SURGERY
Intestinal Obstruction
Dynamic: where peristalsis is working against a mechanical obstruction.
Adynamic:
mechanical element is absent
Peristalsis my be absent (Paralytic Ileus) -May be present in non propulsive form. (mesenteric vascular occlusion or pseudo-obstruction)
Causes of intestinal obstruction:
- Adhesions- 40% Z
- Tumors -15%
- Inflammatory- 15%
- Obstructed hernia-12%
- Intraluminal-10%
- Miscellaneous -8%
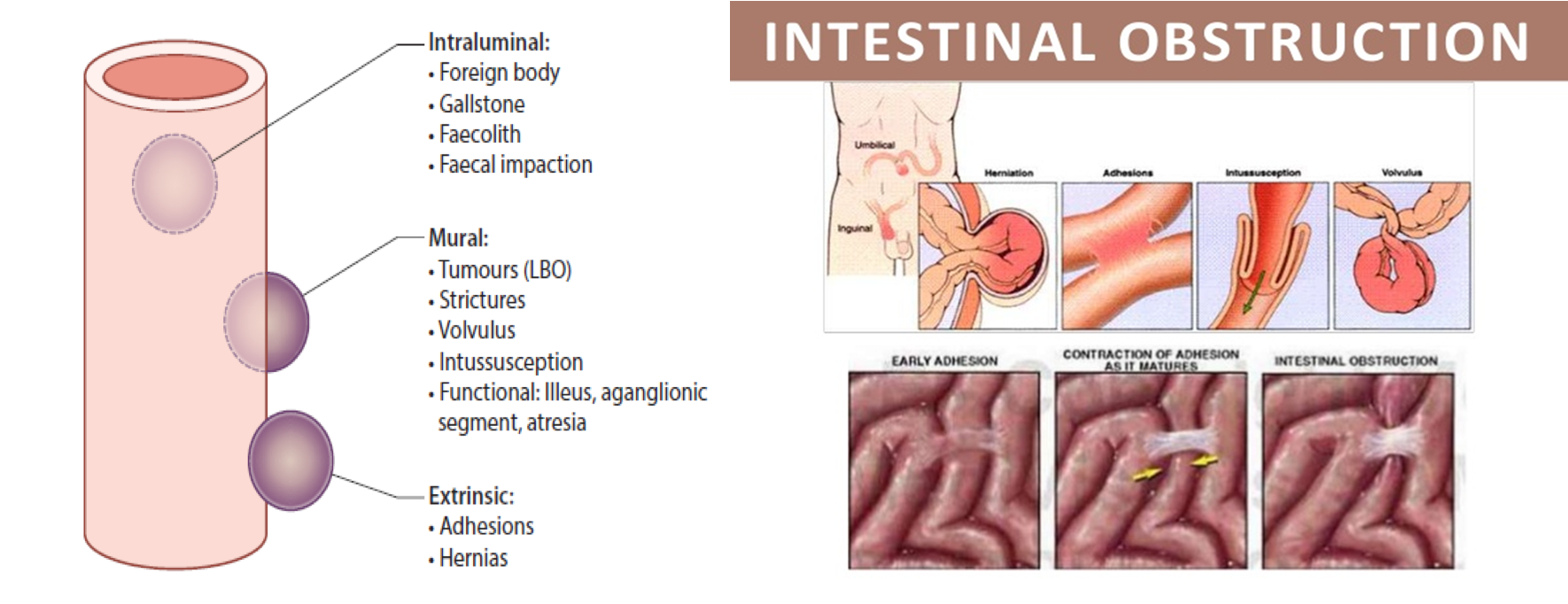
Mechanical Obstruction
- Intraluminal: impacted faeces, foreign bodies, gallstones, Bezoars.
- Intramural: tumors, inflammatory strictures,
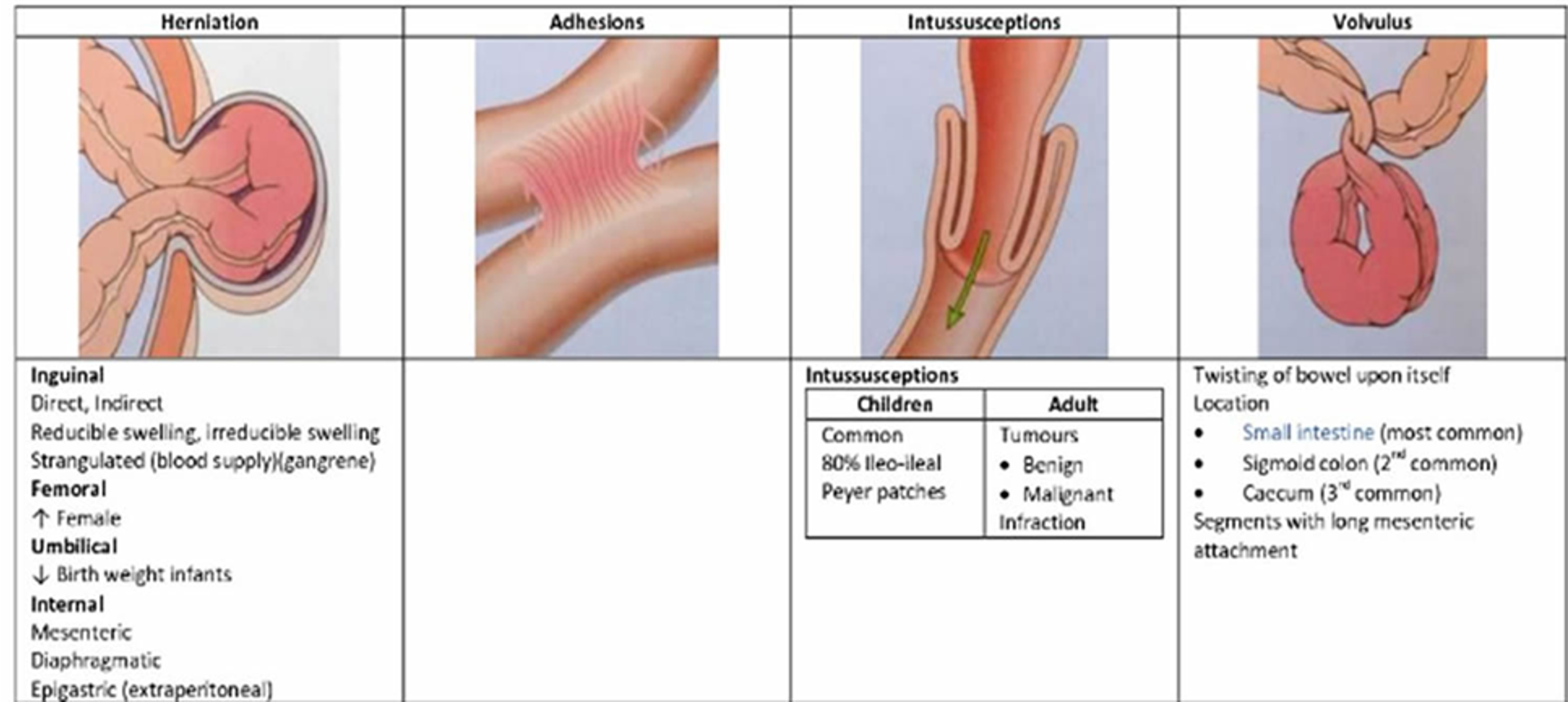
- Extramural: adhesion, hernias, volvulus, intussusception, tumors
Types of Obstructions
| Feature | Acute Obstruction | Chronic Obstruction | Acute on Chronic | Subacute Obstruction |
|---|---|---|---|---|
| Usual Location | Small bowel | Large bowel | ||
| Symptoms | Obstruction w/ Severe colicky central abdominal pain, distension, early vomiting, and constipation | Lower abdominal colic & obstipation followed by distension | Short history of distension & vomiting against background of pain & constipation | Incomplete obstruction |
| Feature | Simple | Strangulation | Closed Loop Obstruction |
|---|---|---|---|
| Symptoms | Blockage without interfering with vascular supply | Significant impairment of blood supply Most commonly associated with hernia, volvulus, intussusception, mesenteric infarction, adhesions/Bands. Surgical emergency | Bowel is obstructed at both the proximal and distal end |
Band adhesion causing a closed-loop obstruction.
Pathophysiology
Proximal to obstruction
- Increased fluid secretion ⇒ abdominal distention
- Accumulation of gas ⇒ abdominal distention
- Increased intraluminal pressure
- Vomiting
- Dehydration
- Dilatation of bowel
