Management of Chronic CAD: stable angina
Non- pharmacological
- Address modifiable risk factors (lipid lowering, cigarette cessation)
- Strict diabetic control
- Optimum blood pressure control
- Correct illnesses that can precipitate or exacerbate angina (anaemia, infection, thyroid disease)
- Encouraged Regular exercise
Important Point
- Blood Pressure : < 140/90 mmHg (Diabetes: BP 130/80 mmHg)
- Serum cholesterol < 4.0 mmol/L
- HDL > than 1 mmol/L
- LDL < than 2 mmol/L
Pharmacological therapy
A- Vasodilator – GTN - Venodilators x
(Glyceryl Trinitrate 0.3-1mg sublingual). Isosorbide mononitrate – 10-60mg orally bd
Action
- Venodilation: ↓ cardiac preload, decreasing wall stress and O2 demand
- Relieving angina and improving exercise tolerance
- does not affect mortality.
Contraindicated:
sildenafil (Viagra), RT ventricular Infarction = and severe hypotension; they result in vasodilation
Nitrates are contraindicated in case of hypotension, myocardial infarction of the right ventricle, and recent use of PDE-5 inhibitors like Sildenafil, because in these situations nitrates can cause really severe hypotension.
B- Beta Blocker : 1st line
- Atenolol (Tenormin) 25-100mg daily
- Bisoprolol (Concor) 2.5-10mg/day
Action
- ↓ heart rate
- ↓ BP
- ↓ myocardial O2 demand (!! heart failure)
- β-blockers reduce both morbidity and mortality. (Post-MI & HF)
C/I: Prinzmetal angina, bradycardia, cardiogenic shock, and cocaine-related ACS.
Calcium channel blockers (CCBs)
- Second-line therapy
- Improve myocardial oxygen supply by ↓ coronary vascular resistance, myocardial demand is ↓ by a ↓ in myocardial contractility.
- Verapamil and Diltiazem Inhibit cardiac conductive tissue.
- Contraindicated: Bradycardia, H block, LVF
- Do not use short-acting dihydropyridines, which increase mortality rates in patients with ACS of CCBs; verapamil; diltiazem use dipines
- Long-acting agents are safe and effective in chronic stable angina
Do not combine β- blockers with non-dihydropyridine calcium antagonists).
If these fail to control symptoms or are not tolerated, trial other agents.* Ranolazine: SDL Z will use
Primary and Secondary Prevention
- Primary Prevention
- prevention of atherosclerotic disease process. (Atorvastatin 20 mg CL)
- Aspirin: Not recommend in primary prevention !!! Z
- Secondary Prevention
- treatment of atherosclerosis (its complication) . Atorvastatin 80 mg
Read SDL: QRISK®3 risk assessment tool https://qrisk.org/ - Age, Sex, Ethnicity, Smoking/DM Status - CKD, Angina H attack in 1st degree relative, RA, Migraines, HTN, SLE, Antipsychotics, Steroid tablets, viagra, steroids. CL/HDL ration, Systolic BP - Standard deviation of recent systolic BP reading - Height/Weight
Secondary Prevention of IHD
Medications that decrease morbidity and mortality
-
Aspirin 75mg daily – All patient unless contraindications. S/E GI bleeding
-
ACE inhibitors – used if hypertension, heart failure.
-
Statins (Lipitor ): elderly ≥ 75 y. & left ventricular (LV) dysfunction (ejection fraction [EF] <40%)
Atorvastatin 20 mg is recommended for the primary prevention of cardiovascular disease in people with a 10-year risk of cardiovascular disease of 10% or higher. In patients with established cardiovascular disease, NICE recommends atorvastatin 80 mg, unless there are potential drug interactions, a high risk of adverse effects or a different patient preference.
Algorithm for Management of Patient’s with Stable Angina
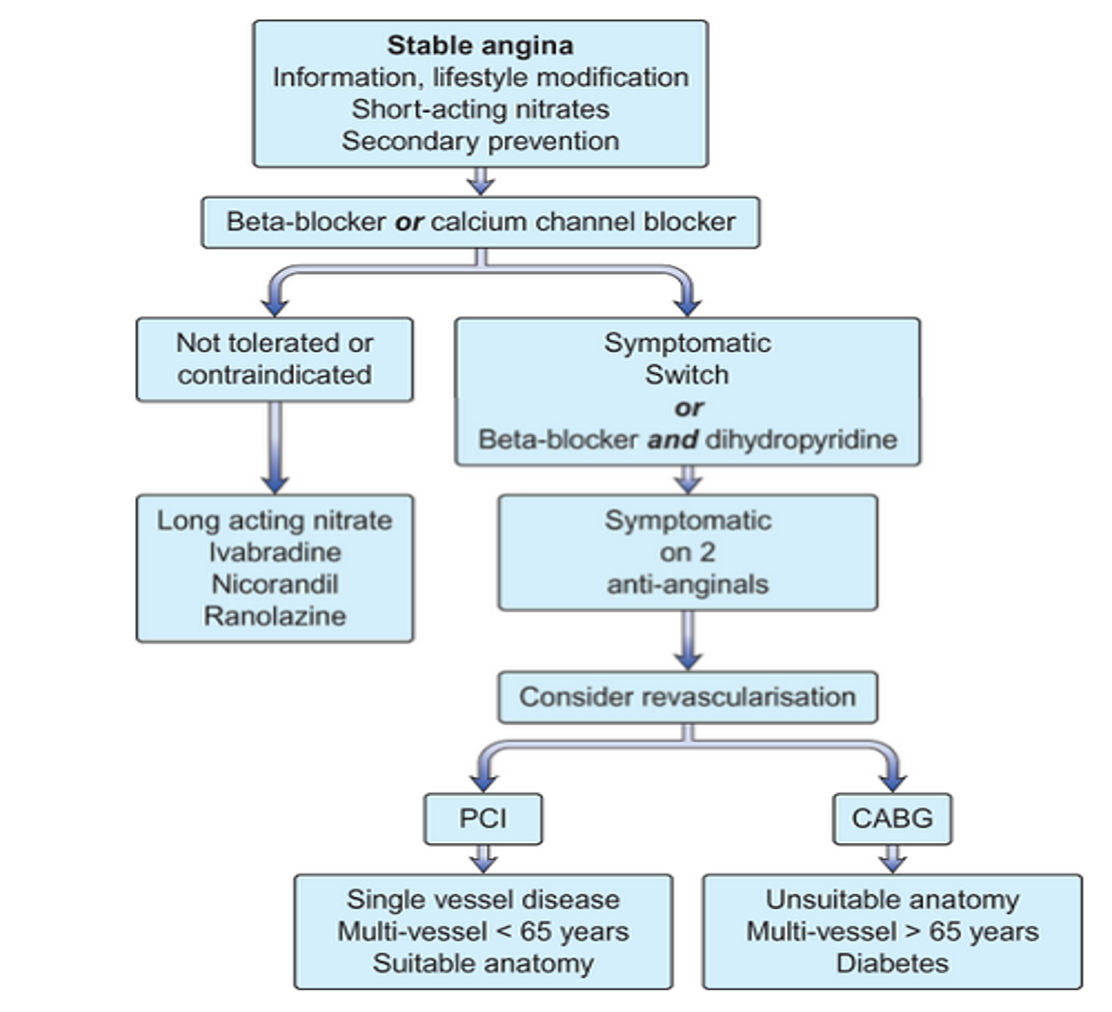 SDL revise Kumar 1083 CC
FIRST MEDICAL THEN ADD BB THEN PCI
SDL revise Kumar 1083 CC
FIRST MEDICAL THEN ADD BB THEN PCI