usually presents between the ages of 35 and 55 years with hypertension, renal failure or hematuria, or following the discovery of bilaterally enlarged kidneys.
The diagnosis is readily made at ultrasound, as well as on CT.
Imaging
Ultrasound
-
In adults: Enlarged kidneys with multiple cysts bilaterally of varying sizes (anechoic masses)
-
In children: evidence of cysts in combination with a family history positive of ADPKD
-
Hepatic, pancreatic, and/or splenic cysts may be visible.
 Ultrasound kidney (longitudinal view;
note that the poles of the kidney extend beyond this view)
Multiple, sharply demarcated anechoic lesions have replaced the majority of the renal parenchyma. Part of the renal sinus is still visible.
These findings are consistent with polycystic kidney disease.
Ultrasound kidney (longitudinal view;
note that the poles of the kidney extend beyond this view)
Multiple, sharply demarcated anechoic lesions have replaced the majority of the renal parenchyma. Part of the renal sinus is still visible.
These findings are consistent with polycystic kidney disease.
CT
Not the method of choice Should only be used if ultrasound findings are unclear (due to the radiation exposure of CT)
Shows
- Multiple cysts: usually hypodense, well-demarcated, not septated, and thin-walled
- Bilateral enlargement of the kidneys
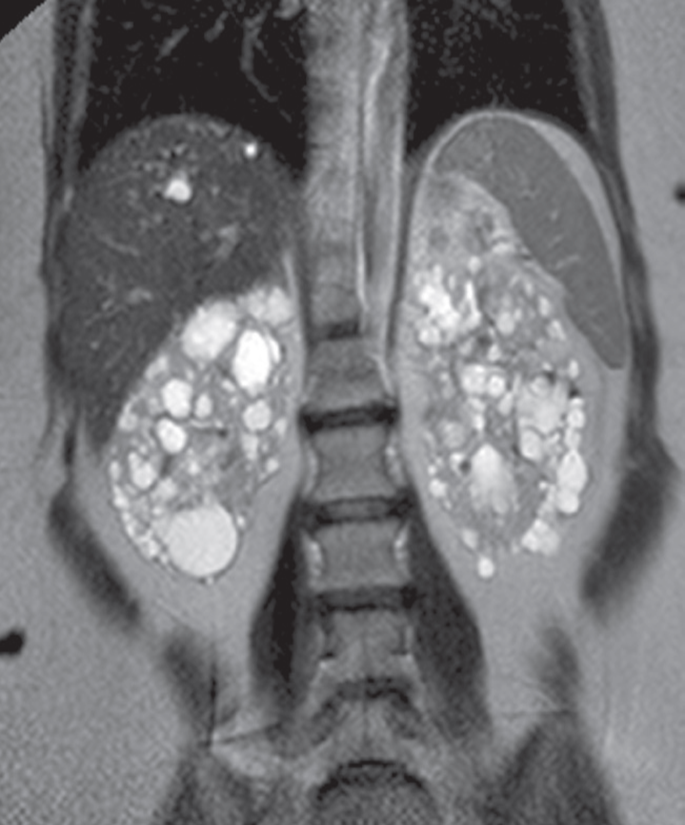
Coronal T2-weighted MRI
demonstrating multiple bilateral renal cysts as well as a few cysts in the liver.
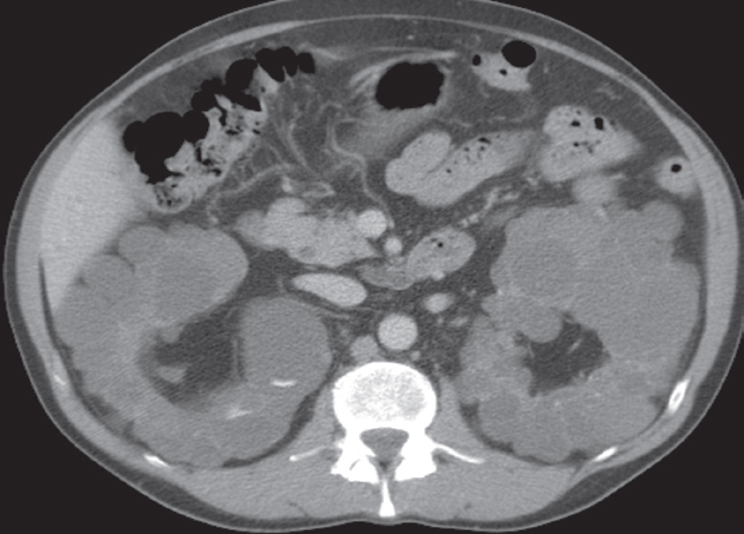
Advanced polycystic disease in adults. (a) CT scan,
taken after intravenous contrast enhancement, showing that both kidneys are greatly enlarged and almost entirely replaced by cysts of variable size.
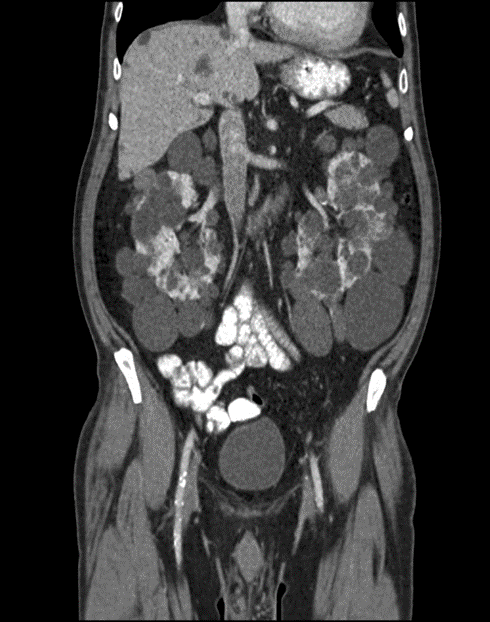
CT abdomen (with contrast; coronal plane) Both kidneys are markedly enlarged and feature multiple round-to-ovoid, hypodense lesions of various sizes compatible with cysts. Some smaller cysts are present in the liver. Contrast-enhanced renal parenchyma is seen between the cysts.
The CT features are consistent with autosomal dominant polycystic kidney disease (ADPKD).
Thus patient had a transplant.
What is the diagnosis
