Diverticular diseases
- Includes a spectrum of conditions
- Asymptomatic vs symptomatic
- Acute vs chronic
- Complicated vs non complicated
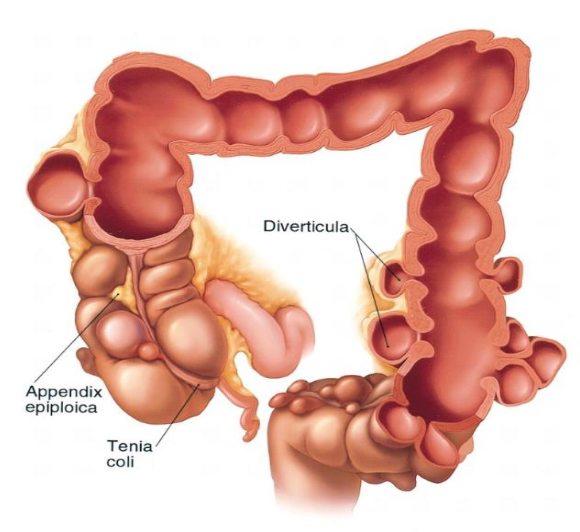
Diverticulosis:
- Small pouches due to herniation of the mucosa into colonic wall
- Commonest pathology responsible for lower GI bleeding
- False diverticula
- Inflammation of diverticula, due to obstruction by fecalith
- Usually affects elderly
- 20% of patients with diverticulitis are younger than 50 years.
- In chronic form, patients may have recurrent low-grade diverticulitis.
Signs and symptoms
Depends on the location, the severity of the inflammatory process, and the presence of complications.
-
Abdominal pain:
-
Left lower quadrant: (70% of patients), as most diverticula occur in the sigmoid colon
-
Right lower quadrant tenderness, mimicking acute appendicitis, can occur in right-sided diverticulitis
-
-
Change in bowel habits
-
Nausea and vomiting
-
Constipation
-
Diarrhea
-
Flatulence
-
Bloating
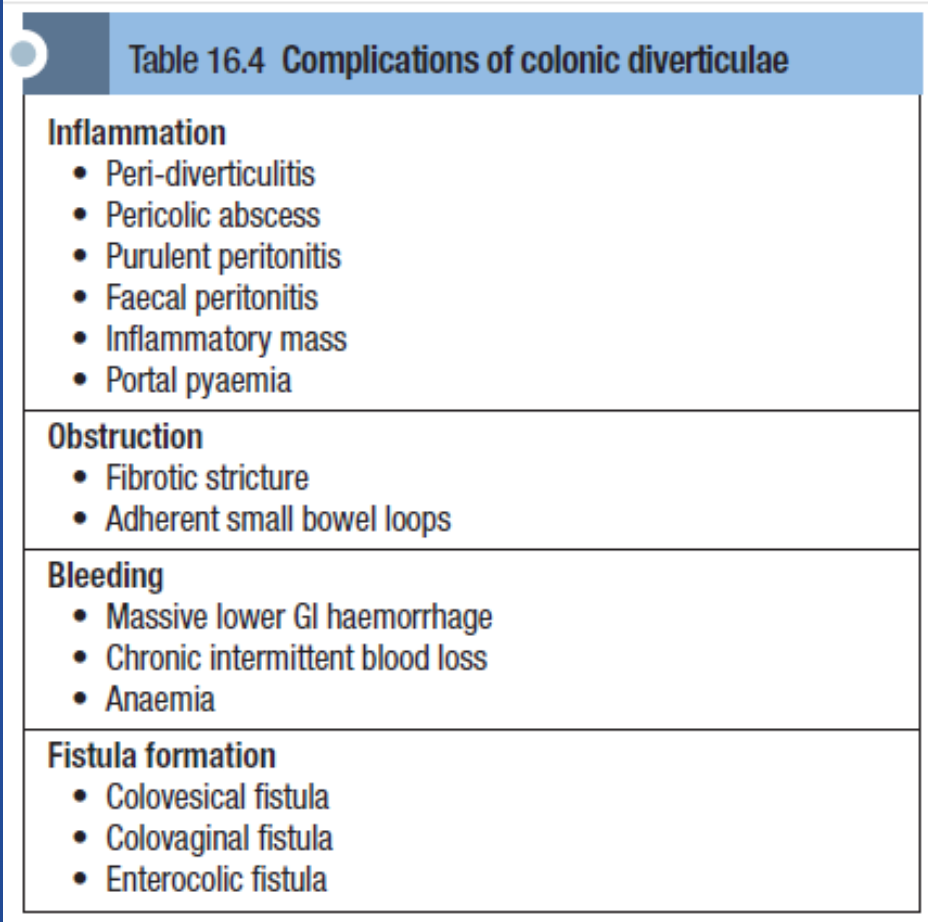
| Complication Category | Specific Complication |
|---|---|
| Inflammation | Peri-diverticulitis |
| Pericolic abscess | |
| Purulent peritonitis | |
| Faecal peritonitis | |
| Inflammatory mass | |
| Portal pyaemia | |
| Obstruction | Fibrotic stricture |
| Adherent small bowel loops | |
| Bleeding | Massive lower Gl haemorrhage |
| Chronic intermittent blood loss | |
| Anaemia | |
