FM
Clinical Features
- One of the commonest causes of true vertigo.
- Age of onset is 40 years (range 20-60).
- Is due to temporary lesion of the vestibular nerve.
Vertigo
- Vertigo comes suddenly and without warning, it is continuous, it lasts for about 6 weeks.
- Head movement may worsen symptoms.
- 90% of patients have nausea.
- 55% have vomiting.
- 70% have nystagmus.
- In 43% attacks are recurrent, each successive recurrent is milder than the one before.
- In 45% the attack is preceded by infectious illness.
Treatment
- Partly by vestibular sedation & partly by the brain compensation.
- Explanation and reassurance are an important part of management.
This is a frightening condition; many patients fear a more severe cause for the symptoms.- Prochlorperazine in a dose of 5 mg three times a day.
- S/E a Parkinson’s like syndrome on chronic use.
Compensation
- In time the brain adjusts to the distorted information it is getting from the labyrinthine; this process can be accelerated by doing exercises.
- Eye, head & shoulder movement can be used.
- Standing and walking with the eyes closed also stress labyrinthine function.
Habituation Techniques
- Avoid quick spins or movements that provoke vertigo.
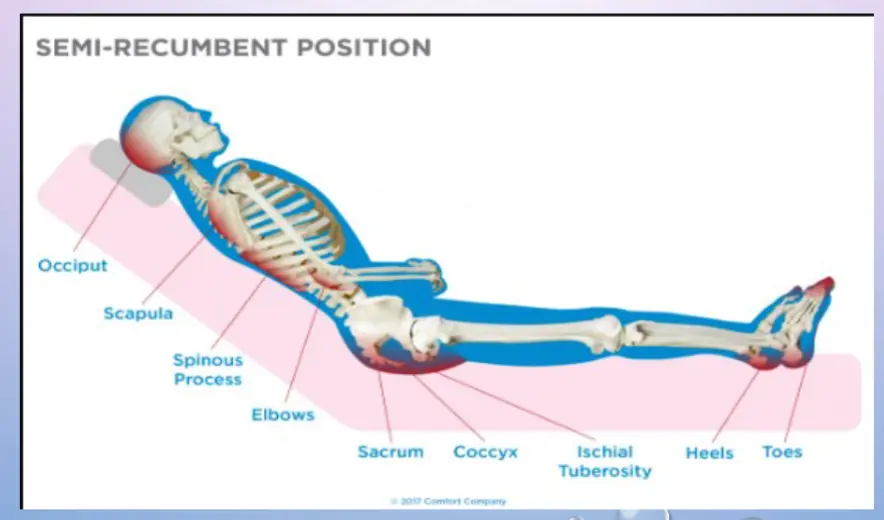
- Sleep in a semi-recumbent position for the next two nights following the above technique. In most cases, a recliner works well, or stacking pillows at the head of the bed. Avoid sleeping on the affected side.
- Try to keep the head upright during the day; avoid all supine activities.
- After a week of being conservative, start to place the head (in controlled environments) in vertigo provoking positions.
ENT
Description
-
It is a disorder characterized by a sudden severe attack of vertigo caused by inflammation of the vestibular nerve.
-
Commonly preceded by attack of URTI .
Symptoms
Vestibular neuronitis may occur as a single, isolated attack of severe vertigo lasting 7 to 10 days, but many people have additional attacks of milder vertigo for several weeks thereafter.
The first attack of vertigo is usually the most severe.
The attack of vertigo is accompanied by nausea, vomiting, and nystagmus . The vertigo is severe at first, and gradually subsides over the course of several days, with residual imbalance lasting up to several months. People do not have tinnitus ,and hearing is usually not affected.
Although vestibular neuronitis and labyrinthitis may be closely related in some cases, vestibular neuronitis is generally distinguished from labyrinthitis by preserved auditory function.
Diagnosis
- -Hearing tests
- -Tests for nystagmus
- -(MRI) of the head should be done to make sure the symptoms are not caused by another disorder, such as a stroke.
Treatment
- -Drugs such as meclizine relieve vertigo
- -Drugs such as prochlorperazine to relieve vomiting
- -Sometimes corticosteroid drugs such as prednisone
- -Intravenous fluids if vomiting persists
- -Physical therapy