Internal Medicine
Professor Salih Bin Salih
HTN & RENAL ARTERY STENOSIS
LATEST DEFINITIONS
According to A.C.C. ( American college of cardiology) & AHA ( American heart association)
- Normal BP : 120/80 or less
- If systolic BP is between 120 & 130, its now called “elevated BP”.
- Stage 1 HTN: Sys. 130 -140 , diastolic 80 to 90
- Stage 2 HTN: Sys. 140 or more, diastolic 90 or more
The diagnosis of HTN is made if BP is high on 2 different days, and the person should not be under stress or acutely sick.
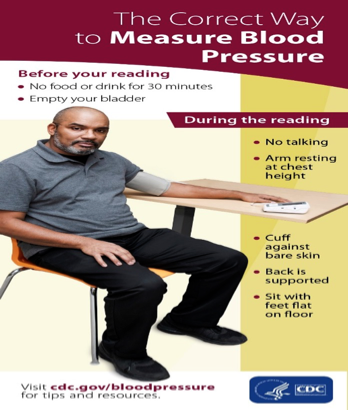
CORRECT WAY OF BP CHECKING
- Beware of “ White Coat Hypertension” ( high BP in doctor’s office).
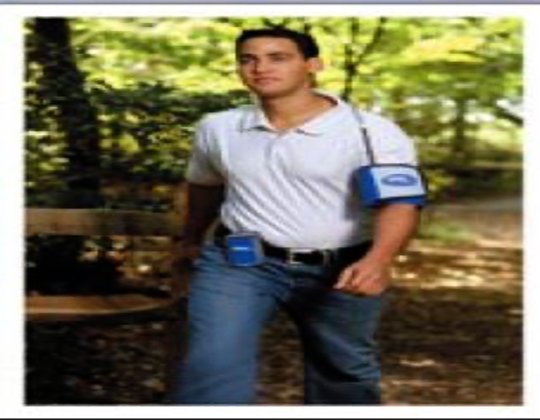
- Sometimes, you may need 24 hrs continuous BP monitoring at home ( ambulatory BP monitoring) to diagnose HTN.
24 hrs BP monitoring
EPIDEMIOLOGY
- In K.S.A, more than 25% of the adult population has HTN ( saudi medical journal, 2007)
- In the U.S., 29% of the adults have HTN
- Incidence is rising throughout the world
- (? Due to lifestyle)
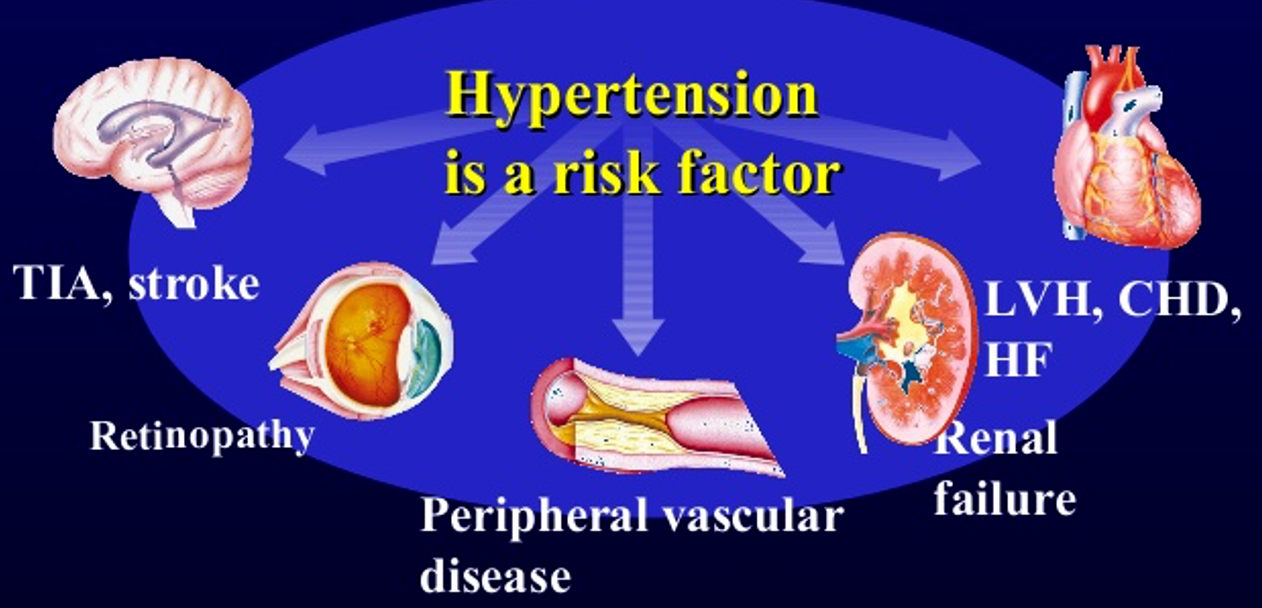
WHY IS HTN HARMFUL?Z
TERMS IN HTN
-
Elevated B.P. : Systolic between 120-130
-
Stage 1 HTN : Systolic between 130-140 and/or diastolic b/w 80 & 90
-
Stage 2 : Systolic 140 or more and/or diastolic 90 or more
-
Hypertensive Crisis : Systolic usually more than 180 and diastolic more than 120 ⇒ Hypertensive urgency X Hypertensive Emergency
Hypertensive Urgency:
- Very high BP. DBP usually >120, but NO acute
end organ damage (encephalopathy, angina,
papilloedema etc)
Hypertensive Emergency :
- Very high BP ( SBP > 210, and DBP> 130) + end organ damage begins ( eg encephalo- -pathy, angina/MI/blurred vision etc)
TYPES OF HTN
Primary hypertension
(no known cause) Also called essential HTN ( most cases are prim.)
