History & Examination of Hernias
Omar Alaidaroos
ILOs
Demonstrate ability to perform:
- Proper history taking.
- Physical examination correctly.
History
-
Name:
-
Age:
- Young Age—indirect
- Old Age—direct
-
Sex:
- Most common hernia in females—indirect inguinal hernia
- Most common hernia in males—indirect
- Femoral hernia most common among—females
- Direct hernia never occurs in females and children
-
Occupation: Most common in strenuous labor
-
Presenting Complaints
- I. About the hernia
- II. Due to hernia (Complications)
- III. Precipitating factors
About the Hernia
- Duration, When first noticed?
- Onset: Suddenly/gradually, How noticed?
- Site of start:
- From groin to scrotum (hernia)
- From scrotum to groin (hydrocele and varicocele)
- Does it disappear completely, does it become smaller/ larger?
- Aggravating factors:
- On straining
- On standing
- On coughing
- Relieving factors:
- By lying down
- Manually by himself
- Associated with pain: Usually painless, Any other lump/ swelling
Pain in inguinal hernia is usually in the region of the umbilicus due to drag in the root of mesentery as bowel enters the sac
Complications
- Irreducibility:
- i. Crowding of the contents
- ii. Adhesion between sac and contents
- History of potential complications:
- Abdominal pain
- Vomiting
- Irreducibility/ painful lump
- Obstruction: Four cardinal features
- Strangulation: (Obstruction + irreducibility + Arrest of blood supply)
- i. Colicky abdominal pain if continues and becomes gangrenous pain disappears
- ii. Sudden increase in size of hernia; becomes tense and tender.

III. History of Precipitating Factors
- Chronic bronchitis/asthma/TB
- Difficulty in micturition
- Difficulty in defecation
- Weight lifting
Past History
- History of diabetes mellitus/Hypertension/Ischemic heart disease/Bronchial asthma/Tuberculosis
- History of previous surgery
History of appendicectomy: Ilioinguinal or iliohypogastric nerve if damaged by grid iron incision or during keeping the drain; Direct Hernia Occurs
If ilioinguinal nerve is cut in the inguinal canal, direct hernia never occurs Because the nerve supplies the abdominal muscles before entering the canal
Family History
History of connective tissue disorders in family.
Personal History
- History of Smoking:
- Smoking leads to chronic bronchitis
- Collagen deficiency occurs in smokers.
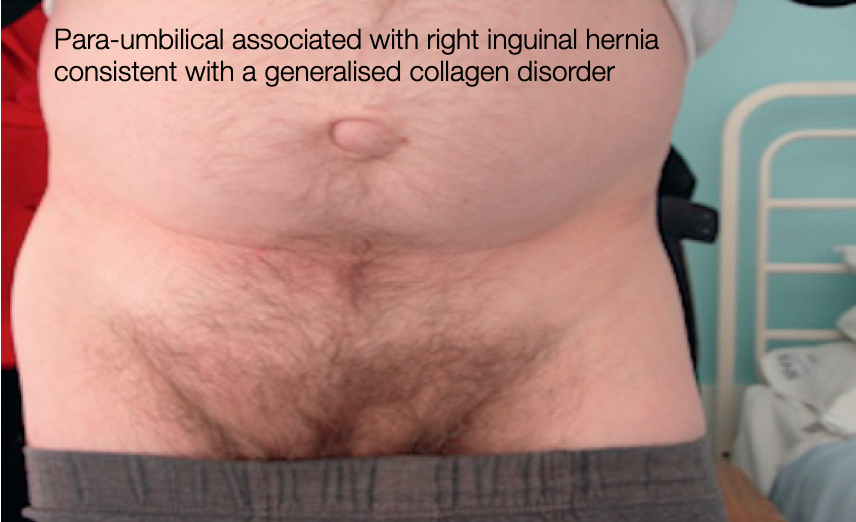
- Para-umbilical associated with right inguinal hernia consistent with a generalised collagen disorder
ِExamination
- Introduce yourself
- Explain & seek permission
- Exposure mid chest to mid thigh
- Start examination- patient in standing then supine position
- Groin swellings- also examine patient in standing
- Always examine both groins
General Examination
Abdomen
- Mass abdomen
- Malgaigne’s bulgings
- Ascites
Malgaigne’s bulging:
- Oval, longitudinal, bilateral bulging produced on straining, in inguinal region or above it; and are parallel to medial half of inguinal ligament
- Present in direct hernia
- Indicates poor muscle tone
- Signifies hernioplasty is the treatment
LOCAL EXAMINATION
Inspection: patient in standing position
- Groin swellings:
- Does it extend down to scrotum?—Inguinoscrotal
- Is testis separate from swelling?
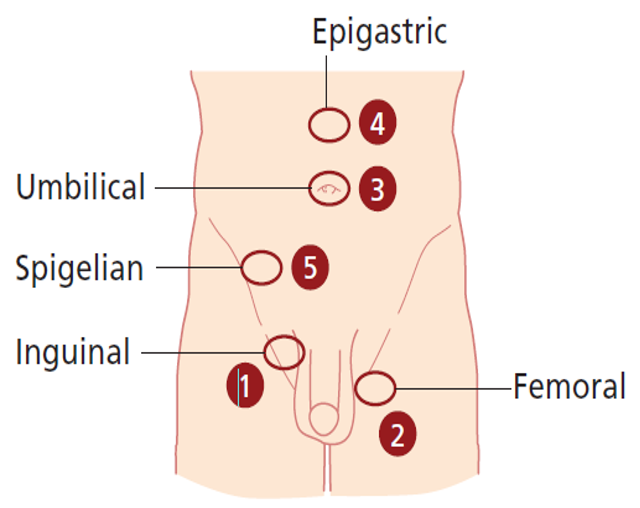
- Site:
- Femoral—below and lateral to pubic tubercle
- Inguinal—above and medial to pubic tubercle
- Size
- Shape:
- Pyriform—indirect
- Hemispherical—direct
- Retort—femoral
- Extent
- Surface
- Skin over the swelling
- Visible peristalsis
- Cough impulse
- Draining lymph nodes
- Penis
- Urethral meatus
- Opposite scrotum

