Management of Diabetes Emergencies
DR H M ABDELRAHIM
Outline
- Diabetic ketoacidosis (DKA)
- Hyperosmolar hyperglycemic state (HHS)
- Acute hyperglycemia
- Acute hypoglycemia
Differences in DKA Treatment Recommendations
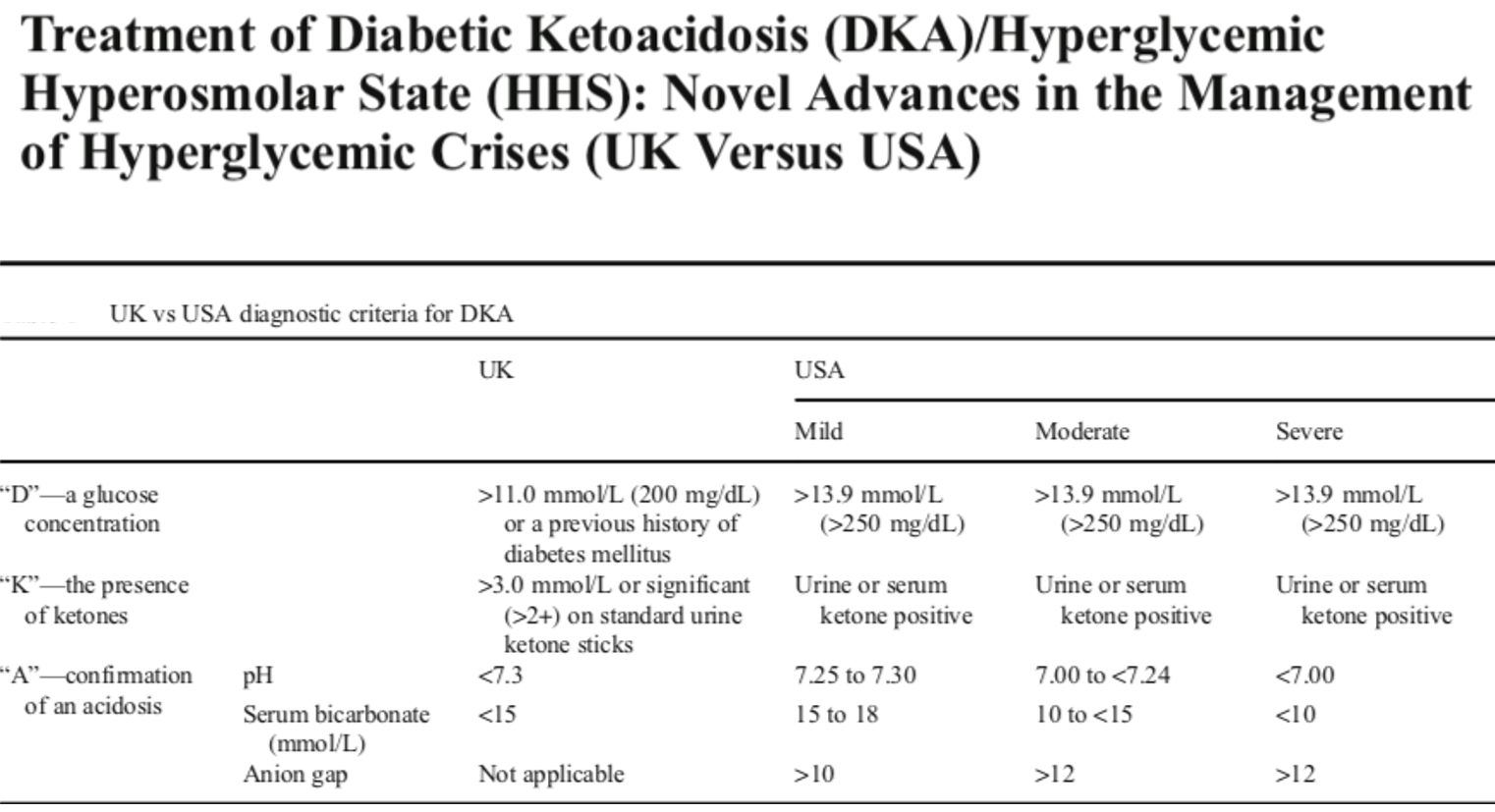
Because the evidence on which the guidelines are based is not very strong, you will find some differences in recommendations between the UK and the American guidelines.