- Reflex contraction of smooth muscle ⇒ colicky pain
- Increased peristalsis to overcome obstruction ⇒ increased bowel sounds
- If obstruction not overcome ⇒ bowel atony
- Decreased reabsorption with time and flaccidity to prevent vascular damage from high pressure
Distal to obstruction: nothing is passed & bowel collapse ⇒ constipation
-
Colicky abdominal pain
-
Vomiting
-
Abdominal distension – increases as the condition progresses
-
Absolute constipation (Obstipation): absence of flatus and stool
-
Proximal small-bowel obstruction:
- less distention and more rapid onset of vomiting.
- Bilious vomiting
-
Distal small bowel obstruction:
- central abdominal distention
- vomiting (feaculent) is a late feature (because the bowel takes time to fill)
-
In strangulation:
- severe constant abdominal pain
- fever
- tachycardia
- tenderness with rigidity/rebound
- tenderness.
- shock
General examination
Early stage:
- Normal vitals
- Hyperactive bowel sounds
Late stage:
- Vital signs
- Signs of dehydration –tachycardia, hypotension
- dry mucus membrane, decreased skin turgor, decreased urine output
- Inspection:
- distension, scars, peristalsis, masses, hernial orifices
- Dilated loops of bowel may be palpable
- Palpation:
- tenderness, masses, rigidity
- Percussion:
- tympanitic abdomen
- Auscultation:
- high pitched bowel sound associated with peristalsis and cramp pain
- or silent abdomen
Examine rectum for mass, blood, feces or it may be empty in case of complete obstruction
Investigations
-
Full blood count (WBC, Hb, Hct), High WBC (neutrophilia with strangulation)
-
Electrolytes ( Hypovolemic hypochloremic hypokalemic alkalosis)
-
Hyper kalemia, hyperamylasemia & raised LDH may be associated with stangulation.
-
BUN, & creatinine levels: If increased, may indicate decreased volume state (e.g, dehydration).