- Also called Essential HTN. Etiology not known
- Most cases are primary HTN( >90%)
- Not due to any underlying disease, but the following may contribute to it :
- genetics, obesity, high salt intake, alcohol,
- smoking.
Secondary Hypertension
(secondary to an underlying disease)
- Secondary to some other disease
- Accounts for less than 10% of HTN cases
Renal etiologies: Commonest etiology of secondary HTN is renal disease :
- Chronic renal failure ( due to any cause)
- Renal Artery stenosisZ
- DM nephropathy
- Polycystic kidney disease
2) Endocrine Causes :
- Excess cortisol (Cushing’s disease)
- Excess aldosterone ( Conn’s syndrome)
- Excess noradrenaline ( Pheochromocytoma) ( all above are adrenal diseases)
3) Drugs & Meds. :
- NSAIDS, Steroids, Estrogens, Flu & cold meds ( will worsen HTN), Cocaine
WHEN TO SUSPECT SEC. HTN?
- Young age ( less than 30 yrs)
- HTN not responding to max. therapy
- Clinical features of the secondary causes ( acromegaly, Cushing’s etc)
S/S of HTN
- Very non-specific
- Asymptomatic
- Headache, dizziness, body pain
- Sec. HTN: features of the underlying disease
- Severe rise in BP can present as angina/MI, CHF, stroke/TIA, altered mental status (encephalopathy) hypertensive crisis
Physical Exam
- Do a detailed examination at the first visit.
- Check the pulses, cardiac examination
- Examine for any S/S of Strokex
- Examine the eyes for retinopathy
- Examine the heart for murmurs, CHF
- Auscultate the abdomen for renal artery bruit ( occurs in renal artery stenosis)
- Look for features of Cushing’s, acromegaly etc. if you suspect these.
HYPERTENSIVE RETINOPATHY
Divided into 4 grades , based on severity
- Grade 1: Retinal vessels become less clear
- Grade 2: A-V nipping
- Grade 3: Edema, hemorrhages, Copper wiring
- Grade 4: Optic disc edema, silver wiring #x
Routine investigations
- CBC, urea, creatinine, electrolytes, lipid profile, ECG, blood sugar, urinalysis
- If secondary HTN is suspected order further tests accordingly
- ECG may show left ventricular hypertrophy
- High creatinine suspect renal pathology
MED
Diagnosis of HTN is made with prolonged High blood pressure without outside stressors, e.g. sickness
Correct way of Blood Pressure measurement
- Must not be in any effect of drugs or actions that may raise BP such as caffeine, talking to patient, smoking prior to the test would report high reading; its best to measure and monitor at home for better diagnosis
- Sitting, back, arm, hand supported
Types & Stages
-
Primary Hypertension; Non known cause, may be *genetics, alcohol, smoking, *
-
Essential Hypertension; Situational
-
Stage 1 HTN: 130-140 / 80-90
-
Stage 2 HTN: 140 / >90
-
Hypertensive crisis: systolic usually >180 / >120
- CO = SV x HR
- BP = CO * PRZ
Risk factors of HTN
- Transient ischemic attack
- Strokes
- Retinopathy
- Renal Failure
- Left ventricular Failure ⇒ CHD ⇒ HF
Routine Investigations
- Full CBC
- If 2ry, order more tests
Treatment
- Aim below 120/80
First trial: diet & exercise 2 months with (Low salt, wt. reduction, exercise, healthy fibers, stop smoking)
- Add medicine if 2 months with no progress - start with one medication
- .
- .
Drugs: ABCD
-
Diuretics; Thiazide; Action on distal convoluted tubules (moderate celing diueretic) lowers preload = less PR (cc); causes hypercalcemia, Hyperglycemia contraindicated in DM, Parathyroidism tumour,
-
ACE inhibitors; Hyperkalemia, contraindicated
- renal artery stenosis - may result in acute renal failure
- Pregnancy; renal failure in child, limb deformities Cat. X
-
ARBS
-
Beta Blockers; Contraindicated in Asthma, COPD due B action Masking of hypoglycemia by DM/Obesity Hypoglycemic drugs Not stopped suddenly; may cause increased & Upshoot hypertension
-
Ca. Channel blockers; may result constipation
-
Others; Alpha blockers (first dose hypotension),
Guidelines Rx
Old / Afro-Arabian:
- Diuretics
- Calcium Channel Blockers; (May cause Headache)
Young / White:
- ACE inhibitors
- Beta blockers (may not be used due sexual dysfunction)
Pregnancy:
- Avoid ACE & ARBS
in Hypertensive crisis Gradually reduce bloop pressure, to avoid cerebral ----
Lingual vein absorption due to nitroglycerin in acute attack