DIZZINESS & VERTIGO IN PRIMARY CARE
Objectives
- Explain the patho-physiology of human balance system
- Compare and contrast dizziness and vertigo
- Recognize the common causes of dizziness / vertigo
- Take an adequate history from a dizzy patient
- Perform Hallpike and Epley’s manoeuvres on a dizzy patient
- Identify the RED flag and ask for appropriate lab investigation in a dizzy patient
- Justify the differential diagnosis of dizziness
- Discuss the available therapeutic options at primary care level and criteria for referral to the secondary care
Definitions
Incidence/Prevalence
- Studies into dizziness indicated that around 30% of patients were found to have vertigo, rising to 56.4% in an older population.
- A GP can therefore expect between 10-20 patients with vertigo in one year.
- 93% of primary care patients with vertigo have either benign paroxysmal positional vertigo (BPPV), acute vestibular neuritis, or Ménière’s disease.
Common Causes in General Practice
- 80%: Vestibular Neuritis or BPV
- 15%: Meniere’s disease or Vertebrobasilar insufficiency
- 3%: Transient Ischemic Attack (TIA)
- 1%: Ear Infections
- 1%: Other causes, including Multiple sclerosis, Psychological causes e.g. Anxiety
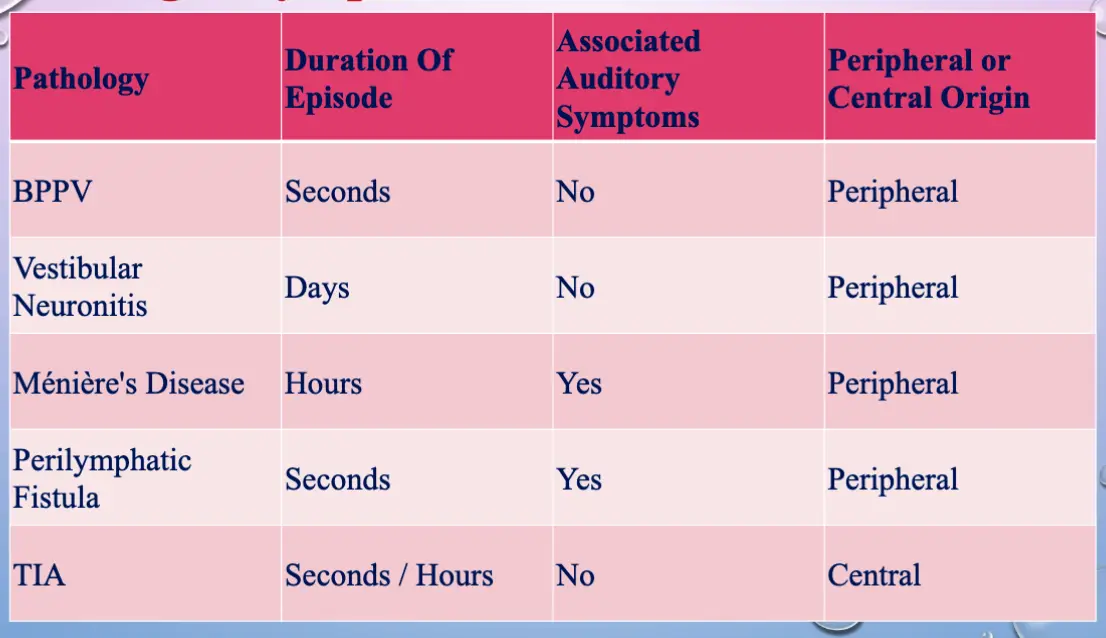
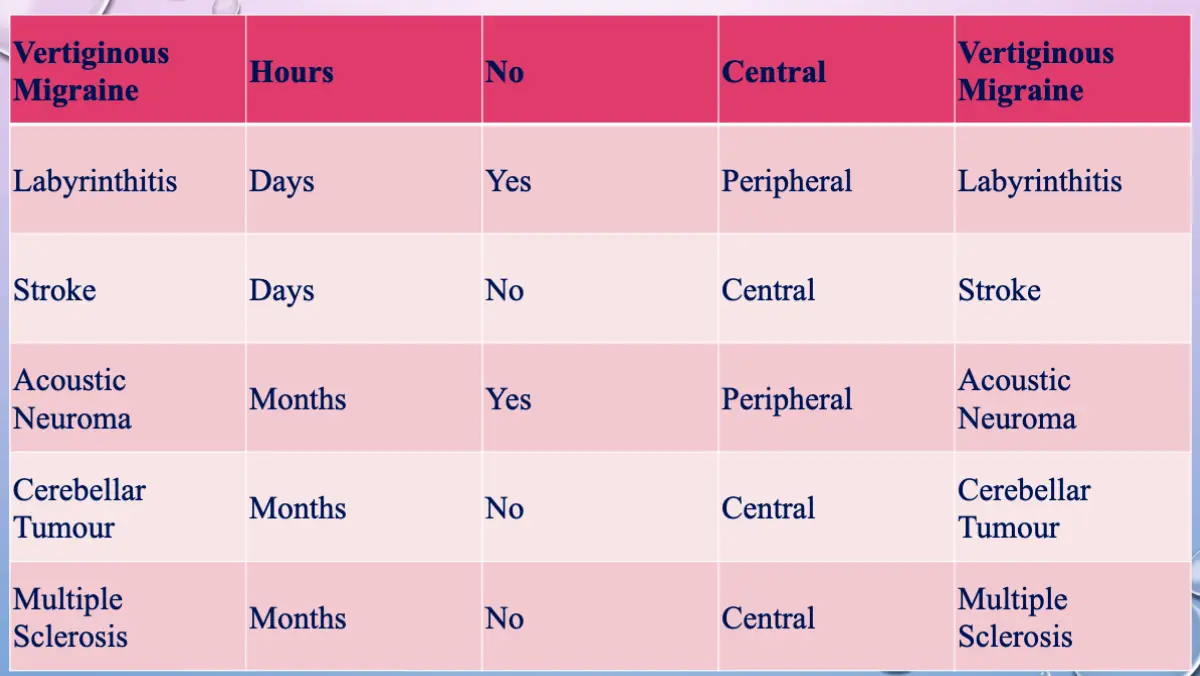
Timing of Symptoms Z
- The duration of vertigo episodes and associated auditory symptoms will help to narrow the differential diagnosis.