-
Abdominal X-ray, at least 2 images (Supine & Erect)
-
Small bowel follow-through
-
CT abdomen with contrast (Triple)
-
Scopes (OGD/Colonoscopy)
Pneumoperitoneum
 The 3-6-9 rule is describing the normal bowel calibre:
The 3-6-9 rule is describing the normal bowel calibre:
- small bowel: <3 cm
- large bowel: <6 cm
- appendix: <6 mm
- caecum: <9 cm
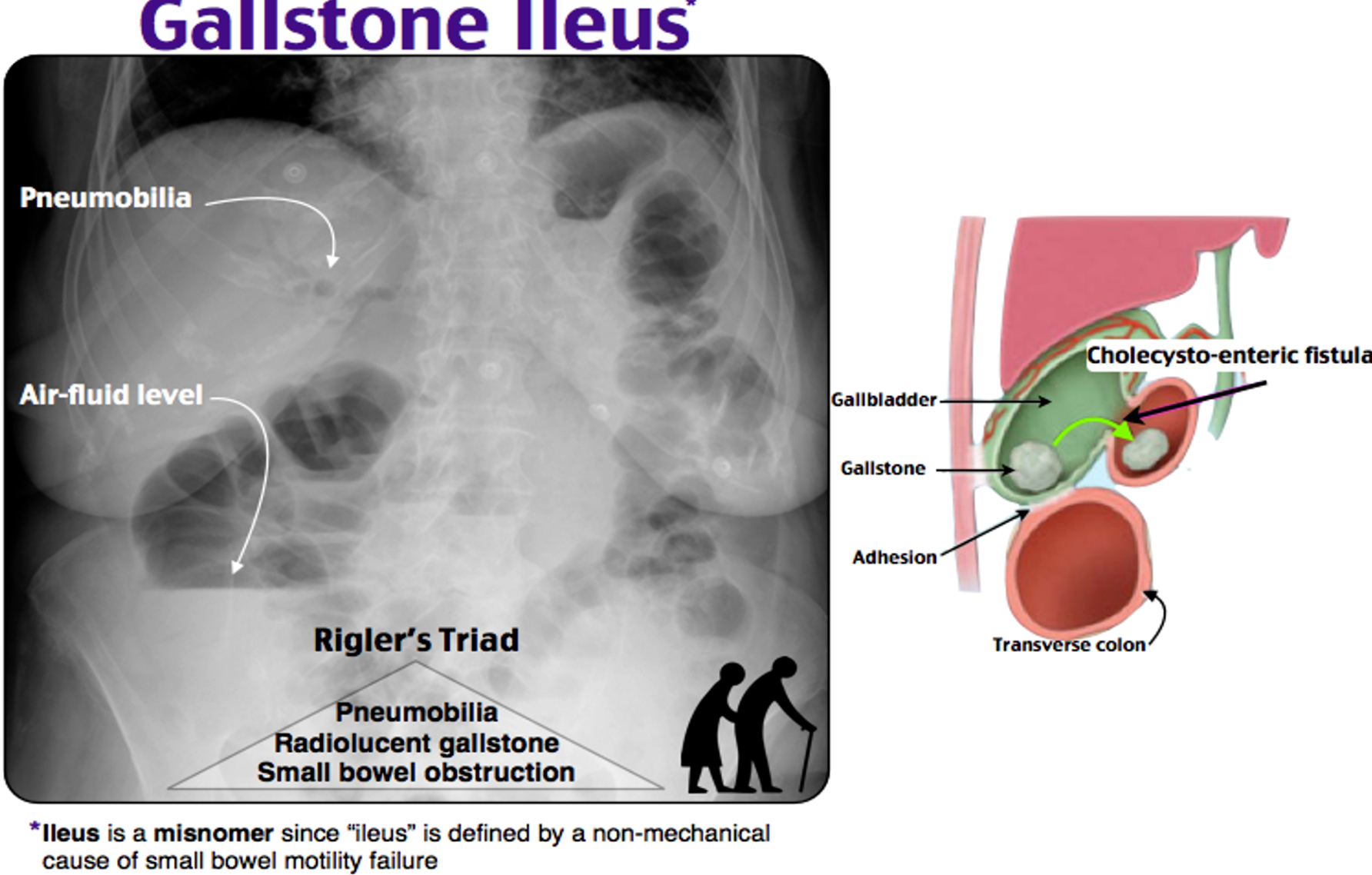
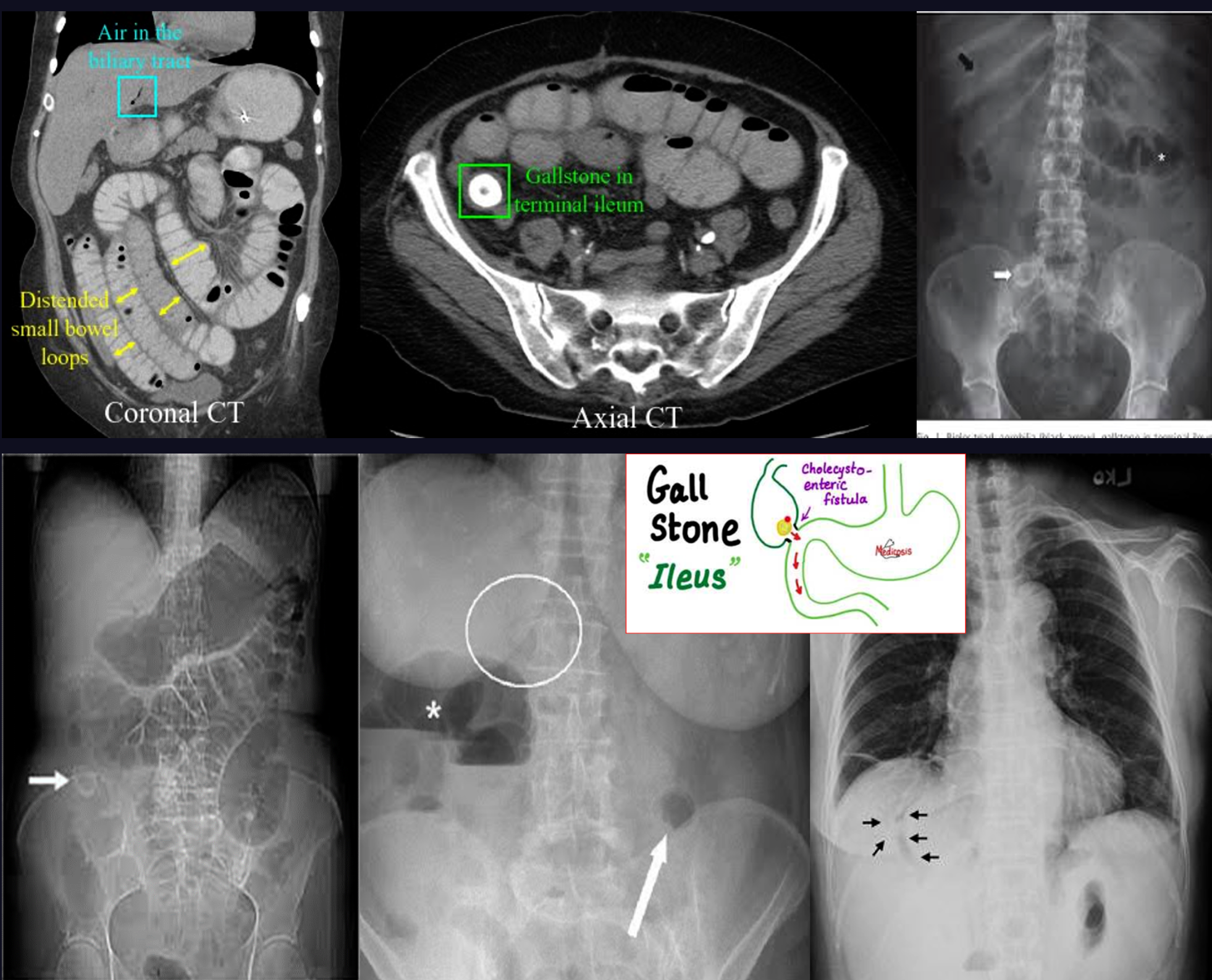
Rigler triad in gallstone ileus
- Pneumobilia; air in gallbladder due gallstone ileus // C. deficelle also Z
- Small bowel obstruction
- Ectopic gallstone
60 c 30f CC
Loss of apetite + pain in illiac fossa + Anorexia weak cough, due pain? - acute appendicitis?
Management
- Starts ABC
- Supportive measures:
- Nil By Mouth
- Intake- output charts
- IV lines, and rehydration (IV crystalloid with K+)
- Foley’s catheter
