Consists of four fused rings, substitutions on rings alter individual pharmacokinetics and spectrum of antimicrobial activity
Drugs:
Oxytertacycline, Tetracycline, doxycycline
Tetracyclines enter susceptible orgnamisms via:
- Passive diffusion through porin channels in the bacterial membrane
- By an energy-dependant transport protein mechanism Also, tetracyclines concentrate intracellullary in susceptible organism
MOA: Static
- Tetracycline reversibly binds to the 30S ribosomal subunit. This action prevents binding of tRNA to the mRNA– ribosome complex, thereby inhibiting bacterial protein synthesis
- They chelate some cations necessary for enzymatic action in bacteria e.g. Ca, Mg and Mn.
Antibacterial spectrum ±
Tetracyclines display broad-spectrum activity and are effective against:
- Most gram-positive, many gram-negative bacteria and anaerobic bacteria.
- Rickettsia, Coxiella, Mycoplasma and Chlamydia, Brucella.
- Spirochetes, Actinomycines, Protozoa.
- Helico bacter pylori.
Resistance
- Efflux pump, pushes out the drug.
- Enzymatic inactivation of the drug
- Production of bacterial proteins that prevents tetracyclines from binding to the ribosomes
Pharmacokinetics
A) Absorption
Nuritions, vitamins, causes inability of drug to act. such as milk, iron. May leade to Superinfection
-
These antibiotics are partially absorbed from the stomach and upper gastrointestinal tract and the amounts remaining may alter bacterial flora leading to super infection.
-
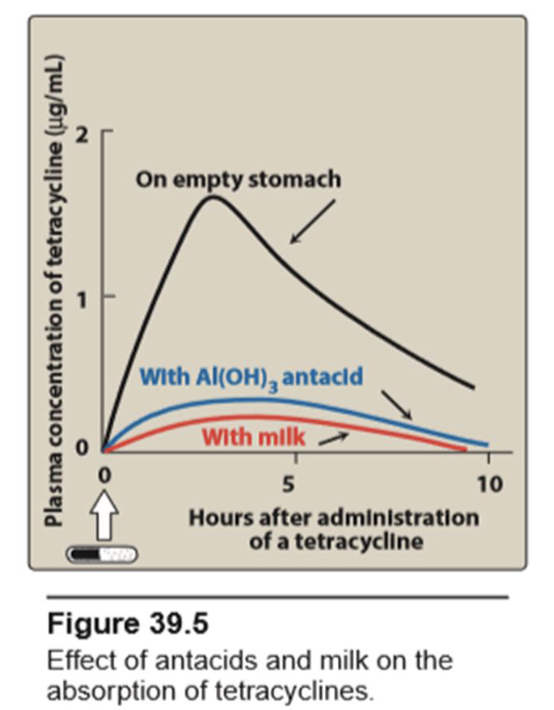
Calcium (milk and Ca. antacids), magnesium (Mg hydroxide), aluminum hydroxide and iron interfere with their absorption since they form insoluble chelates with tetracyclines.
-
Food did not impair absorption of doxycyclin. Because absorption of doxycycline is rapid and complete ,it has weak effect on intestinal flora
B) Distribution Least lipid soluble, can be used for eye infection, and CSF such as (minocyclins & doxycyclins) - Can cause bone, growth, tooth, discoloration deformations. espicially in pregnancy and children under age of 8 - Tetracyclines are distributed throughout body tissues and fluids. - Doxycycline is the most lipid-soluble, while oxytetracycline is the least lipid soluble. - All concentrate well in the bile, liver, kidney, gingival fluid, and skin. - All, bind to tissues undergoing calcification (for example, teeth and bones) or to tumors that have a high calcium content. All tetracyclines cross the placental barrier and because of their chelating properties with calcium they tend to be deposited in growing bones and teeth causing yellow discoloration. - Only minocycline and doxycycline achieve therapeutic levels in the cerebrospinal fluid (CSF). - Minocycline also achieves high levels in saliva and tears, rendering it useful in eradicating the meningococcal carrier state.
