RNA. It is heat-stable and primarily infects humans and other primates.
Epidemiology and Transmission
- Prevalence: Global, especially in developing countries.
- Transmission: Person-to-person via the fecal-oral route.
- Incubation period: 15–50 days.
- Communicability: Highest 1 week before and after the onset of symptoms. Fecal viral excretion is prolonged in infants.
Risk Factors:
-
Contact with infected persons.
-
International travel to areas with poor hygiene.
-
Childcare centers.
-
Foodborne outbreaks.
-
Perinatal transmission: Rare; pregnancy does not generally increase complications for the mother or newborn.
Clinical Manifestations of HAV
- Age correlation: Often asymptomatic or mild in children <5 years. Older adolescents and adults are more likely to be symptomatic.
- Symptoms: Often resemble viral gastroenteritis; can be anicteric.
- Duration: Typical illness lasts 7–14 days.
Diagnosis of HAV
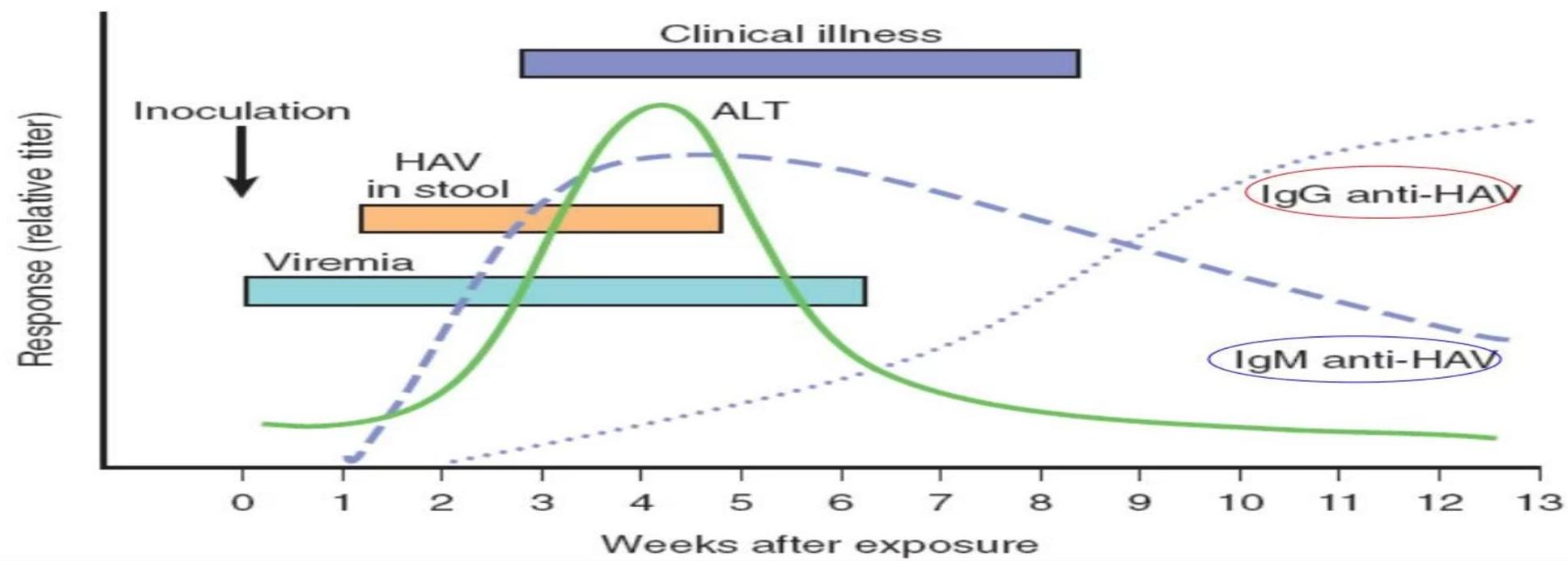
- Acute Infection: Detected via anti-HAV IgM. Detectable at symptom onset and remains positive for 4–6 months.
- Past Infection/Immunity: Anti-HAV IgG is detected within 8 weeks and confers long-term protection.
- Viral PCR: Commercially available.
- LFTs: Elevated transaminases (ALT/AST), bilirubin, alkaline phosphatase, 5’-nucleotidase, and γ-glutamyl transpeptidase (non-specific).
Complications and Treatment
- Complications: Full recovery is typical. Fulminant hepatic failure (ALF) is rare (more common in adults/immunocompromised). Prolonged cholestatic syndrome may occur.