- NG Tube to aspirate content for ‘decompression’
- TED stockings, DVT prophylaxis
- Antibiotics
- Antiemetics
- Analgesia
- Might needs ICU
- Obstruction due to adhesion rarely need surgery
Indication for surgery:
- Virgin abdomen. (No previous surgery)
- failure of conservative management
- tender, irreducible hernia
- strangulation, peritonitis
Surgery:
- Assess bowel viability
- Treat the cause
- Adhesions…. Adhesiolysis
- Mass…… Resection
- Hernia…… Repair
- Etc.
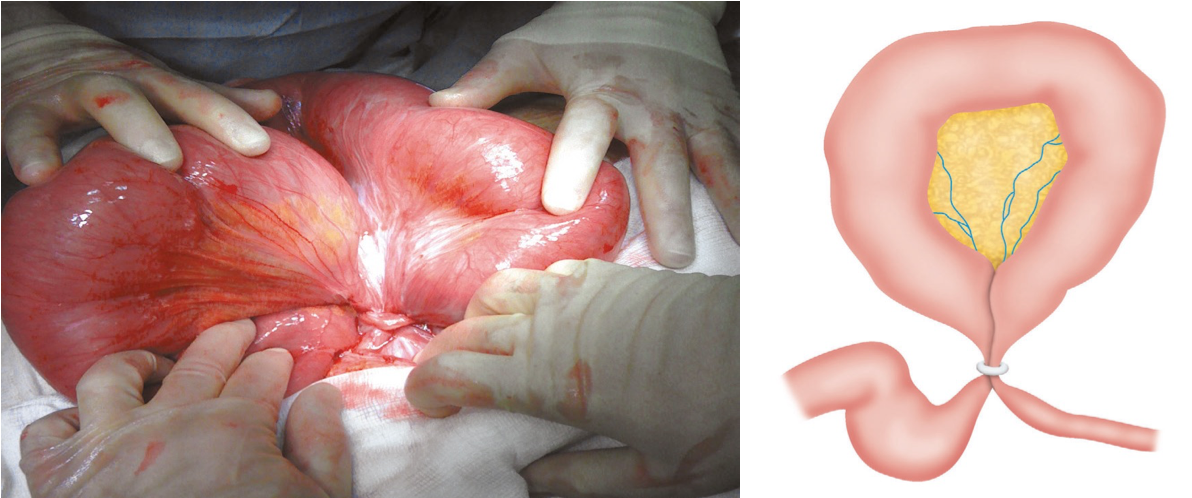
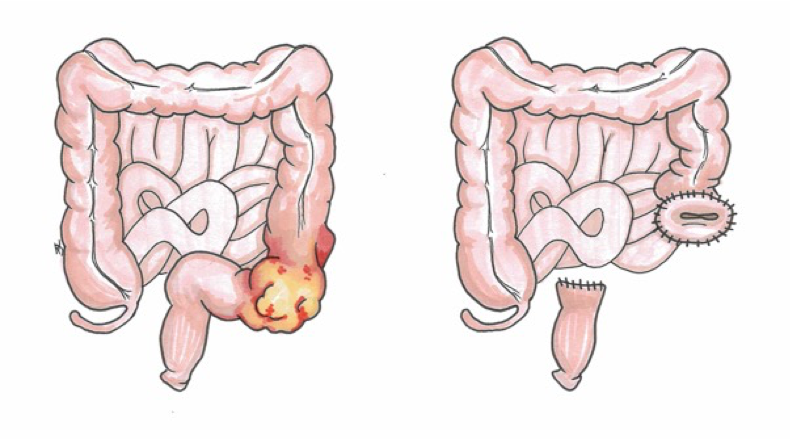 Sigmoid colon tumour obstruction
Sigmoid colon tumour obstruction
IMAGING
A) Mechanical bowel obstruction
is the interruption of normal passage through the bowel due to a structural barrier (Small or large)
B) Functional bowel obstruction or paralytic ileus
is a temporary disturbance of peristalsis in the absence of mechanical obstruction.