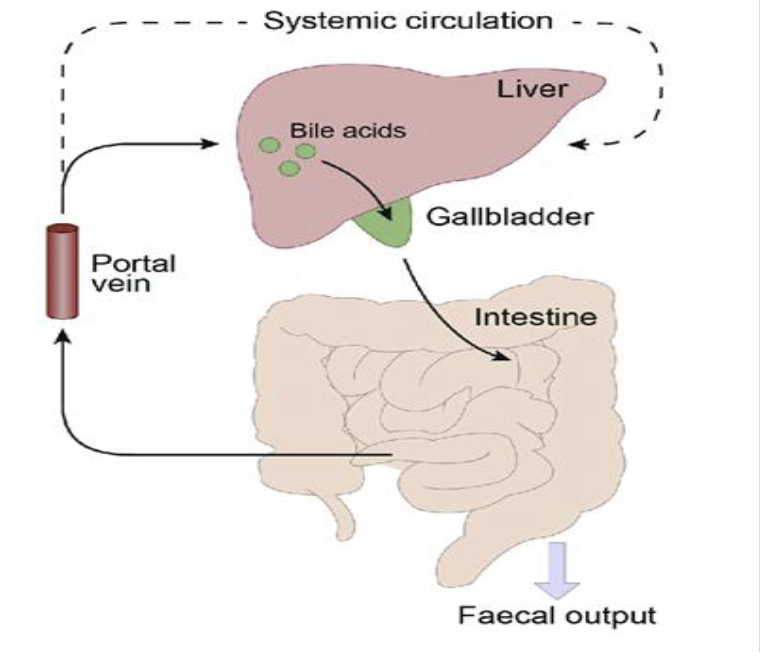
C) Metabolism and excretion: Tetracyclines are metabolized in the liver and are concentrated and excreted in the bile then reabsorbed (EHC). Tetracyclines is primarily eliminated unchanged in the urine by glomerular filtration.
Doxycycline is primarily eliminated via the bile into the feces therefore, it is preferred in renaly compromised patients.
Therapeutic Uses
The use of tetracyclines became limited because of other safe and bactericidal antibiotics, the appearance of tetracycline- resistant strains as well as their various adverse effects.
- Mycoplasma pneumoniae: although other agents may be equally effective
- Drug of choice for treatment & Prophalaxis of cholera (1st choice)
- Combination regimen to treat gastric and duodenal ulcer disease caused by helicobacter pylori.
- clinically effective in white spots acne; sebum - highly irritant to pressure. (Minocycline & Doxycyclin)
- Rickettsia (typhus) and coxiella
- Granuloma inguinale and relapsing fever
- Chlamydial disease (trachoma, lymphogranuloma venereum)
-
- Nonspecific urethritis and mixed bacterial infection of respiratory tract e.g. sinusits, bronchitis
- They are also effective in the treatment of brucellosis and infections caused by pasteurella (plague)
-
- Tetracyclines are second choice in other diseases resistant to penicillins and in patients sensitive to penicillins e.g. syphilis, chancroid, gonorrhea, actinomycosis, anthrax and shigellosis.
-
- Bacillary and amoebic dysentery as adjuvant therapy (Oxetetracycline is the most active one, it acts indirectly by modifying the intestinal flora necessary for amoebae to survive in bowel lumen).
-
- Doxycycline in combination with quinine may be an alternative treatment of plasmodium falciparum malaria when resistance has developed to fancidar.
-
- Local applications of tetracycline e.g. eye ointment for treatment of eye infections.
- Demeclocycline is also used to treat SIADH, and pleural and pericardial effusions (inappropriate secretion of antidiuretic hormone (e.g. by some malignant lung tumours), causing hyponataemia: demeclocycline inhibits the action of this hormone
- (Lyme disease,Q fever, and Rocky mountain)
Adverse effects:
- Gastrointestinal disturbance: nausea, vomiting, epigastric burning and hyperacidity. Epigastric distress commonly results from irritation of the gastric mucosa . It is often responsible for noncompliance with tetracyclines. Tetracyclines can cause esophageal irritation and esophagitis which can be minimized: through co-administration with food (other than dairy products) or fluids and patients should take the drug while standing up if possible.
Antacids may help but avoid those containing Al, Mg and milk because they chelate tetracycline.
Diarrhea may occur secondary to tetracycline treatment due to: *The irritative effect of tetracycline on GIT (leading to frequent fluid stools which do not contain blood or leucocytes).
- *Superinfection of bowel (see before)e.g. Pseudomembranous colitis caused by the overgrowth and production of toxins by clostridium difficile (which is cytotoxic to mucosa leading to ulcer, severe diarrhea, fever, shreds of mucosa in stools with large number of neutrophils. Diarrhea in these cases could be treated by vancomycin orally or metronidazole with stopping of the causative agent).
- Disorders o Epithelial surfaces:
- e.g. sore throat, sore tongue, black hairy tongue, perioral soreness. The cause is decreased synthesis of Vit. B12 and mild superinfection.