First, there are small differences in the diagnostic criteria for DKA. The threshold level of glucose required for diagnosis in the UK is 200 mg/dL, whereas it is 250 mg/dL or above in the American guideline.
The presence of ketones in serum or urine is required in both guidelines, but a specific level is given in the UK guideline of 3 mmol/L or more if serum ketones are checked and two crosses or more if urine ketones are tested for by using urine ketone sticks.
Regarding the acidosis level required for diagnosis, both agree that a pH of less than 7.3 is needed to confirm acidosis. But for bicarbonate, a level of less than 15 mmol/L is chosen in the UK guideline, but in the American guideline, they stated that a level of bicarbonate below 18 mmol/L is enough to make a diagnosis of mild DKA.
Lastly, the American guideline talks about a high anion gap as needed for the diagnosis, but because in the UK checking chloride is not part of the routine biochemistry that is done, anion gap is not mentioned as a condition for making the diagnosis. I will come back to talk in more detail about the anion gap and how to calculate it.
| Recommendation | UK | ADA/Uptodate |
|---|---|---|
| IV fluids | 0.9% saline only | Consider 0.45% saline if sodium high |
| Change to dextrose | When glucose ≤ 250 mg/dl | When glucose ≤ 200 mg/dl |
| IV insulin bolus | No | Yes |
| Continue basal insulin analog | Yes | Not mentioned |
| SC insulin analog | No | Yes, for mild/moderate DKA |
| Bicarbonate | No | Consider when pH ≤ 6.9 |
Differences in DKA treatment recommendations between UK and ADA/uptodate guidelines:
- The UK guideline recommends changing the IV fluid to dextrose when the glucose level reaches 250 mg/dL, whereas the cut-off level for change in the American guideline is 200 mg/dL.
- The UK guideline does not recommend an IV bolus of insulin before starting IV insulin infusion, whereas this is recommended in the American guideline.
- The UK guideline recommends continuing the basal insulin analog, but in the American guideline, this is not mentioned.
- There is no mention in the UK guideline of using a subcutaneous insulin analog as a way of insulin administration, whereas this is given as an option for treatment in the American guideline for mild or moderate DKA.
- Lastly, the UK guideline does not recommend using IV bicarbonate to treat acidosis, but the American guideline recommends considering giving bicarbonate if the pH is very low at less than 6.9.
DKA/HHS/Hyperglycaemia
- Spectrum of diabetic hyperglycemic emergencies:
- In any patient with severe hyperglycemia, need to rule out DKA.
- DKA is the most important as relatively common and potentially fatal.
- HHS is more serious but rare.
The three conditions of DKA, HHS, and just hyperglycemia should be considered as part of the spectrum of diabetic hyperglycemic emergencies. Whenever any patient presents with severe hyperglycemia, the most important task is to rule out DKA because it is the most common and can potentially be fatal. HHS is actually more serious and has a higher mortality, but it is much less common.
Epidemiology of DKA and HHS
In the USA:
- Annual incidence: 5-8 per 1000 diabetic subjects
- 145,000 cases of DKA per year
- 2.8% of all diabetic admissions are due to DKA
- HHS: <1% of all diabetes-related admissions
How common are DKA and HHS? Figures from the United States show that the annual incidence of this condition is between 5 to 8 per 1000 diabetic patients, with 145,000 cases of DKA reported per year and 2.8% of all diabetic admissions are due to DKA, whereas HHS is a much less common condition, representing only less than 1% of all diabetes-related admissions
Mortality of DKA and HHS
DKA Mortality:
- Overall: <1%
- Elderly + co-morbidities: >5% Z
Causes of death:
- DKA
- Underlying cause of DKA, e.g., infection, MI
- Complications of treatment, e.g., hypokalemia, cerebral edema
HHS mortality: 15%
How about mortality from DKA and HHS? Well, in DKA, the mortality is generally less than 1%. But the mortality can be as high as more than 5% in the elderly and in those with multiple co-morbidities. The causes of death in DKA include the metabolic abnormalities of DKA itself, but it could also be due to the underlying condition that caused DKA, such as infections or myocardial infarction. And death could also result from the complications of treatment, such as hypokalemia or cerebral edema. HHS is associated with a much higher mortality of up to 15%.