- Bowel obstruction typically manifests with nausea, vomiting, abdominal pain, abdominal distention, and constipation.
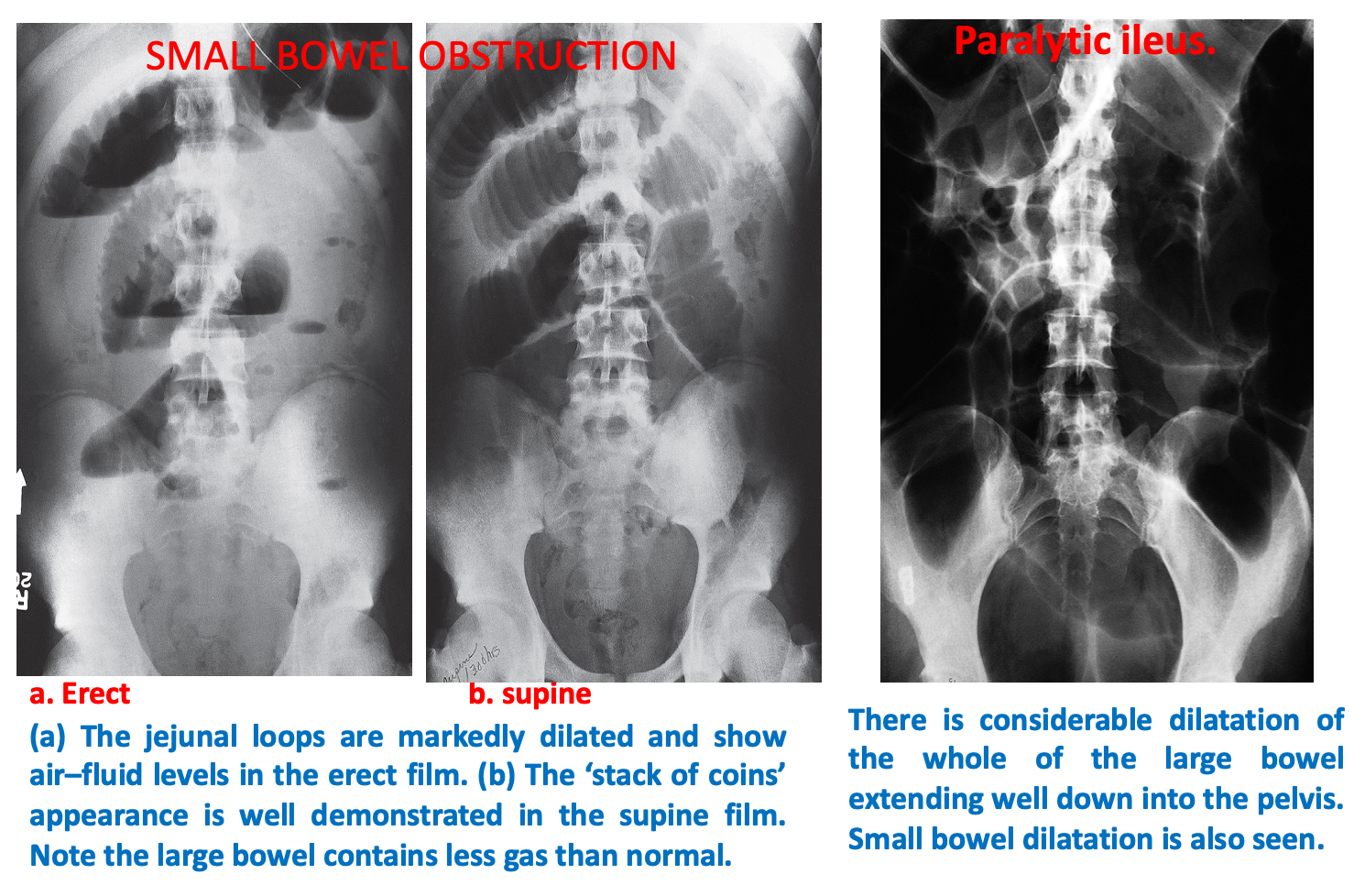
Radiological appearances:
Dilatation of bowel loops proximal to the obstruction: 3-6-9 rule :To help guide the identification of