Primary Care Guidelines – Vertigo/Dizziness
- Vertigo is defined as an illusion of movement.
- Explore characteristics of symptoms; examine for nystagmus.
- Do a Hallpike test in all patients presenting with vertigo/dizziness.
- At every stage, explore ‘red flags’ and refer as necessary.
- Dizziness with presyncopal symptoms should be referred to cardiology.
- Exclude orthostatic/Postural hypotension.
- Consider migraine & treat if appropriate.
Presentations
1. Vestibular Neuritis
2. Benign Paroxysmal Positional Vertigo (BPPV)
3. Meniere’s Disease
Examinations
RED FLAGS
- First attack of vertigo with acute severe headache (REFER TO A/E – R/O CVA)
- Persistent symptoms for > 1 month (REFER TO ENT)
- Nystagmus lasting > 48 hours (REFER TO ENT)
- Unilateral tinnitus/dyacusis/aural fullness
- Sudden/fluctuating hearing loss
- Dysconjugate eye movements
- Posterior circulation symptoms
- Positive Hallpike test, provoking nystagmus but no symptoms
- Vertical nystagmus &
- Cerebellar signs
(All these refer to neurology).
Important Points in the History
- Onset - specific provoking events such as flying or trauma.
- Duration:
- Seconds - benign positional vertigo
- Hours - Meniere’s disease
- Weeks - labyrinthitis, post-head trauma, vestibular neuritis
- Years - may be psychogenic
- Associated auditory symptoms - rare in primary CNS lesion.
- Other associated symptoms:
- Nausea and vomiting in a vestibular cause.
- Neurological symptoms such as visual disturbance, dysarthria in a central lesion.
Preventive Measures for Recurrent Attacks
- Restrict salt and fluid intake.
- Stop smoking and restrict excess coffee or alcohol.
- Betahistine hydrochloride 16mg regularly TDS seems most effective in Meniere’s.
- Cinnarizine 15-30 mg TDS.
Points to Consider
- Warn patients when drugs may sedate.
- Prochlorperazine is less sedating than some other recommended antihistamines but may cause a dystonic reaction (particularly in children and young women).
- Benzodiazepines are not recommended.
Recurrent Vertigo
- The most important first step in the management of recurrent vertigo is to distinguish vertigo from dizziness.
- In attacks of vertigo, there is a sense of mobile disequilibrium (“the room spinning”) which, if severe, results in uncontrolled staggering in one direction, which may be only prevented by grabbing a solid object.
Referral to Secondary Care
- Recurrent episodes
- Neurological symptoms (e.g., dysphasia, paraesthesia, or weakness)
- Associated sensorineural deafness
- Inadequate visualization of the entire tympanic membrane or an abnormality (e.g., Cholesteatoma)
- Atypical nystagmus (e.g., Non-horizontal, persisting for weeks, changing in direction or differing in each eye)
Referral Guidelines
- If the patient has hearing problems in addition to vertigo, then referral should be made to an ENT specialist. Other cases should be referred to a neurologist.
While Awaiting Referral
- Consider symptomatic drug treatment for no longer than 1 week because prolonged use may delay vestibular compensation.
- It is important that the person stops symptomatic treatment 48 hours before seeing a specialist, as it will interfere with diagnostic tests such as the Dix-Hallpike manoeuvre.
References
- Clinical practice guideline: BPPV
- Vertigo - diagnosis and management in primary care: BJMP – 2009
- Dizziness primary care management guidelines for GPs. 24 June 2016