- Treatment: No specific treatment. Supportive care (fluid and nutritional management) is the cornerstone.
- Pruritus: Antipruritic agents for cholestasis.
- Vitamins: Fat-soluble vitamin supplementation if needed.
- Avoid: Acetaminophen, as it can exacerbate liver damage.
- Note: Corticosteroids offer no benefit.
Prevention and Prognosis
- Prognosis: Excellent, with no long-term sequelae and lifelong immunity. No risk of chronic infection.
- Vaccination: Universal vaccination recommended for all children. Booster dose ≥6 months after the initial dose. Preferred over Ig for pre/post-exposure in those ≥12 months.
- Immunoglobulin (Ig): Used for travelers <6 months or those allergic to vaccines.

General Infection Control:
- Handwashing: Essential after diaper changes and before handling food.
- School Exclusion: From 2 weeks before to ~7 days after jaundice onset.
- Hospital Precautions: Contact and standard precautions for 1 week after symptom onset.
IM
HEPATITIS A
Key Features
- Most common cause of acute viral hepatitis.
- Causes only acute hepatitis. No carrier state or chronic hepatitis. Usually, does not happen twice.
Transmission
- Fecal-oral route: Contamination of food and water due to poor hygiene by food handlers.
- Saliva of the infected person also contains the virus but in very small amounts.
Clinical Features
Prodromal Phase (Initial 1-2 weeks)
- Anorexia (loss of appetite)
- Nausea
- Malaise (general feeling of discomfort)
- Bad taste in the mouth
- Fever
- Jaundice is absent initially
Icteric Phase (Next 3-6 weeks)
- Jaundice (yellowing of skin and eyes)
- Pain in the right upper quadrant of the abdomen
- Dark urine
- Pale stools
- Tender hepatomegaly (enlarged liver)
Severity of Hepatitis A
- Asymptomatic: Usually in children
- Mild to Moderate Symptoms: Most cases
- Fulminant Hepatic Failure: Rare but serious complication
Investigations
- Liver Function Tests (LFTs):
- High bilirubin (mainly direct bilirubin)
- AST & ALT are very high
- Alkaline Phosphatase slightly high
- Urine: Contains bilirubin
- Diagnostic Test: Hepatitis A antibody (anti-HAV)
Treatment
- No specific drug treatment. The disease is self-limited and usually results in complete recovery within 3 months.
- Strict isolation of the patient is not advised, but they should wash their hands thoroughly after defecation.
- Good nutrition: Eat whatever can be tolerated.
- Vitamin supplements
- Avoid alcohol and hepatotoxic drugs
- Symptomatic treatment
Prevention
- General Measures:
- Good hygiene
- Drink bottled water in high-risk areas
- Avoid risky foods
- Immunization: Hepatitis A vaccine is recommended for:
- Patients with other chronic liver disease
- Patients traveling to a high-risk area for a long time
Rapid Fire Questions (Hepatitis A)
- Mode of transmission of Hep A? fecal oral
- Which test is diagnostic? anti-HAV
- In hepatitis, which type of bilirubin is elevated predominantly? Direct
- Which specific drug is used for Hep A treatment? no specific drug
- Who should get the Hep A vaccine? High risk area for CHD
- How to avoid getting infected? avoid risk factors
- A man tells you that he had Hep A 2 years ago. Now he is jaundiced. The doctor tells him that he has Hep A re-infection. Is the doctor right? no, antibodies protective for life
Thera
Transmission:
- Fecal-oral: contaminated water or food (raw shellfish).
- Anal oral sex.
- Parenteral (not common).
Pathogenesis:
- hepatocytes destruction by the immune system,
- (the virus is not cytopathic).
Clinical features:
- Right upper quadrant pain, tender hepatomegaly, fever, malaise, anorexia, nausea, vomiting, jaundice (dark urine and pale stools), pruritus.
- Mortality rate is 0.1–0.3%.
Diagnoses:
- Antigens detection in stool.
- RNA detection in stool & blood samples by rt-PCR.
- Anti-HAV IgM in serum.
- IgM - Currently infected
- IgG - infected before
Treatment
- Generally self-limited.
- Symptomatic treatment: antiemetics, rehydration.
- Use medications that are metabolized by the liver with caution (e.g., acetaminophen “paracetamol”).
Prevention:
- Inactivated vaccine.