





Acne Vulgaris (AV) CS-OSPE
Patient Presentation:
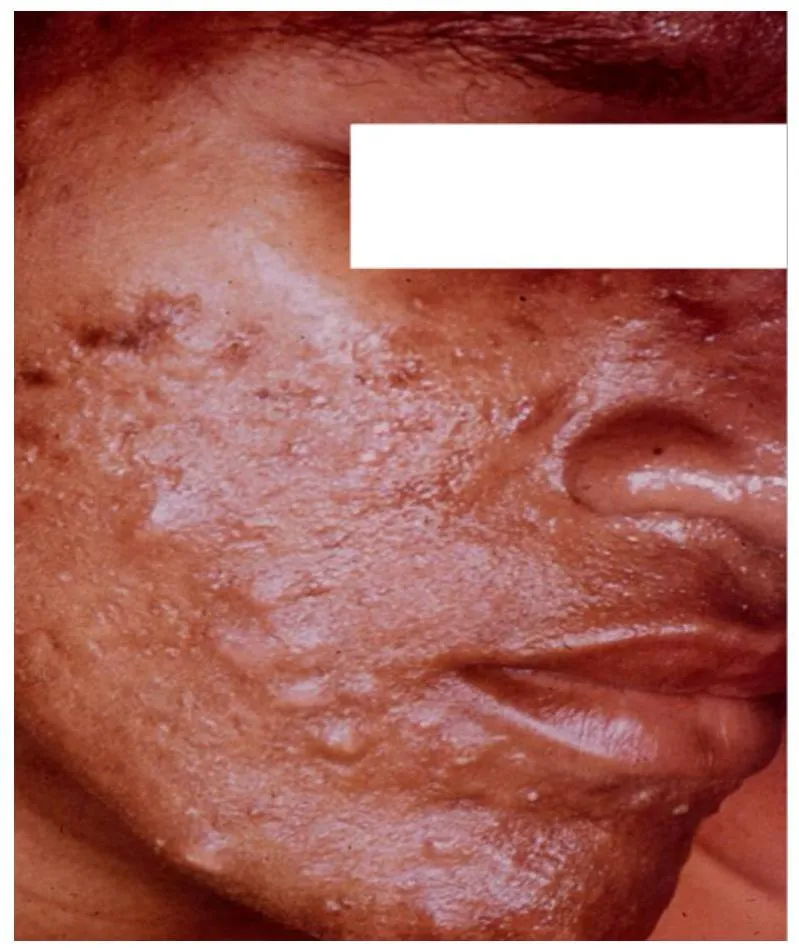
- An 18 Y/O teacher presents with skin lesions for 9 months.
- A 19-year-old man developed a facial eruption 6 months ago.
Diagnosis:
- Diagnosis: Acne Vulgaris
- Severity: Severe Acne Vulgaris
Differential Diagnosis:
- Rosacea (Acne Rosacea)
- Seborrheic dermatitis
- Folliculitis (Also recognized as a condition with pustule as a primary lesion, similar to Acne Vulgaris)
Clinical Description / Primary Skin Lesions:
- Pustule
- Papule (less than 5cm)
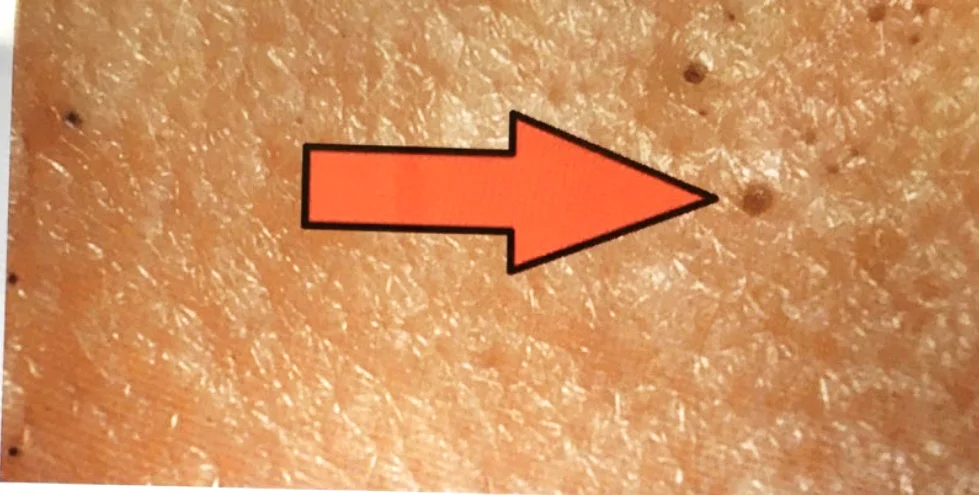
- Comedone (a hallmark primary lesion in this condition); these can be (close) white or (open) black headed (Open comedon)
- Nodule
- Cyst
- Scar
- Erythema
- Lesions are typically Red - Face
Severity Classification & Explanation:
- Classify the severity of this condition? Severe acne vulgaris
- Explain your classification/Pathological factors:
- Presence of Comedones, Papules, Pustules, Cysts, and Nodules.