-
Yellow staining of both the deciduous and permanent teeth: and dental enamel hypoplasia (increased susceptibility to caries, as well as retardation of bone growth) because of their chelating properties with calcium.This can occur if tetracyclines are administered after the fourth month of gestation or if they are given to children less than 8 years of age, this is a further reason for avoiding their use during pregnancy. Doxycycline is less likely to cause tooth discoloration
-
- Hepatotoxicity: Rarely hepatotoxicity may occur with high doses, particularly in pregnant women and those with preexisting hepatic dysfunction or renal impairment
-
- Phototoxicity: Severe sunburn may occur in patients receiving a tetracycline who are exposed to sun or ultraviolet rays. This toxicity is encountered with any tetracycline, but more frequently with tetracycline and demeclocycline. Patients should be advised to wear adequate sun protection. Minocycline can sometimes lead to blue coloring of tissues.
-
Vestibular dysfunction: Dizziness, vertigo, and tinnitus may occur particularly with minocycline, which concentrates in the endolymph of the ear and affects function. Doxycycline may also cause vestibular dysfunction.
-
Pseudotumor cerebri: The name means “false brain tumor” because its symptoms are like those caused by brain tumors. It is characterized by headache and blurred vision may occur rarely in adults. It is also called “idiopathic intracranial hypertension” or “benign, intracranial hypertension” Discontinuation of the drug reverses this condition.
-
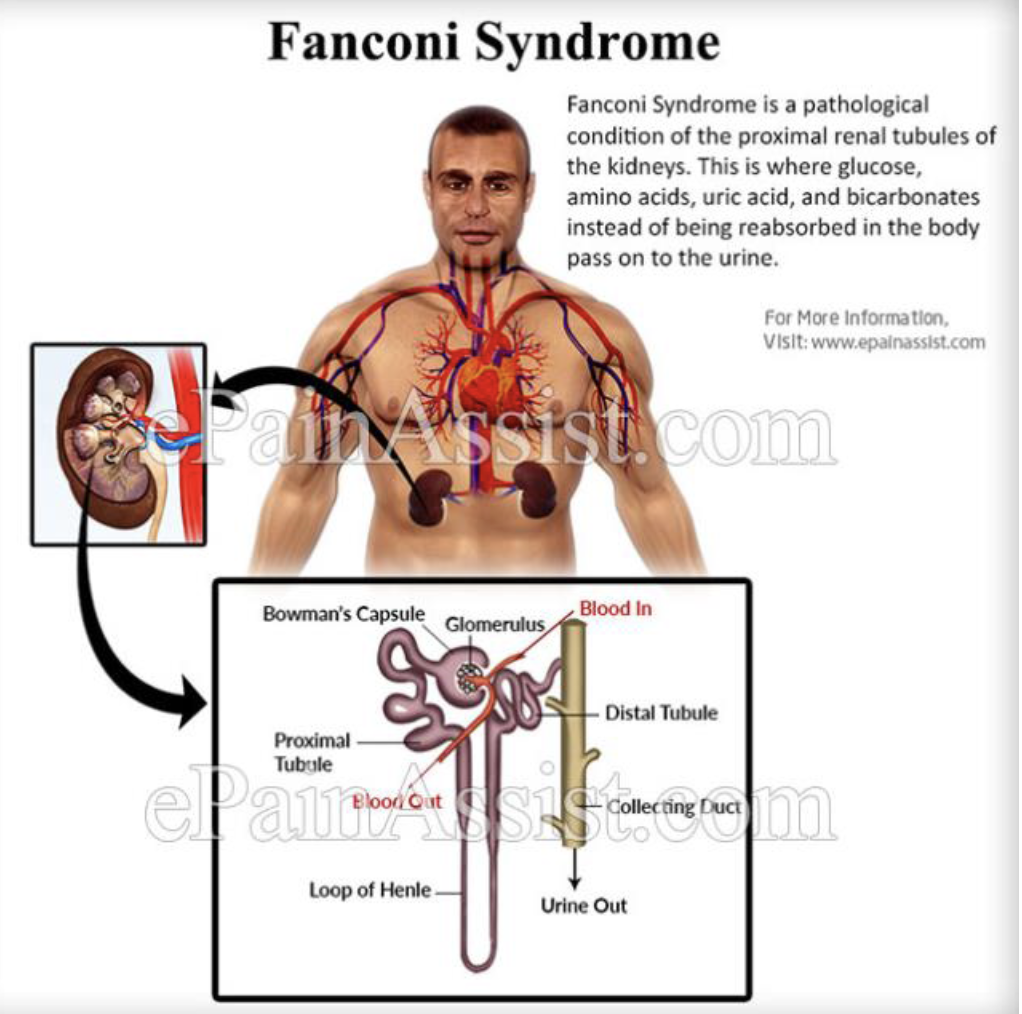
Fanconi syndrome may occur in patients taking outdated tetracycline, presumably due to toxic effects on the proximal tubule.
-
Cardiovascular: Omadacycline can lead to increases in heart rate.
-
Teratogenesis, when administered early in pregnancy.
-
Hypersensitivity reactions