bowel dilatation on imaging. Transverse diameter greater than the following indicates dilation: Small bowel > 3 cm Large bowel > 6 cm Cecum > 9 cm
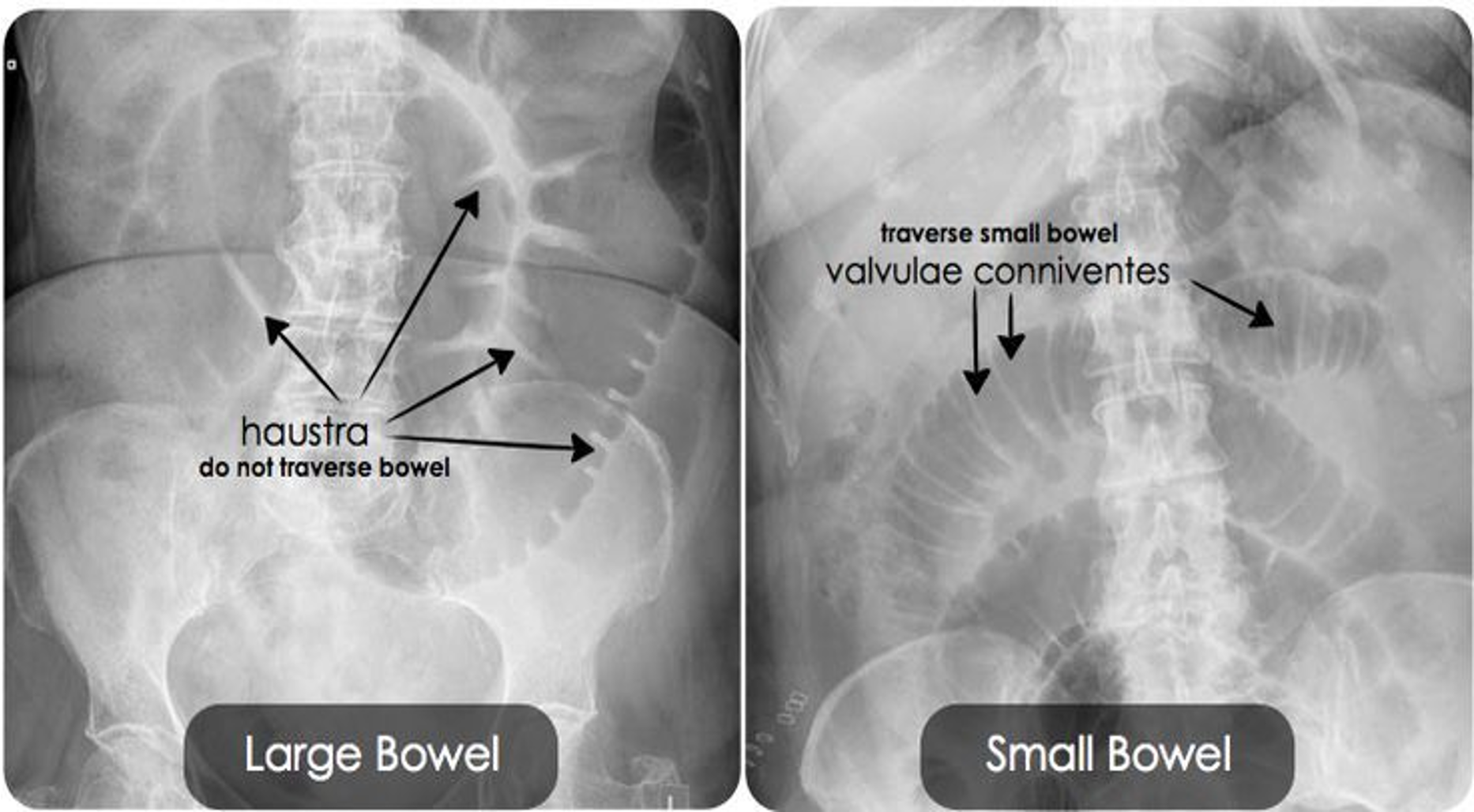
- SBO: Dilated loops are predominantly central.
- LBO : Dilated loops are predominantly peripheral.