- Also noted: Erythema, and Scars on the face and scattered.
- Severity is indicated by the presence of the nodule.
Body Sites Commonly Examined:
- Face
- Upper chest
- Back
- Shoulder
What are the 4 factors that contribute to development of ACNE?
- Production of excessive sebaceous gland secretion (Follicular Hyperkeratosis).
- Obstruction to outflow of this sebum at the mouth of the pilosebaceous canal.
- Inflammation arising as a result of leakage of contents of the pilosebaceous follicle into the surrounding dermis.
- Excessive colonization or infection of the pilosebaceous ducts with propionibacterium acnes (P.acnes).
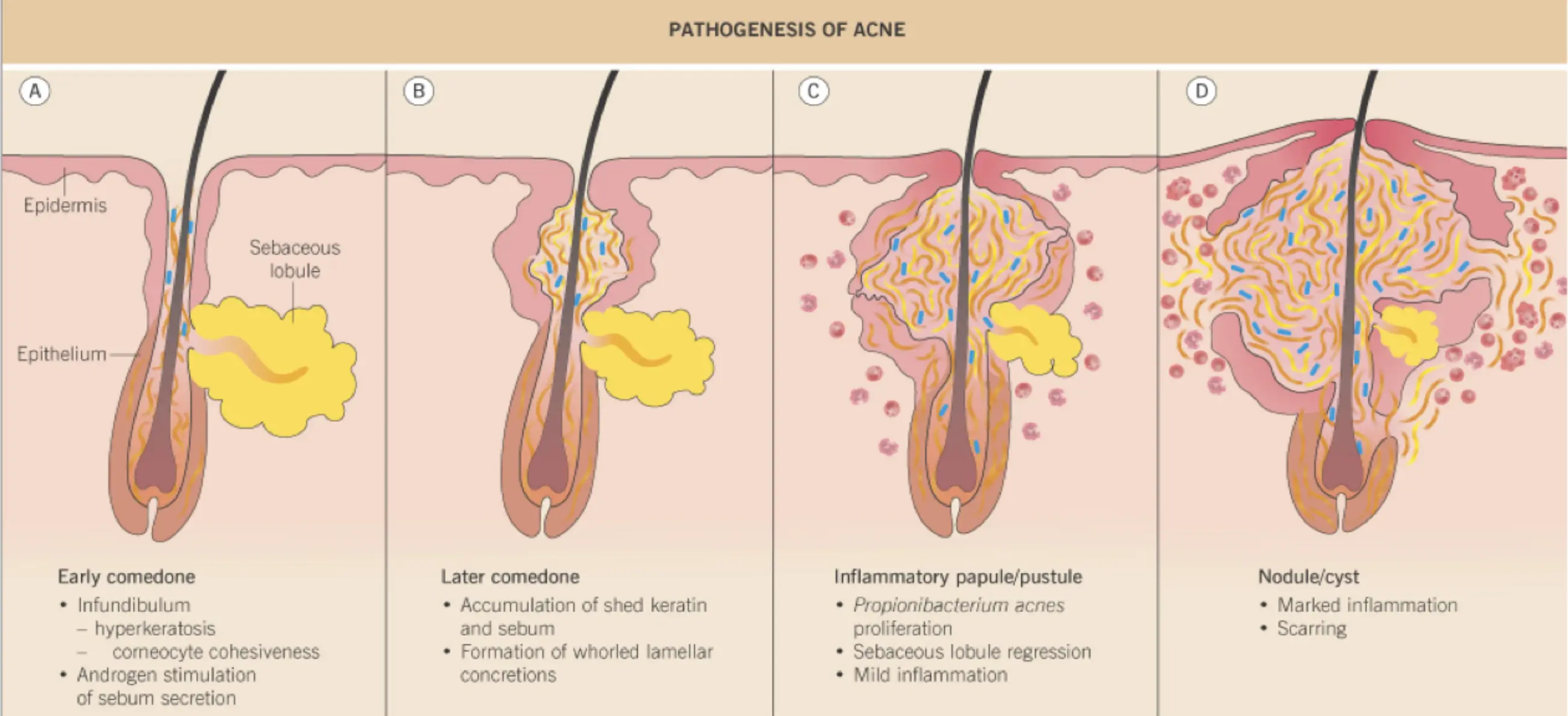
Pathogenesis of acne?
- A
- Epidermis
- Epithelium
- Sebaceous lobule
- Early comedone
- Infundibulum
- Hyperkeratosis
- Corneocyte cohesiveness
- Androgen stimulation
- Of sebum secretion
- B
- Later comedone
- Accumulation of shed keratin
- And sebum
- Formation of whorled lamellar
- Concretions
- Later comedone
- C
- Inflammatory papule/pustule
- Propionibacterium acnes
- Proliferation
- Sebaceous lobule regression
- Mild inflammation
- Inflammatory papule/pustule
- D
- Nodule/c
- Marked
- Scarring
- Nodule/c
Hyperproliferation at Hair Follicle “Hyperkeratosis” ↑ sebum production Proliferation at propionibacterium ↑ Inflammatory response
What are the Stages of acne?
- Normal follicle.
- Open comedone (blackhead).