| Fistula formation | Colovesical fistula |
| Colovaginal fistula | |
| Enterocolic fistula |
Diagnosis
- Usually made on the basis of history and physical examination,
Laboratory tests :
- CBC: high WBC, Hb,
- Electrolytes,
- Renal function,
- LFT
- Urinalysis / culture
- Blood cultures
- Pregnancy test
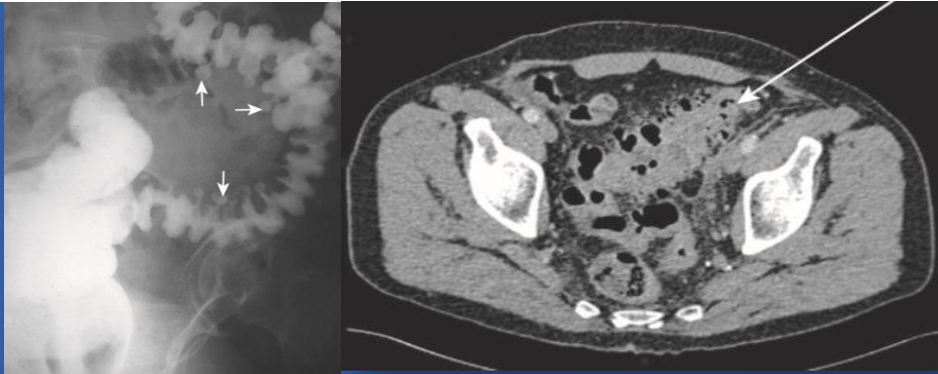
Radiology images:
-
Plain abdominal radiograph series
-
Contrast enema, * Water-soluble medium, * Mild-to-moderate uncomplicated cases
-
CT abdomen with contrast * Best imaging method to confirm the diagnosis. * Sensitivity and specificity 97% * Bowel wall thickening * Soft-tissue inflammatory masses * Complications, exclude other pathology
Hinchey’s classification for complicated cases:
- Clinical staging
- To chose the proper management option
| Hinchey Grade | Description |
|---|---|
| I | Localised para-colonic abscess |
| II | Distant abscess (e.g. pelvic, sub-phrenic) |
| III | Purulent peritonitis |
| IV | Faecal peritonitis |
Management:
- Conservative: (mild cases) * Initiate bowel rest and intravenous fluid hydration * Broad-spectrum intravenous antibiotic Within 2-3 days of hospitalization, fever, pain, and leukocytosis should begin to resolve * Start on a clear liquid diet and advanced as tolerated * CT-guided percutaneous drainage
Surgical intervention:
- Hinchey’s stage III or IV Z
- Complications
- Inability to rule out carcinoma
- Failure of medical therapy