Palpation
- Temperature
- Tenderness
- Site
- Size
- Shape
- Extent
- Surface
- Skin over
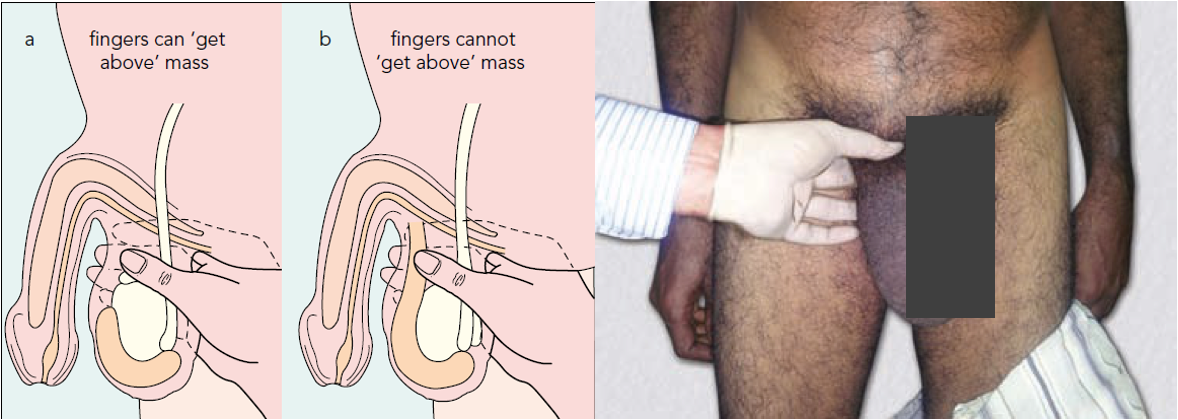
- Get above the swelling: (hernia vs scrotal swelling)
- Is testis separate from swelling?
- Get above the swelling is a classical feature of hydrocele
- Cough impulse
- Consistency:
- Soft elastic—intestine
- Doughy granular—omentum
- Reducibility:
- a. Intestine: Last part is easy to reduce; Initial part is difficult to reduce; gets reduced with gurgling sound.
- b. Omentum: First part easy to reduce, last part is difficult because omentum adheres to fundus of sac.
- Direction of reduction of hernia
- Direct hernia—directly backwards
- Indirect—goes upwards, backwards and laterally
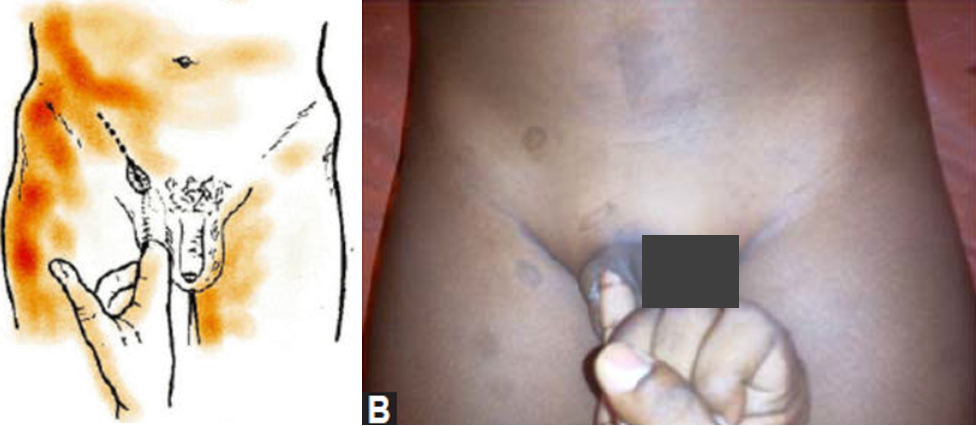
- Ring invagination test
- Only test in hernia; done in lying position.
- Prerequisite:
- ––Swelling should be reducible
- ––Lax of skin should be there for invaginating (so this test could not be done in females)
- Procedure
- Reduce the swelling.
- For right side, invaginate with right little finger into the superficial ring.
- Rotate the little finger medially so that the pulp faces medially.
- Note the direction of entry and site of impulse.
- Look for:
- Strength of superficial ring: Normal ring admits only the tip
- Site of impulse:
- Pulp—direct
- Tip—indirect
- Deep ring occlusion test: (only after complete reduction of hernia)
- After reducing the contents, patient in standing position, occlude the deep ring with thumb. Ask the patient to cough.
- If swelling appears - Direct
- Does not appear – Indirect
- Fallacy of deep ring occlusion test (When will you get the swelling even though it is an indirect hernia by deep ring occlusion test?)
- A. Pantaloon hernia
- B. Wide deep ring (Occlude in such cases with index and middle finger together)
Ring invagination test
Deep ring occlusion test

Percussion
- Enterocele: Resonant
- Omentum: Dull
Auscultation
Peristaltic sounds occasionally heard.
Others
- Testis: ‘Traction Test’ to find whether the inguinal swelling is an Encysted Hydrocele of Cord.
- Epididymis.
- Penis:
- Phimosis
- Penile strictures
- Pinhole meatus
- Regional nodes.
- Opposite groin.
Per-rectal Examination
To Rule out:
- Benign Prostate hypertrophy—micturition difficulty
- Malignant obstruction
- Chronic fissure—constipation