- Closed comedone (whitehead).
- Papule.
- Pustule.
What is the possible cause of acne? Mostly Genetic Aspect. ⬆️ Androgen production
How to manage this patient? / Most appropriate treatment:
- Full history
- Examination
- Education
- Sunscreens (Sun block)
- Avoidance of aggravating factors.
- Mild: Topical keratolytic (Topical Tretinoin)
- Moderate: Oral antibiotic (doxycycline)
- Topical Antibiotic: clindamycin
- Laser and light therapy
- Severe: Oral Isotretinoin (indicated for Nodulocystic Acne, or when not responding to topical treatments)
- Emollient
Isotretinoin Specifics:
 Mechanism: works on all pathogenesis of acne
Mechanism: works on all pathogenesis of acne
Indication:
- Severe acne (nodules scars) + failure of topical treatment + psychosocial.
Pre-prescription tests for Oral Isotretinoin:
- Lipid profile
- LFT (Liver Function Test)
- RFT (Renal Function Test)
Side Effects / Complications:
- Dryness (Xerosis is the most common)
- Mood changes (Depression)
- Increased intracranial pressure (pseudo cerebri)
- Teratogenicity
- Epistaxis
- Photosensitivity
- Contraindicated to give with doxycycline
Specific Notes on Lesions:
- Lesion pointed by the arrow (example from image): Open comedon
- Diseases with pustule as primary lesion:
- Acne vulgaris
- Folliculitis

Folliculitis
What is the Diagnosis?
- Folliculitis
Mention two diseases with pustule as primary lesion?
- Acne vulgaris
- Folliculitis