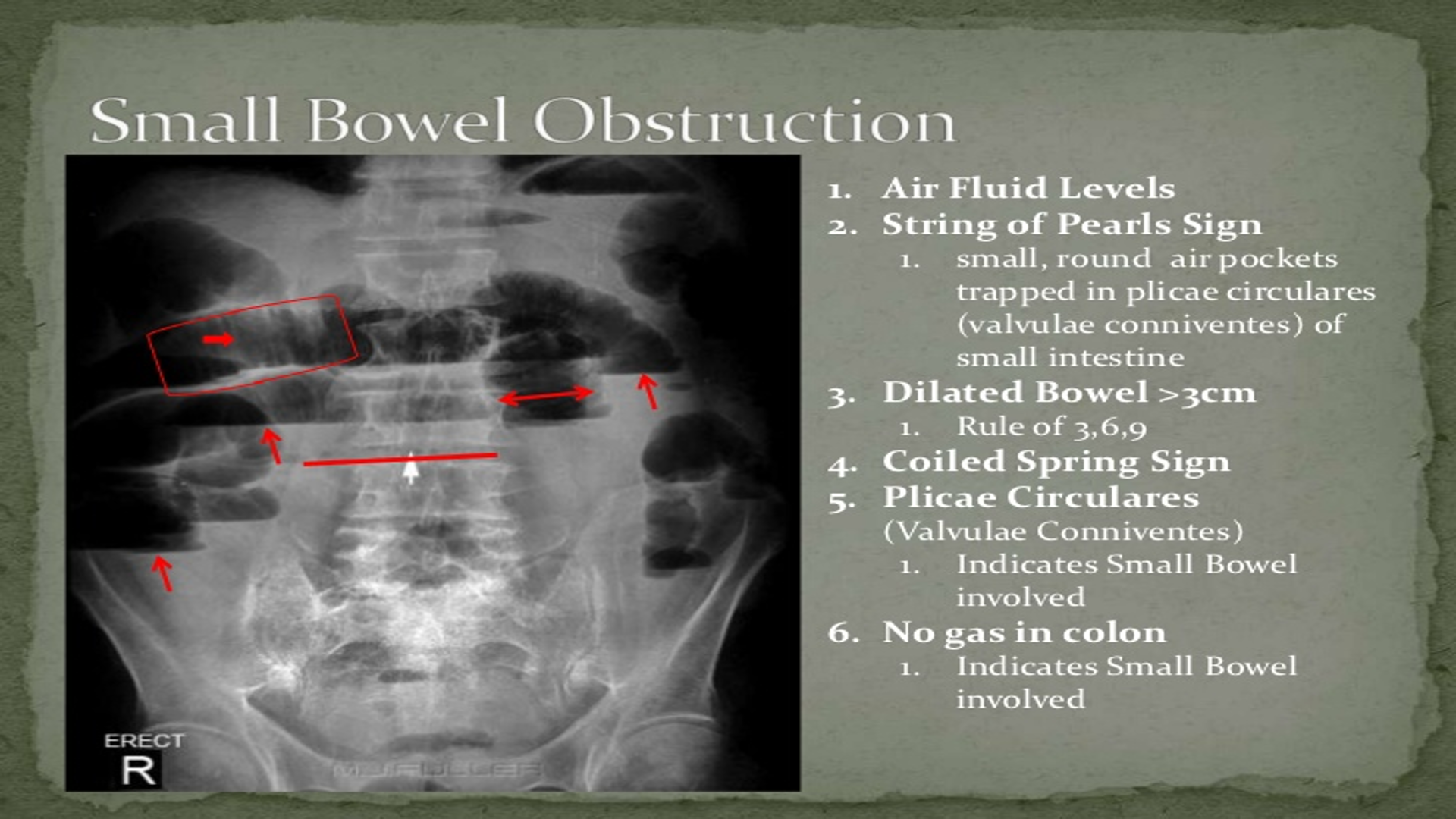
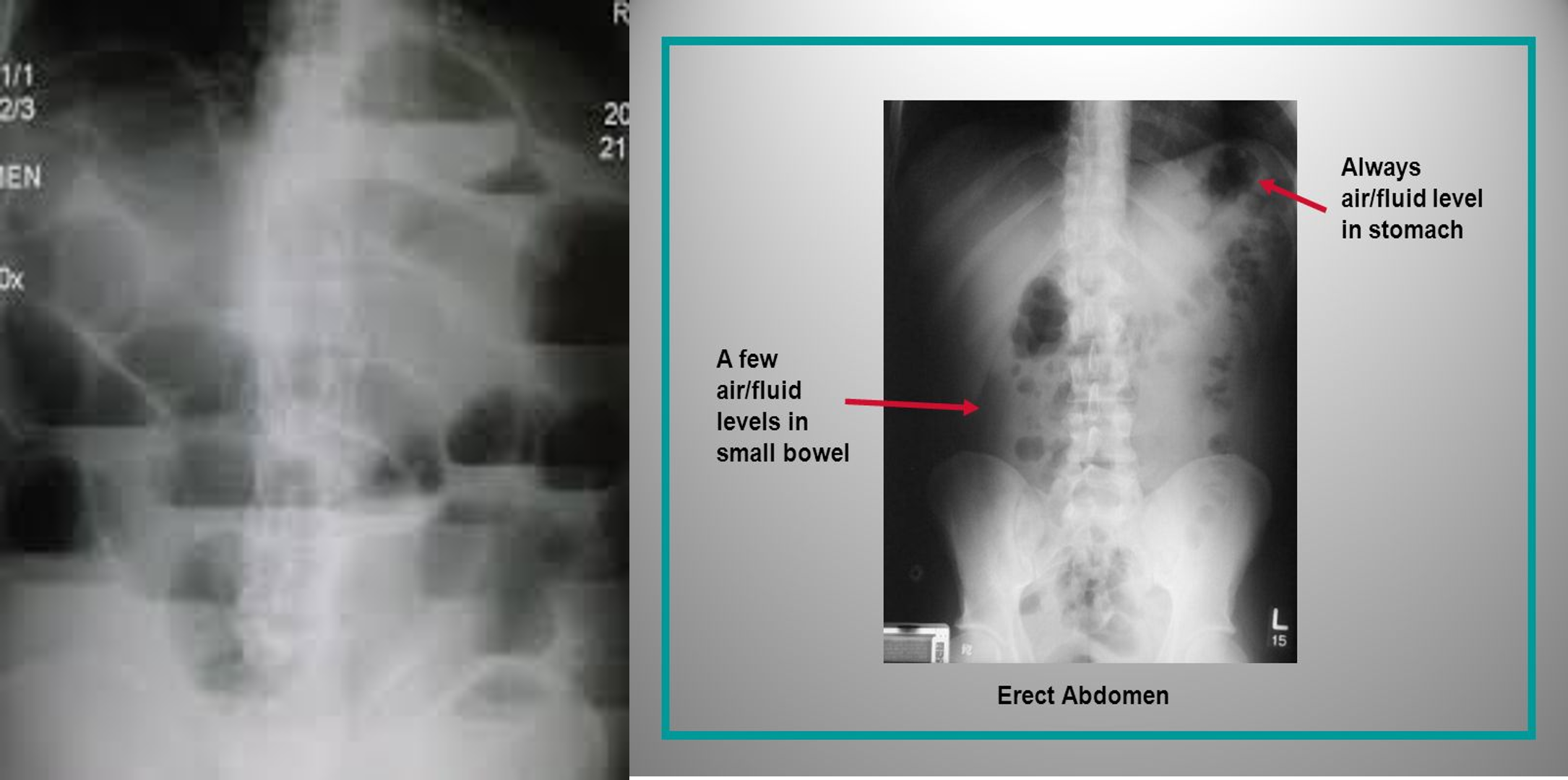
Air-fluid level:
- Visible on upright or decubitus views
- Common criteria for diagnosing SBO 3 air-fluid levels & Air-fluid level diameter > 2.5 cm
 #Z
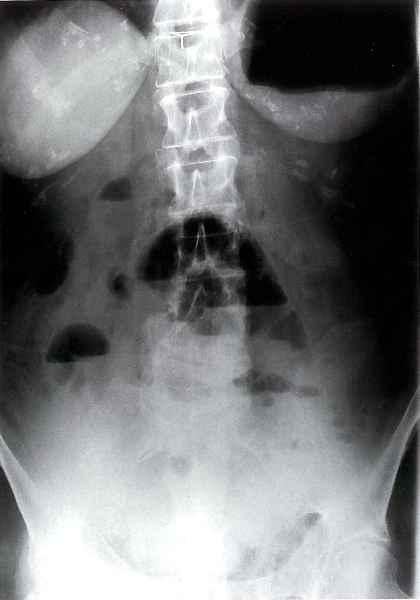
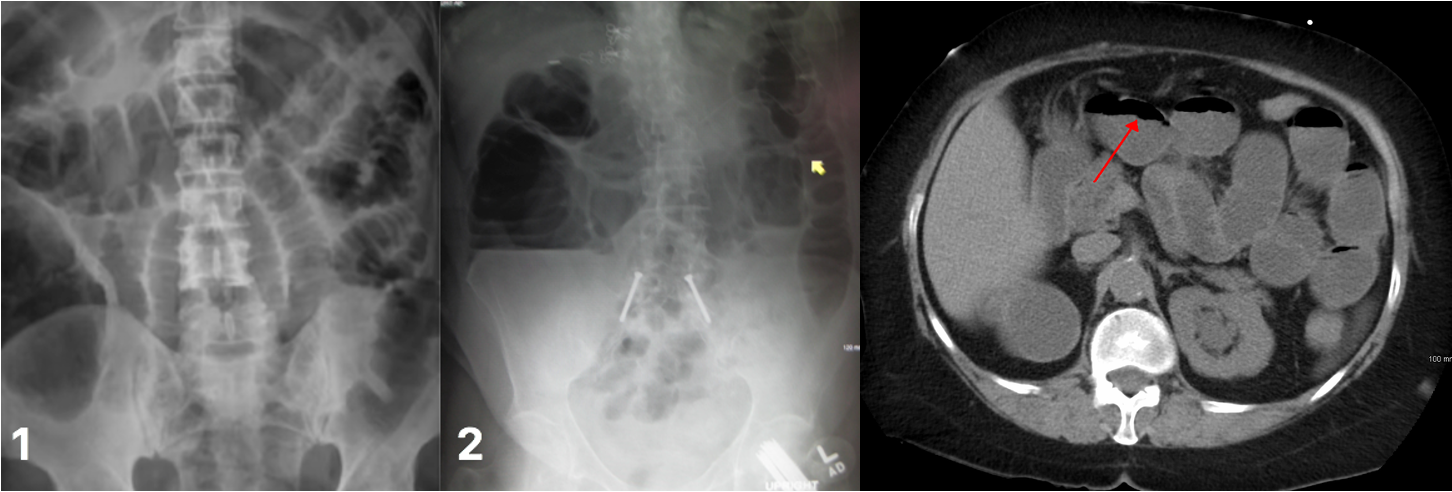
Mechanical small bowel obstruction-X-ray abdomen (erect)
Multiple air-fluid levels are visible in the mid-abdomen. The opaque appearance of the pelvis is due to fluid-filled loops of small bowel. There is a paucity of gas in the colon, and an air-fluid level is present in the dilated stomach.
#Z
Mechanical small bowel obstruction-X-ray abdomen (erect)
Multiple air-fluid levels are visible in the mid-abdomen. The opaque appearance of the pelvis is due to fluid-filled loops of small bowel. There is a paucity of gas in the colon, and an air-fluid level is present in the dilated stomach.
 bowel obstruction
bowel obstruction